
Abstract
Abstract
Objectives:
Symptomatic angiomyolipoma (AML) and asymptomatic AML larger than 4 cm in size are usually treated with nephron-sparing surgery or transarterial embolization. We used radiofrequency ablation to treat the vascular pedicle of exophytic AML with low R.E.N.A.L. nephrometry score and investigated its feasibility for hilar off-clamping nephron-sparing surgery.
Methods:
Contrast-enhanced computed tomography (CT) showed enhanced, well-defined lipomatous tumors with a maximum diameter of 4–8 cm in the kidney of 15 patients. Results indicated that the exophytic tumors featured in the enlarged tumor vasculatures extended into the parenchyma of the involved kidney. The patients underwent radiofrequency ablation by using a Cool-tip™ probe placed into the root of the AML mass from different directions under laparoscopic ultrasonography guidance. After sealing the vascular pedicle of the tumor, the bloodless tumors were resected en bloc without renal hilar clamping or suturing the resection defect of the kidney.
Results:
All patients underwent the procedure smoothly, and no perioperative complications occurred. The contrast-enhanced CT scan showed small defects in the contrast-enhanced renal parenchyma at third month after the procedure, and the decrease in function of the treated kidneys was <10% during the 12-month follow-up.
Conclusions:
Our initial experience suggests that sealing the tumor vessels by radiofrequency ablation based on the tumor vasculature features of a renal mass is an alternative to hilar clamping in laparoscopic nephron-sparing surgery. Laparoscopic radiofrequency ablation and tumor excision are a definitive and safe minimally invasive procedure that allows the successful removal of exophytic sporadic AML mass with low R.E.N.A.L. nephrometry score.
Introduction
S
These lesions are benign. Thus, evidence suggests that the majority of these lesions can be safely followed up without treatment. However, an increasing wealth of available information suggests that the prophylactic treatment of some individuals with AMLs is indicated to prevent complications, such as dangerous retroperitoneal hemorrhage; furthermore, pregnant women have a high risk of AML rupture. 1
Tumor diameter is a significant parameter in choosing the correct treatment. 2 In such cases, treatment with radiological interventional techniques with subselective particle embolization has superseded surgical treatment in most cases. The arterial embolization of AML is often considered the first line of treatment for patients with renal AML with few procedural morbidity. 2 Even in emergency cases with catastrophic rupture, prompt embolization may save the patient with the additional benefit of renal salvage. Embolism is palliative with a slow regression of the tumor mass in the follow-up. However, regrowth and repeated hemorrhage or the required repeated procedure after arterial embolization remains a concern. 2 The surgical excision of the tumor is preferable for most patients and their surgeons.
In this article, we present a novel technique for treating exophytic renal AML by the radiofrequency ablation (RFA) and surgical excision of the tumor mass under laparoscopy and intraoperative ultrasonography monitoring. This technique is designed on the basis of the imaging findings of the tumor vasculature features in the exophytic renal AMLs with low R.E.N.A.L. nephrometry score.
Patients and Methods
Following the diagnosis, 15 patients who were being considered for RFA were enrolled in an IRB-approved prospective pilot study (Supplementary Fig. 1. Supplementary data are available online at www.liebertpub.com/lap). The patients were aged 22–59 years old. Contrast-enhanced computed tomography (CT) showed enhanced, well-defined lipomatous tumors with a maximum diameter of 4–8 cm in the involved kidneys. All cases had one point for the E domain of the R.E.N.A.L. nephrometry score, which is used to describe the exophytic or endophytic property of the mass. 3 A diagnosis of exophytic AML in the kidney was usually made by contrast-enhanced CT. As shown in the diagram (Figs. 1A and 2A, B), the tumors located at the renal parenchyma resemble the mushroom-soil mode, such that the major vascular pedicles of the tumoral body are rooted and extended directly into the renal parenchyma similar to the stem of a mushroom. Our technique was designed on the basis of this salient feature of exophytic AMLs of the kidney (Figs. 1B and 2C, D).

