
Abstract
Abstract
Peritoneal dialysate leakage is a well-known complication of continuous ambulatory peritoneal dialysis (CAPD). In late leakage, it is usually managed conservatively and subsequently converted to hemodialysis. We hereby report a case of peritoneal dialysate leakage secondary to necrotic peritoneum, which was managed by laparoscopic excision of the affected peritoneum. Regeneration of new peritoneum was documented and the patient could resume CAPD successfully.
Introduction
P
Late dialysate leakage is usually conservatively managed by stopping the CAPD for a while until the peritoneum heals or by surgical intervention in cases of hernia. Here, we report our case of late dialysate leakage due to necrotic peritoneum, which was managed by laparoscopic excision of the affected peritoneum.
Case Report
A 48-year-old gentleman presented as bilateral pedal and scrotal edema and symptoms of fluid overload for 1 month, and also right abdominal wall edema during peritoneal dialysis (PD). He has been diagnosed to have end-stage renal failure secondary to hypertension for 5 years. He received three-port laparoscopic Tenckhoff catheter insertion and had uneventful PD for 5 years until the current admission. He has no other medical illness or other surgical history. He had urgent hemodialysis through perm catheter insertion on the right internal jugular vein and was investigated for dialysate leakage in the ward. The catheter outside abdomen was intact with no sign of peritonitis or hernia. The peritoneal fluid has no bacterial growth. The 99mTc-phytate scintigraphy showed dialysate leakage at the posterior-lateral aspect of the right upper abdomen (Fig. 1), whereas computed tomography (CT) scan of the abdomen showed right extraperitoenal leakage (Fig. 2). Otherwise, no radiological evidence of leakage in the pelvis was documented.
