
Abstract
Abstract
Background:
Single-port laparoscopy is a step forward toward nearly scar less surgery. Concern has been raised that single-incision laparoscopic surgery (SILS) is technically more challenging because of the lack of triangulation and the clashing of instruments. Robotic single-incision laparoscopic surgery (RSILS) in chopstick setting might overcome these problems. This study evaluated the outcome in time and errors of two tasks of the Fundamentals of Laparoscopic Surgery on a dry platform, in two settings: SILS versus RSILS.
Methods:
Nine experienced laparoscopic surgeons performed two tasks: peg transfer and a suturing task, on a standard box trainer. All participants practiced each task three times in both settings: SILS and a RSILS setting. The assessment scores (time and errors) were recorded.
Results:
For the first task of peg transfer, RSILS was significantly better in time (124 versus 230 seconds, P = .0004) and errors (0.80 errors versus 2.60 errors, P = .024) at the first run, compared to the SILS setting. At the third and final run, RSILS still proved to be significantly better in errors (0.10 errors versus 0.80 errors, P = .025) compared to the SILS group. RSILS was faster in the third run, but not significant (116 versus 157 seconds, P = .08). For the second task, a suturing task, only 3 participants of the SILS group were able to perform this task within the set time frame of 600 seconds. There was no significant difference in time in the three runs between SILS and RSILS for the 3 participants that fulfilled both tasks within the 600 seconds.
Conclusions:
This study shows that robotic single-port surgery seems easier, faster, and more precise to perform basis tasks of the Fundamentals of laparoscopic surgery. For the more complex task of suturing, only the single-port robotic setting enabled all participants to fulfill this task, within the set time frame.
Introduction
T
Despite the increasing interest in single-port surgery worldwide, the actual role of this novel approach in the field of minimally invasive surgery remains to be determined and its claimed advantages to be demonstrated. Randomized prospective, large-scaled clinical trials of the short- and long-term outcomes are essential to determine the precise effects of single-port laparoscopy. It is hypothesized that single-port surgery results into a benefit for patients in terms of less port-related complications, faster recovery time, less pain, and improved cosmetic results, as compared to conventional laparoscopic surgery. Possible disadvantages of single-incision laparoscopic surgery (SILS) could be increased wound infections and incisional hernia on the longer time. Randomized controlled trials have suggested that single-port surgery is at least comparable to standard laparoscopy.2–49
Single-port laparoscopy poses several challenges, specifically the handling of straight instruments in parallel with the laparoscope through a small single incision. This causes clashing of instruments and poses the surgeon the difficulty of laparoscopic surgery with lack of triangulation. Technical limitations of instrumentation in SILS have led to advancement in techniques and production of new instruments to overcome the limitations and therefore show the potential of SILS to outperform conventional laparoscopic surgery.
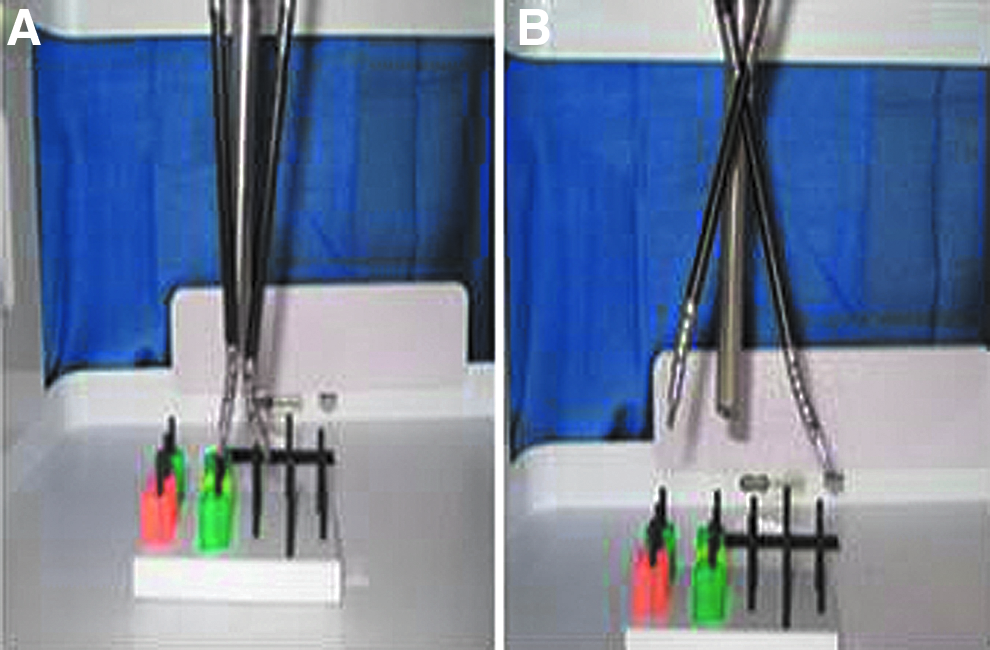