Diagrammatic description of the principle of designing the surgical procedure.
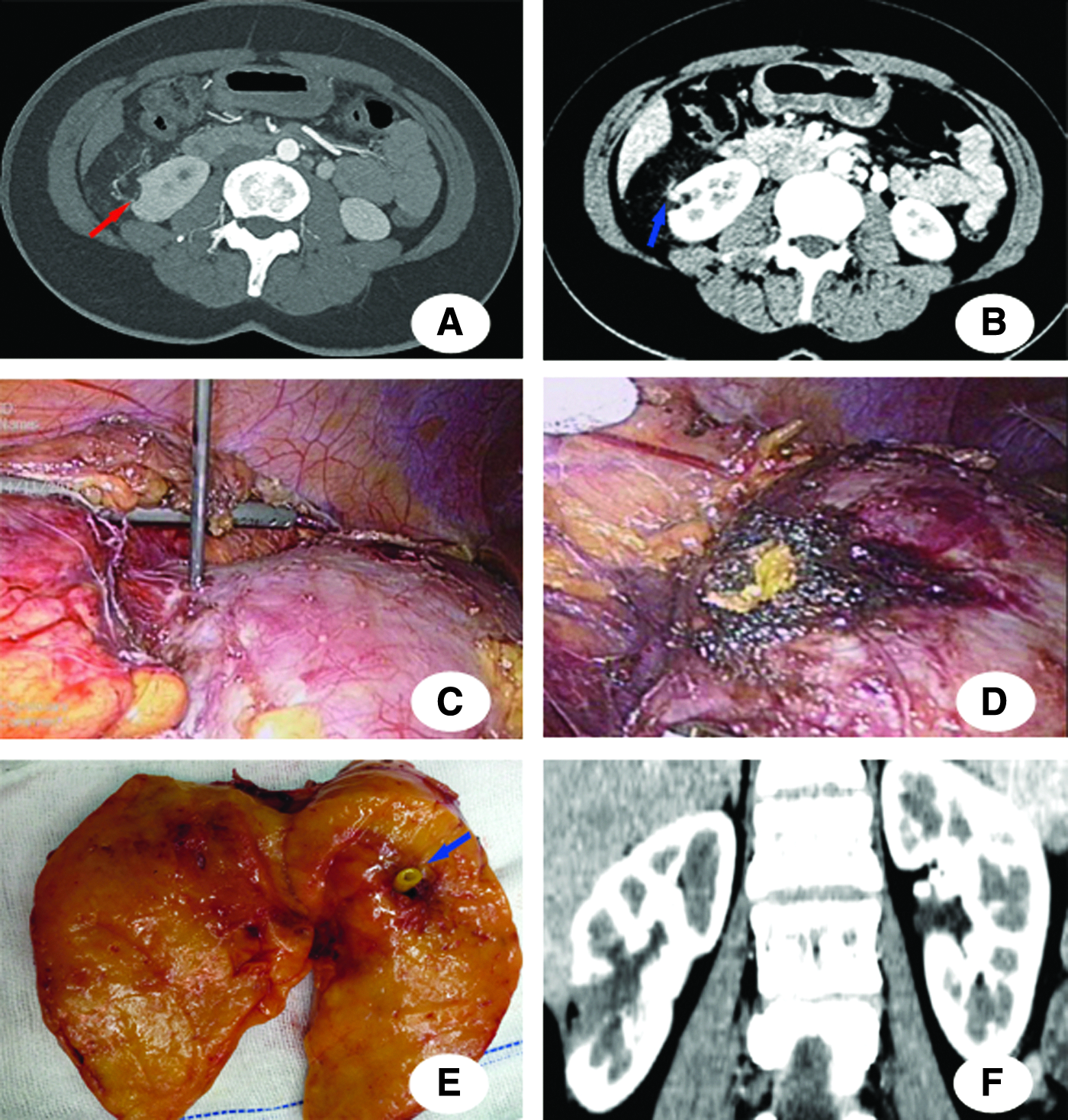
Vasculature features of the renal tumor, surgical procedure, and clinical outcome: supplying artery (
The procedure was performed by the transperitoneal laparoscopic approach as follows. The patients were secured in a 70° flank position on the operation table. The 10 mm camera port was placed 5 cm around the umbilicus. A 5 mm assist port and another 12 mm instrument port were then placed in a triangular manner with three ports. Toldt's line was incised, and the colon was mobilized medially to expose Gerota's fascia. Gerota's fascia was opened to the renal capsule near the tumor to expose the entire tumor mass and its base on the kidney (Fig. 2C). After the intraoperative procedure, a Flex Focus 800 laparoscopic ultrasonic probe (BK Medical, Inc., Peabody, MA) was used to evaluate the depth of the tumors infiltrating the renal parenchyma. The radiofrequency needle was inserted by penetrating the abdominal wall into the renal parenchyma at ∼0.5 cm to the root of the tumor under the direct vision of laparoscopic monitoring and laparoscopic ultrasonographic guidance during operations.