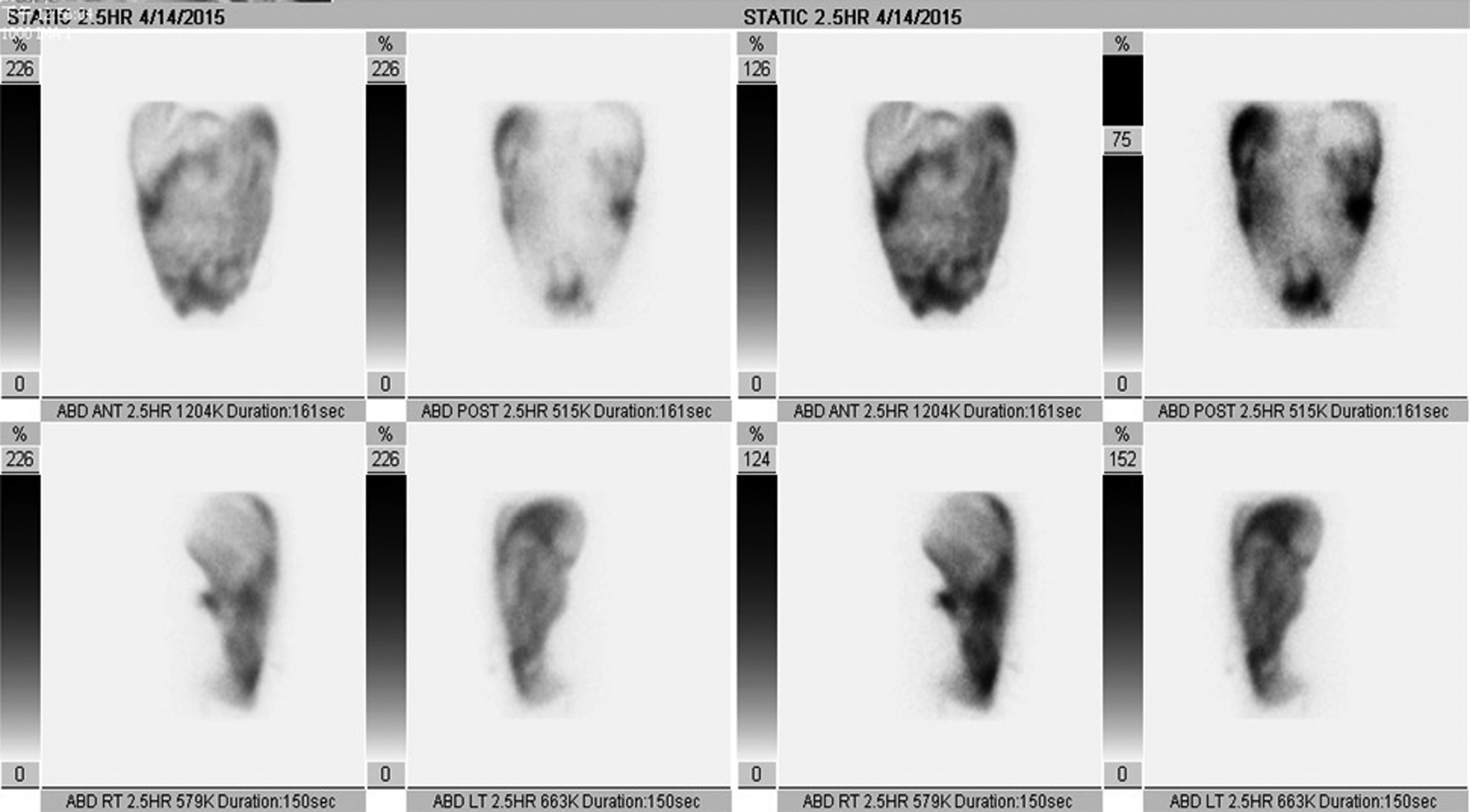
The 99mTc-phytase with CAPD dialysate peritoneal scintigraphy shows accumulation of radioactivity in the posterior-lateral aspect of the right upper abdomen near the hepatic flexure. CAPD, continuous ambulatory peritoneal dialysis.

Computed tomography of abdomen shows right extra-peritoneal leakage.
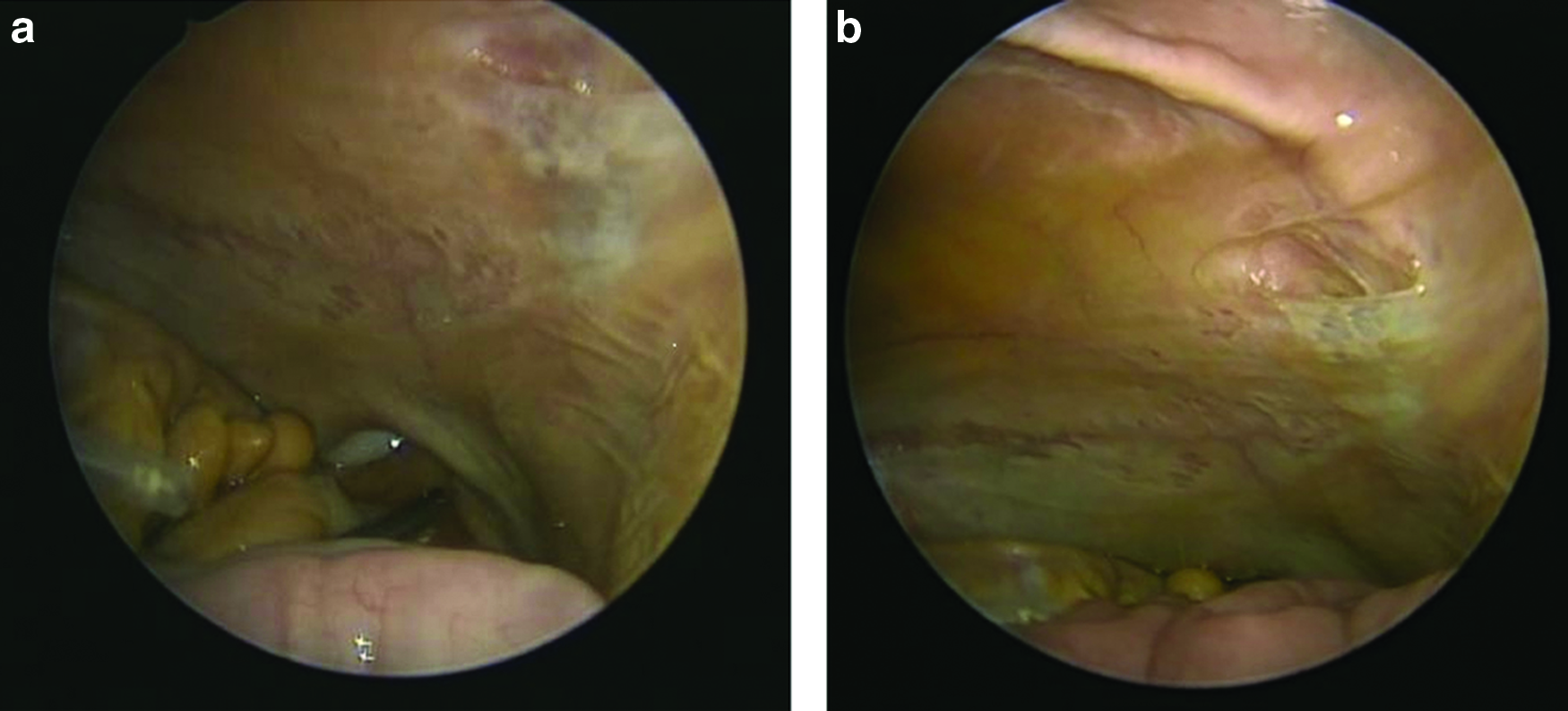
During the same admission, diagnostic laparoscopy was performed to find out the cause of this dialysate leakage. Three 5-mm ports were inserted at previous port sites and pneumoperitoneum was created. Fragile and nonelastic peritoneum in the pelvis with multiple perforations was found over the junction of right medial umbilical ligament and bladder region (Fig. 3a, b). The Tenckhoff catheter was intact and the rest of the abdomen was normal with no evidence of hernia, adhesion, or peritoneal perforation. The perforated and necrotic