Robotic technology has been applied in single-port surgery with the aim to overcome the technical problems experienced with SILS.50–58 A surgical robot with wristed instruments and six degrees of freedom could overcome the limited maneuverability; but as with standard laparoscopy, the robotic arms do not work well when arranged coaxially through a single-port due to collision and malfunction. As demonstrated by Joseph et al., robotic single-incision laparoscopic surgery (RSILS) in chop stick setting might be the answer to the above mentioned technical problems (Fig. 1). By leveraging the superior range of motion and operator ergonomics of the da Vinci Surgical platform (Intuitive Surgical, Inc., Sunnyvale, CA) a chopstick arrangement of the robotic arms was created, which not only crosses the instruments internally at the abdominal wall but also overcomes the handicap of reversed handedness seen in conventional laparoscopy. This unique configuration was tested using standardized laparoscopic drills to objectively prove that the chopstick arrangement decreases instrument collision and malfunction and improves performance times and surgeon dexterity. 4 Additionally, surgical robots offer the advantage of tremor filtering and greater ergonomic and intuitive device manipulation. 59
When a new surgical technique is introduced, preferably it should not only be comparable to (or better than) existing techniques, but it should also be rather easy to learn. Therefore, an important aspect of a new surgical technique is whether it can be performed by other surgeons and how much effort is needed to master this new technique.
The aim of this study was to investigate the performance curve of experienced laparoscopic surgeons, with different experience level in robotic surgery, in single-port laparoscopy and robot-assisted single-port laparoscopy tasks.
Materials and Methods
Participants
Nine experienced laparoscopic surgeons from the departments of surgery, urology, cardiothoracic surgery, plastic surgery, and gynecology participated. Their experience with the robot varied from certified training experience on an exercise platform to weekly robotic surgeries. None of the surgeons had experience in single-port laparoscopy. Skills were tested at the operating theater of the Maastricht University Medical Center, The Netherlands (MUMC+). Informed consent was obtained by all participants.
Methods
Interview
One single question was asked after the performance of the tests in both settings: Which setting of single-port laparoscopy feels most comfortable, the SILS setting or the RSILS setting? The tasks in the RSILS setting were performed, using the da Vinci Si Surgical System™ (Intuitive Surgical, Inc., Sunnyvale, CA) with specialized single-site instrumentation (Intuitive Surgical), which included a single-site port, Crocodile Grasper, Needle driver, and Maryland Dissector. All of the single-site instruments were flexible and were not wristed.
For the SILS setting a D-Box trainer (Olympus) and a TriPort+™ device (Olympus, Advanced Surgical Concepts, Wicklow, Ireland) were used with conventional laparoscopic instruments (Olympus).
This study is exempt from IRB approval.
Tasks
Two tasks of the Fundamentals of Laparoscopic Surgery 13 curriculum were performed in three runs in both RSILS and SILS setting. There was a time limit of 600 seconds for each task. The task was stopped when the time limit of 600 seconds was reached. Half of the participants started with the tasks in the SILS setting, the other half of the participants started in the RSILS setting. The first task was peg transfer. Each of the six pegs was grasped with one of the Maryland dissectors, and transferred mid-air to the instrument in the other hand. Then the peg was placed on the other side of the pegboard. When all six pegs where transferred, the process was reversed and the pegs had to be placed back on the original side of the peg board with again a mid-air transfer to the other hand.