RFA was performed by the Covidien Cool-tip™ RFA system (Covidien, Inc., Mansfield, MA), which consists of a generator that supplied up to 200 W of power connected to a 15-gauge Cool-tip RFA single electrode.
To ablate the major vascular pedicle of the AML, the initial power was set at ablation power upon the electronic resistance of the targeted tissue for 6–12 minutes according to the protocol provided by the manufacturer, thereby resulting in an end temperature of the targeted zone above 65°C. Ablation with three or four needles was performed from different directions to the root of the AML mass located at the involved kidneys to seal the vasculature pedicle characterized by contrast-enhanced CT (Figs. 1B and 2C). The bloodless tumor masses were excised by cold scissors or a monopolar electrohook. The tumor samples were retrieved from the abdomen by harvesting into the sample bag.
The intraperitoneal draining tube was placed near the surgical site, and the patients returned to the surgical ward. Routine care was given, and a follow-up was conducted by CT at 3 months, 6 months, and 1 year after the operation and annually thereafter.
The variables studied were tumor size, technical success, operative time, treatment safety, blood loss, hemorrhage-free surgical resection, hospital stay, renal function alterations, and kidney consistency. The renal function, hemoglobin levels, and perioperative complications were recorded before and after the operation. The patients were followed up for 12 months. Furthermore, we reviewed the functional and oncologic outcomes.
Results
The cool-tip radiofrequency ablation under a laparoscope was successfully performed in the 15 patients. For all patients, laparoscopic partial nephrectomy was performed successfully without renal hilar clamping and any suturing. The patients recovered evenly without any complications related to the procedure after the surgery and were discharged on the third day after the operation. During the 6- to 12-month follow-up period, no function of the treated kidneys decreased at 12 months. The patients did not have any complications or AML-related symptoms developed.
The operation was successful in all cases and had an operative time of 65–125 minutes and estimated blood loss of 20–65 mL. The tumor was completely removed (100%) with the absence of enhancement in the tumor sites, and no AML recurrence was observed by contrast-enhanced CT scan during the 12-month follow-up period (Fig. 2E, F). The estimated glomerular filtration rate (eGFR) in patients was re-evaluated at 3 months after the operation and indicated no significant alteration of renal function compared with preoperative eGFR (Table 1).
AML, angiomyolipoma; eGFR, estimated glomerular filtration rate.