peritoneum (6.5 × 1.5 × 0.5 cm) was resected with a hook diathermy (Fig. 4). The port sites were closed with absorbable sutures. The histopathology result of the excised peritoneum showed fat necrosis and fibrosis.
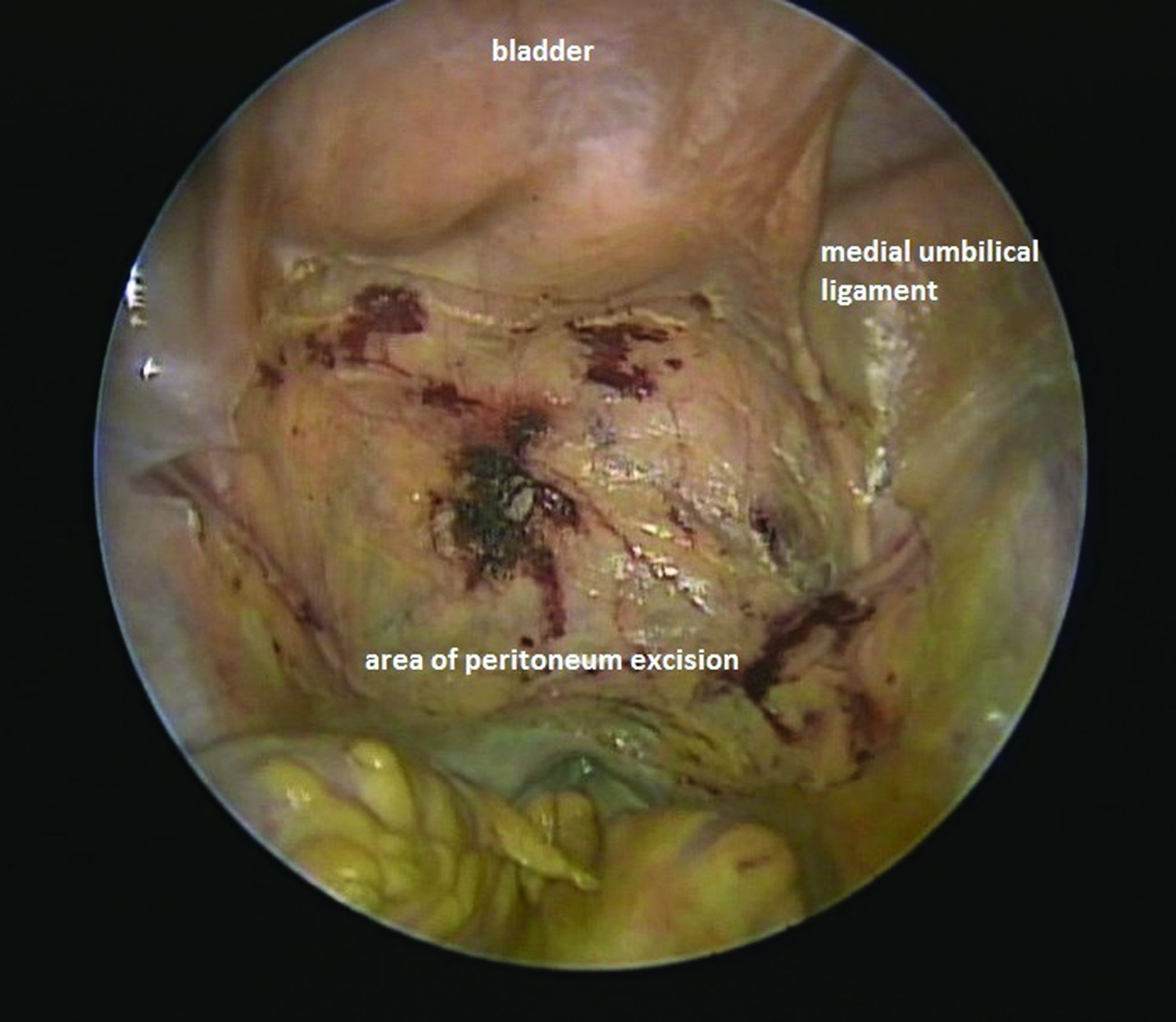
Laparoscopic view after excision of the affected peritoneum in the pelvis until the end of bilateral medial umbilical ligaments.
Meanwhile, he continued with hemodialysis using the perm catheter uneventfully. He was then readmitted electively for diagnostic laparoscopy 2 months later. Previous excised site of the peritoneum was completely regenerated with no evidence of adhesion to the pelvis and the Tenckhoff catheter was in situ (Fig. 5). The patient resumed his PD and the perm catheter was removed. The patient has uneventful CAPD for the past 1 year.
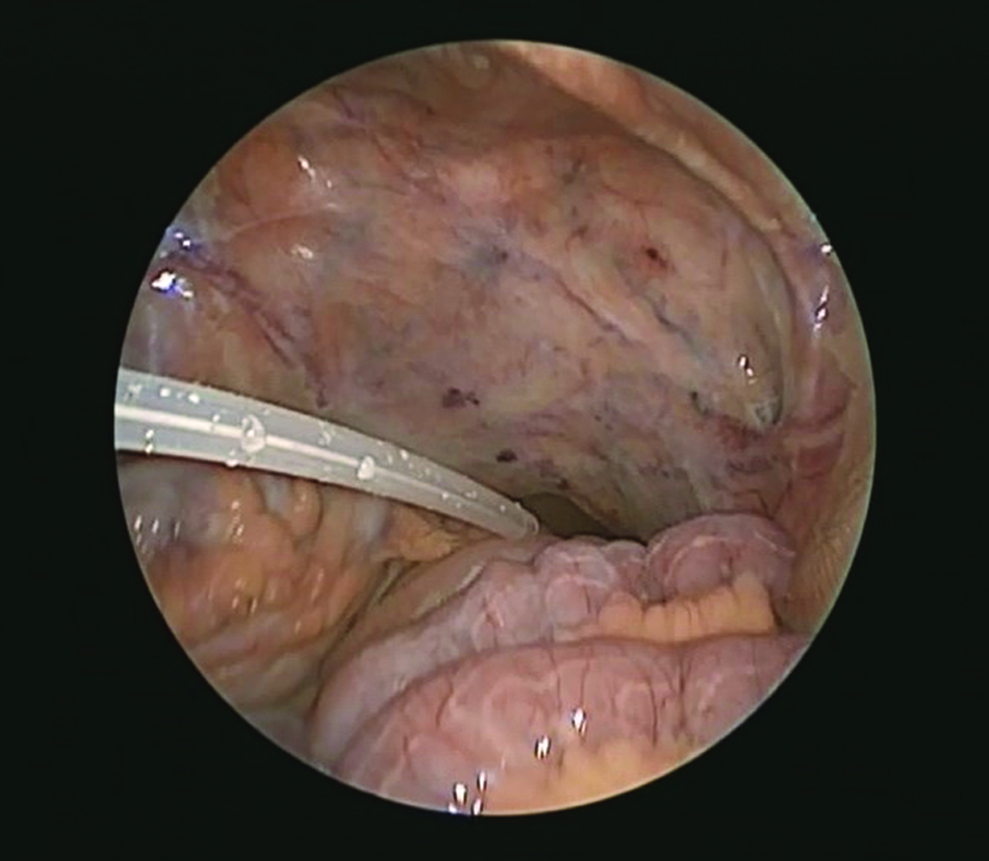
Laparoscopic view of Tenckhoff catheter and new regenerated peritoneum.