Time and errors were measured. Dropping of the pegs, clashing of instruments and instruments out of view were marked as errors. Dropping pegs outside the view of the scope were put into working field again by the observer, without stopping the time. The task was continued. The second task was a suturing task. The participants had to make a suture at a marked place; the suture had to be tied with three knots, the first two knots could be a slip tie knot. The goal of surgical knot tying was to allow the capacity of the knot to be tightened and remain tight. During this task, only time (in seconds) was scored. The strength of the knot was not scored. Procedures were monitored and scored by two observants. Figure 2 shows the setup of the tasks RSILS and SILS.
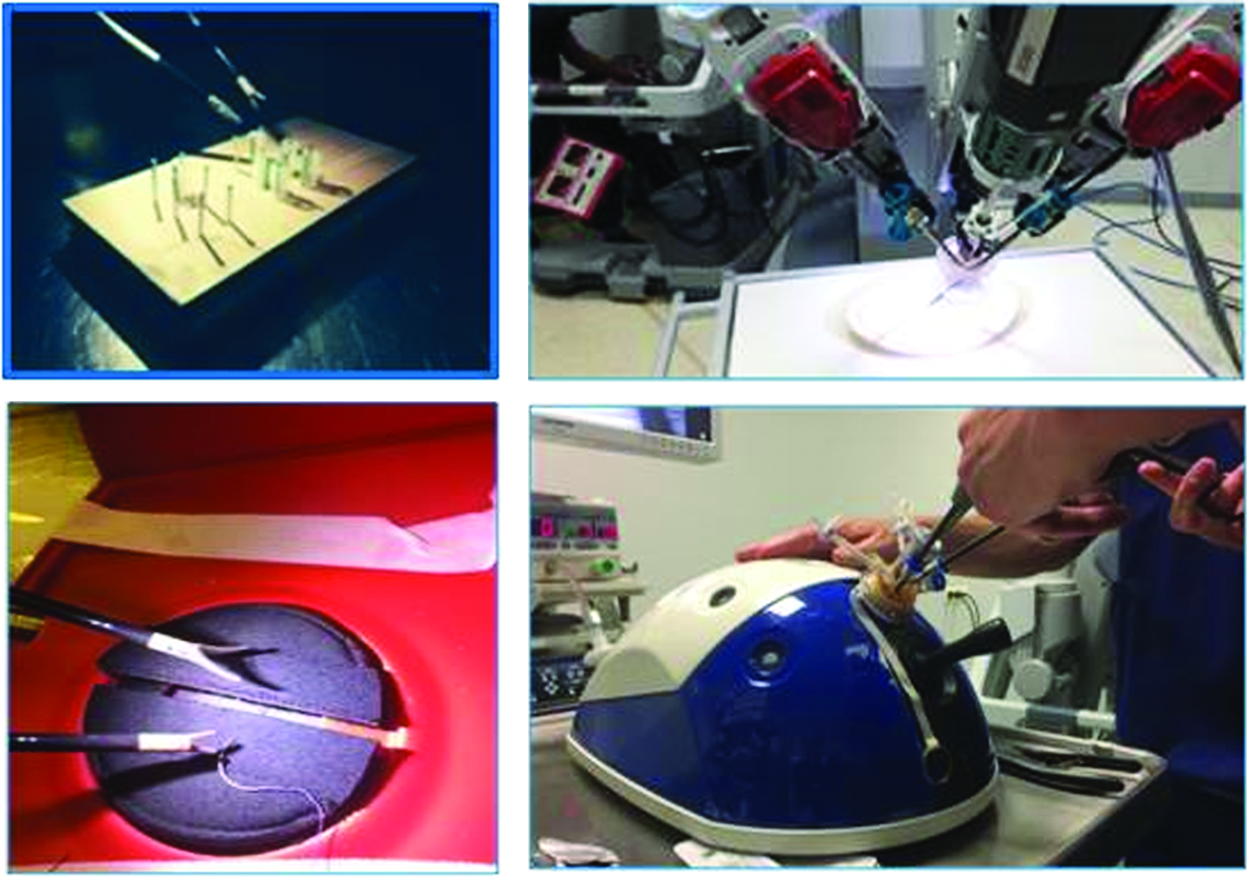
Setup tasks robotic single-incision laparoscopic surgery (RSILS) and single-incision laparoscopic surgery (SILS).