Discussion
AMLs are benign renal neoplasms with a propensity to bleed among patients with tumors exceeding 4 cm in diameter, but can be effectively be treated with transarterial embolization to arrest or prevent hemorrhage. The removal of tumors appeals to patients and surgeons. Current imaging technology allows the detailed delineation of the anatomy and vasculature of the renal mass and enables the application of the anatomic feature scoring system to accurately describe the tumor and design precise patient-specific surgical plans. 4
The confident identification of a lesion as an AML is important because its benign nature obviates the need for surgery in most cases. The presence of fat is paramount in the confirmatory identification and characterization of these lesions. Although fat-rich AMLs are easy to diagnose, some lesions are fat poor and require novel imaging techniques. Renal AML arising from the kidney shows characteristic parenchymal defects on contrast-enhanced CT. 5 A defect in the renal parenchyma should be present at the origin of the AML, whereas a perirenal liposarcoma is more likely to displace and compress the kidney. In addition, the renal AML usually contains enlarged vessels.
The ischemia time, tumor size, and endophytic/exophytic properties of a localized renal mass are the most important determinants of renal parenchymal volume loss after nephron-sparing surgery. 6 From a practical perspective, the most technically relevant surgically modifiable factor that affects remnant function after partial nephrectomy is the duration or extent of ischemia. The renal hilar or main artery clamping results in the greatest renal ischemic insult, which can be significantly reduced by the early unclamping of the main renal artery, with selective renal segmental artery clamping or super-selective renal tumor tertiary or quaternary artery branch arteriole clamping techniques.7,8 Although the selective clamping technique is primarily used in minimally invasive partial nephrectomy, Nohara et al. 9 found that a segmental renal artery could be isolated in only half of the cases during open partial nephrectomy. Selective arterial clamping may not be feasible in certain instances such as dense or adherent perirenal fat or short segmental arteries. Therefore, the unclamping techniques in renal surgery should be extensively explored and developed in practice. The accessibility of medical imaging has changed the pattern of the diagnosis, and some unique anatomic characters of the renal mass had been meticulously identified and evaluated.
We report our initial experience on the removal AML mass by RFA combined with surgical resection. The tumoral vessel extending into the renal cortex could be detected in thin-section contrast-enhanced CT, and the parenchymal defect was commonly seen in renal AML.10,11 The vascular characteristic of exophytic AML was featured by contrast-enhanced CT, and the major vascular pedicle is positioned in the center of the root and into the renal parenchyma. The vascular pedicle was defined as the feeding vessel of the AMLs. 10 The blood supply of renal AMLs is frequently bizarre and torturous. 11 Generally, the tumor may recruit from a variety of surrounding vessels, including renal, adrenal, urethral, gonadal, phrenic, and lumbar arteries. These features account for the high frequency of aneurysms detected within AMLs and for the high incidence of hemorrhage from these lesions. 12 However, the high-definition imaging technology of dual-source CT has revealed that the renal parenchymal vascular pedicle is one of the features that differentiate the exophytic renal AML from perirenal liposarcoma.13,14 The renal tumor-supplying arteries seen on CT angiography were defined as the feeding branches from the renal segmental arteries directly entering the tumor. These new attributes could be utilized to design a novel approach to treat lesions by combination with surgical energy devices such that the thermal energy precisely seals the vasculature of the renal tumors toward perfect hemostasis in nephron-sparing surgery. The radiofrequency energy may facilitate the sealing of major vessels entering into the vascular pedicle toward the definitely safe hemostasis to realize the bloodless resection of AML. The defect after removing the tumor can be closed with an intraparenchymal running suture or thrombin sealant; however, RFA obviates the need for parenchymal renorrhaphy suturing. The residual renal parenchyma suffers no warm ischemic injury for off-clamping of the renal hilar or suturing the renal parenchymal defect. Herein, we present a new approach to ablate the vascular pedicle of the exophytic AML to perform an off-clamping nephron-sparing surgery. This approach has not been reported in literature to date. Reyes et al. 15 used thermal ablation in low- or moderate-complexity lesions measured by the R.E.N.A.L. nephrometry scoring system. The evolving trend of partial nephrectomy is designed on the basis of anatomical features of the renal mass for nephron-sparing surgery.6,16 The R.E.N.A.L nephrometry score of the tumor considers the physical location in the kidney rather than the functional characters, such as tumor vasculature and renal parenchymal volume. Our technique integrated the features of location with the vasculature features of the renal mass.