Discussion
CAPD is one of the renal replacement therapies. The long-term effectiveness of CAPD is limited by its complication, namely infection and noninfection causes. Dialysate leakage accounts for 5% of CAPD complication and may lead to localized edema and poor dialysate drainage and subsequently the CAPD becomes less effective. 3 Imaging modalities such as peritoneal scintigraphy, CT scan, and magnetic resonance imaging are useful tools for characterizing this dialysate leakage. 5
Dialysate leakage can either be early or late CAPD complication. In late dialysate leakage, it is usually related to peritoneal pathologies as seen in this patient. PD initiation increases inflammatory stimuli in such patients, such as the presence of the peritoneal catheter, use of bioincompatible dialysis fluids, and also infectious peritonitis. These factors result in structural and physiological changes of the peritoneal membrane either pores in the peritoneum or peritoneal fibrosis, which leads to failure of ultrafiltration and finally results in peritoneal dialysate leakage. 6
Most of the late dialysate leakage is managed conservatively. Such patients will be stopped from CAPD and put on hemodialysis meantime. CAPD will be resumed if there is no more dialysate leak. In cases of hernia, the hernia will be repaired. In our case, once the diagnosis of dialysate leakage was suspected, he was subjected for a diagnostic laparoscopy during the same admission. Laparoscopy showed fibrotic and necrotic teared peritoneum seen over the right inguinal region, but the PD tube was in situ and patent was with no sign of hernia or perforation at the tube insertion site. Excision of the affected peritoneum was done laparoscopically and the raw site of the anterior abdominal wall was left to heal for 2 months. A second laparoscopy showed completely healed peritoneum, thus enabling the patient to resume his CAPD immediately. As early as 1919, Hertzler 7 showed that when a defect was created in the parietal peritoneum of experimental animals, “the entire surface became endothelialized simultaneously and not gradually from the border as in epidermitization of skin wounds.” Mesothelial regeneration takes place immediately with the help of inflammatory mediators and fibroblast proliferation. This parietal peritoneum wound completely heals within 8 days. 8 Therefore, even 2 weeks of discontinuation of CAPD might be reasonable after this procedure.
If this necrotic and fibrotic peritoneum was left untreated as most literatures described, there will be a possibility of recurrence of this complication and then need to be converted to hemodialysis in near future. Laparoscopic excision of diseased peritoneum allows regeneration of new peritoneum; patients could keep the CAPD and might even prevent recurrence of dialysate leakage in the future.
Another concern is adhesion of bowel to a new growing peritoneum. Development of intraperitoneal adhesions is a dynamic process. Any surgically traumatized tissues in apposition bind through fibrin bridges and become organized with fibroblast proliferation. 9 However, in this case there was no adhesion noted during both surgeries. If there was a presence of intraperitoneal adhesions, placement of the adhesion barrier can be easily done laparoscopically. 10
Conclusion
Chronic dialysate leakage from necrotic peritoneum can be laparoscopically excised. It offered fast recovery, early resumption of CAPD, and might also prevent recurrence leak.
Footnotes
Disclosure Statement
No competing financial interests exist.