Statistical analysis
Differences in time and errors were analyzed with a paired T-test. The performance curve was measured by a Repeated Measures analysis of variance (ANOVA). The significance level was set at a P value less than .05. All statistics were performed with SPSS v22.0 (IBM, Armonk, NY). The repeated measures ANOVA outcome was adjusted for sphericity with the Maucley's test and if sphericity was violated, the Greenhouse Geisser statistical test was used to decrease the Type 1 error rate.
Results
Peg transfer
In run 1 the mean time was 231 seconds in the SILS setting versus 124 seconds in the RSILS setting (P = .004). In run 3 the mean time in SILS setting was 156 seconds compared to 116 seconds in the RSILS setting (P = .088). In run 1 the mean number of errors was 2.60 in the SILS group versus 0.80 errors in the RSILS group (P = .024).
In the final run 3 the mean number of errors was 0.80 in the SILS group versus 0.10 in the RSILS group (P = .025). Analyzing the performance curve in time with a Repeated Measures ANOVA, no significant learning curve can be found in time for both settings. A significant learning curve was found for errors in the RSILS group (P = .020). Table 1 and Figure 3 both present these results.
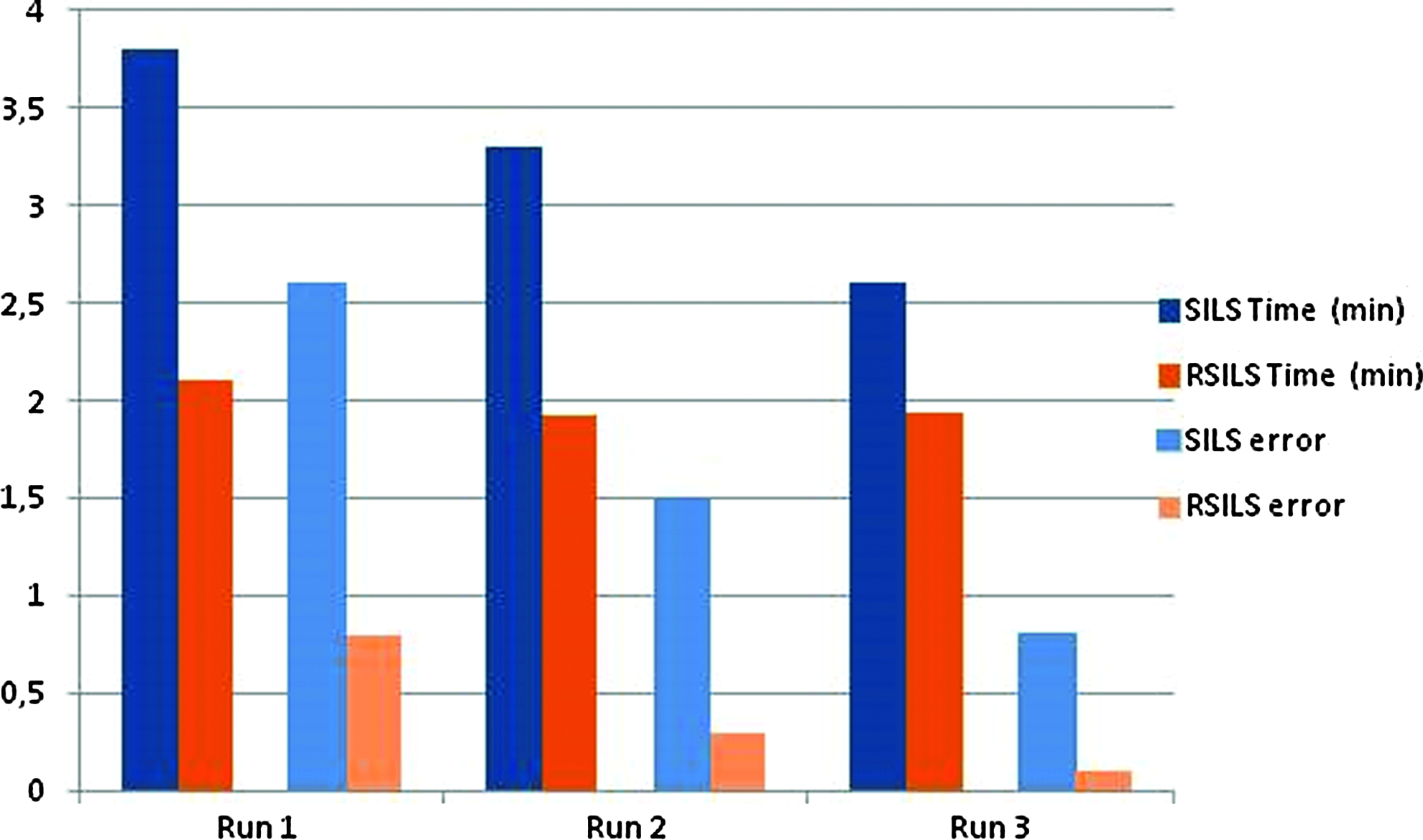
Peg transfer task: outcome and errors in three runs.