The R.E.N.A.L. (radius, exophytic/endophytic properties of the tumor, nearness of tumor's deepest portion to the collecting system or sinus, anterior/posterior descriptor, and location relative to polar lines) nephrometry scoring system was introduced to objectively evaluate the renal mass anatomy and standardize academic reporting. Schmit et al. 17 used the R.E.N.A.L. nephrometry score to help predict the outcome and complications of the percutaneous ablation of renal masses. We adopted the R.E.N.A.L. nephrometry and PAUDA scores as the preoperative tools to evaluate the complexity of the procedures and included the AML cases with an E-score of one. A low R.E.N.A.L. nephrometry score implied that the parenchymal rim around the tumor was thick enough to place the ablation needle safely far from the renal collecting system and the major branch of the renal artery in the renal sinus. Although partial nephrectomy may be performed without any vascular clamping whatsoever when the tumor has favorable anatomical features (small size, exophytic lesion, and low nephrometry scores), tumor excision and renal reconstruction are performed unclamped. Previous studies revealed an increase in the estimated blood loss for this approach without an increase in the transfusion rates. 18 The moderate diameter of the renal mass in our series was larger than 4 cm with low R.E.N.A.L. nephrometry scores and removed without any increase in the estimated blood loss.
Compared with the other techniques to manage AML by RFA, numerous reports presented the routine method, such that the ablation needle was placed into the mass body of the AML guided by the CT or ultrasound to ablate the tumor without removing the tumor body after the procedure. CT scanning will be given at a specific interval for the follow-up. Some minor complications could occur, such as the bleeding of the tumor.19,20
Various approaches have been presented for off-clamping nephron-sparing surgery. 21 We started this new modality such that the ablated target tumor is based on the vascular features of the mass in the patients with renal AML, but we have not applied it on patients with renal malignant masses thus far. A precise ablation margin is difficult to achieve by radiofrequency for securing the resection of renal malignant lesions. To obtain the secure ablation boundary, neighboring renal parenchyma need to be ablated, which may injure the branches of renal segmental arteries or renal sinus tissues and decrease the preservable renal tissue by the unnecessary removal of healthy parenchyma. Therefore, we chose the AML mass with a low R.E.N.A.L. nephrometry score, particularly an E-score of less than two.
Compared with the series used by Wu et al., 22 the series used in the present study is the Habib 4 × RFA device, which coagulates a margin of normal parenchyma around the renal mass and allows the excision of the mass within a bloodless plane. However, the Habib 4 × RFA device cannot precisely manipulate the targeted blood vessels. The amount of renal parenchyma preserved was not indicated.
Although this study clearly demonstrates that this novel RFA technique improved the safety of the off-clamping renal surgery in cases with specific vasculature features and low R.E.N.A.L. nephrometry scores, the proposed method does not adapt for all renal AML without limitations, thereby limiting its use to manage renal AML. The surgical decision-making for renal AMLs remains overly subjective, but the imaging evaluation of renal AMLs is important to utilize this novel technique to manage renal AMLs. High-definition contrast-enhanced thin-section CT imaging is preferred in accurately characterizing the vascular features of the renal AML. Second, the lack of randomization with the conventional minimally invasive surgery with renal hilar clamping attenuates the robustness of the current study, which needs further randomized control trials to provide more evidence for this promising technique.
Conclusions
Our initial experience suggests that the laparoscopic RFA of feeding vasculature and tumor excision is the definitive, minimally invasive treatment alternative for achieving satisfactory hemorrhage control without ischemic/reperfusion injury. This treatment preserves renal functions and successfully removes exophytic sporadic AML mass with low R.E.N.A.L. nephrometry scores. We have demonstrated the feasibility of this novel approach to hilar off-clamping in laparoscopic nephron-sparing surgery for AML.
Footnotes
Acknowledgment
The authors thank Dr. Jingyi Yang from the Department of Radiology for providing the consultation on medical imaging.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.