ANOVA, analysis of variance; CI, confidence interval; RSILS, robotic single-incision laparoscopic surgery; SILS, single-incision laparoscopic surgery.
Suturing task
In the SILS setting 5 participants were not able to perform the suturing task within the set time frame of 600 seconds. One participant did not complete the SILS suturing task. In the RSILS setting all participants succeeded in the suturing task within 600 seconds per task.
For the 3 participants who completed the suturing tasks in both settings, there was no significant difference in time in the three runs between SILS and RSILS. In the first 2 runs, robotic SILS was faster (RSILS run 1, 206 sec and run 2, 197 sec, versus SILS run 1, 308 and run 2, 286 sec), but not significantly. In the third run, SILS was faster (SILS run 3, 164 sec versus RSILS run 3, 183 seconds), also not significantly (Table 2). No further analyses in learning curve for this task were performed because of failure of 6 participants to complete the tasks.
RSILS, robotic single-incision laparoscopic surgery; SILS, single-incision laparoscopic surgery.
Questionnaire
All 10 participants preferred the RSILS setting for the performance of both tasks.
Discussion
In this study, we hypothesized that RSILS was easier to perform in time and more precise for two basic tasks of the Fundamentals of Laparoscopic surgery curriculum. For the three runs of peg transfer, indeed single-port surgery in a robotic setting showed to be less difficult (as illustrated by time needed to perform the task and errors made) compared to the conventional single-port setting). Suturing is a more complex task, which could only be performed by 3 out of the 10 participants in both settings within the predefined time.
The tasks were stopped when the time limit of 600 seconds was reached. The breaks between each run for both tasks was 10 minutes, or less, whenever the participants felt ready for it. All participants were able to make a suture with three knots in the RSILS setting in time, but only 3 participants completed this task in the SILS setting. This suggests that especially in more difficult tasks, which are even more challenging in single-port surgery due to the intrinsic impossibility of using a standard triangulation approach, the robotic approach has an advantage over conventional single-port laparoscopy. For the suturing task, quality of a knot is even more important than time. Knots have to be tight and remain tightened. The authors acknowledge that the quality (the strength) of the knot was not measured. Half of the participants started with the tasks in the SILS setting, the other half of the participants started in the RSILS setting. This was done to exclude the influence of practicing one task in one setting and having advantage for the performance of the same task in the other setting. The tasks used in this study are basic tasks from the Fundamentals of Laparoscopic Surgery61,62 curriculum. These were chosen as they are validated for discriminating proficiency level in laparoscopic surgery.
Overviewing the surgical experience of all participants, it has to be noticed that they are all well-experienced laparoscopic surgeons, with a variable experience in robotic surgery. None of the participants had experience with single-port laparoscopy. Since single-port laparoscopy is the topic of this study, the authors concluded that all surgeons were novices in single-port laparoscopy and therefore their learning curves could be compared.
As far as the authors know, there is no previous literature comparing robotic with laparoscopic single-port surgery on a dry platform. Several studies, however, have reported on excellent early clinical outcomes with the latest single-port robotic technology. All of these surgeons had extensive robotic experience before attempting the single-site method.50–58,60,63–68 This differs from our setting, in which proficient laparoscopists with variable experience in robotic surgery participated. We did not observe differences in performance between the robotic novices and experts. This illustrates the advantage of robotic surgery in performing more complex tasks.
In this respect two articles are of specific interest. Spinoglio et al. compared the learning curves in single-port laparoscopic cholecystectomy with single-port robotic cholecystectomy. 63 The surgeries were performed by surgeons well-experienced in both laparoscopic and robotic surgery, but with no specific experience in single-port laparoscopy. This study on the learning curve for robotic single-site cholecystectomy concluded RSILS to be a safe and feasible option, even during the early cases. This was illustrated by the fact that these surgeons, experienced in conventional four-trocar laparoscopic cholecystectomy, only needed a short training period in RSILS to achieve good and steady operative times without major complications. It was observed that dissection, ligation, and transection were faster in RSILS compared to the SILS setting. 63 Angus et al. described the learning curve for robotic single-port cholecystectomy by one single surgeon, experienced in laparoscopy, who had no experience in robotic surgery. The authors observed that the learning curve was short and clinical results were comparable to those of robotic experts. 60 It was concluded that a robotic surgery novice, with extensive laparoscopic experience could safely be trained to perform robotic single-port laparoscopy.
Robotic technology is constantly improving. The authors believe that, with further development in robotic technology, this robotic single-port laparoscopy will be applicable on future platforms of all types, and not specifically the da Vinci Si single-site platform. It has to be acknowledged that each robotic platform has its own specifically developed single-port, but the technical surgical aspects of working with these different single ports will be comparable.
Why would RSILS be easier to perform than its conventional laparoscopic counterpart?
The RSILS setting restores the intuitive control that is lacking in laparoscopic single port surgery. The robotic single-port instruments allow the surgeon to associate his or her hands with the instrument tips, regardless of the robotic arm that holds the instrument. Therefore, the surgeon uses the right hand for the instruments visualized on the right side of the operation field, even if the instrument comes from the left. 59 Working in this robotic chopstick single-port laparoscopy setting is more comparable to four-port laparoscopy than conventional single-port laparoscopy. A previous study by the authors showed that for novice laparoscopists single-port laparoscopy on a dry platform was as easy to learn as conventional laparoscopy, probably because of the fact that no laparoscopic memory and adapted skills exist yet. 69 The advantage we observed in this study for the robotic chopstick approach can probably be explained by the fact that laparoscopically experienced surgeons lean on their laparoscopic memory and previously adapted skills when performing the RSILS setting. In this way, the new technique (i.e., single port surgery) can be trained easier and faster.
We performed a very simple oral questionnaire on the wellbeing (e.g., comfort) after executing both tasks in both settings. All participants preferred the RSILS setting. This setting caused less fatigue and a better ergonomic experience. Considering the fact that surgeons nowadays are mainly working laparoscopically and therefore will practice laparoscopy for several decades, ergonomics and comfortable working are essential. Heemskerk et al. showed that the use of robot laparoscopy leads to less physical stress and mental strain of the surgeon as compared to conventional laparoscopy 70
Limitations of this study are the relatively small number of participants and the small number of repetitions of the tasks. A low number of repetitions, as in this article is not enough to describe a proper learning curve. Nevertheless, even the three runs already showed significant improvement in performance of the first task. This suggests a steep learning curve of the technique for experienced laparoscopic surgeons. It may be possible that with a longer learning curve the performance in errors and times equalizes for both groups.
Experienced laparoscopic surgeons will be more eager to adopt a new technique if the learning curve is not too long and if the time of performance not much longer as compared to their conventional technique. This article shows that for experienced laparoscopic surgeons with no single-port experience and a variable robotic experience, robotic surgery facilitates single-port laparoscopy at the beginning of the learning curve. One of the general arguments used against the use of robotic surgery is the longer setup time for the robot and its cost. Although the setup time in robotic single-port laparoscopy and its direct costs are higher, this might be compensated by a decreased completion time of the procedure and better ergonomics and less working disability.
Conclusion
We can conclude that RSILS is feasible, faster, and easier to perform with less error on a dry platform, compared to the SILS setting. Furthermore, especially in more difficult tasks the robotic setting appears to be of advantage. Further research and randomized studies are needed for a better insight in the differences in learning curve between conventional and robotic single port laparoscopy, with an emphasis on the ergonomics.
Footnotes
Acknowledgments
The authors acknowledge Prof. G. Beets, MD, PhD, E. Belgers, MD, P. Callewaert, MD, Prof. Maessen, MD, PhD, T. Tuyten, MD, PhD, O. Uludag, MD, PhD, T. Van Gorp, MD, PhD, J. Van Roermund, MD, PhD, and Diana Onstenk for their contribution.
Disclosure Statement
No competing financial interest exists.