
Abstract
Abstract
Background:
Although laparoscopic left hepatectomy (LLH) for hepatolithiasis had been successfully performed in a series of cases, its advantages over open left hepatectomy (OLH) are still uncertain. This meta-analysis is to compare the clinical outcomes of LLH with those of OLH.
Materials and Methods:
A systematic literature research was performed to identify comparative studies on LLH versus OLH for hepatolithiasis from January 1991 to May 2016. Operative outcomes, postoperative outcomes, and gallstone clearance rate were evaluated. Pooled odds ratios and weighted mean differences with 95% confidence intervals were calculated using fixed-effect or random-effect models.
Results:
Eight studies, including one randomized controlled trial (RCT) and seven nonrandomized observational clinical studies, met the inclusion criteria. There were 739 patients in this meta-analysis, including 316 LLHs and 423 OLHs. The volume of intraoperative blood loss favored LLH (P = .015). Intraoperative transfusion (P < .001), overall complication (P < .001), and hospital stay (P = .001) were significantly low in LLH. There was no obvious difference in operation time, residual stone rate, and recurrent stone rate. The mean conversion rate was 9.5% (range, 2.2%–15.6%).
Conclusion:
LLH seems to be more effective and safer for selected patients with hepatolithiasis than OLH. As only one RCT was included, the evidence of which is still limited. More prospective, multicenter, and RCTs are needed to further define the real role of the laparoscopic technique in hepatolithiasis.
Introduction
H
Since 1990s, minimally invasive techniques have been applied to hepatectomy. Reich et al. 7 reported the first laparoscopic liver resection (LLR) in 1991. Azagra et al. 8 reported the first anatomic LLR in 1996 and Hüscher et al. 9 performed the first major LLR in 1997. After that inspiring initial experiences, laparoscopic hepatectomy has been utilized for the treatment of various liver diseases, including malignant liver tumors and hepatolithiasis. 10 And the international position of laparoscopic liver surgery has been widely recognized since Louisville's statement in 2008. 11 However, unlike cystic or solid liver tumors, patients with IHD stones have alterations of normal anatomical structures and perihepatic adhesions because of chronic recurrent inflammation, which may lead to laparoscopic procedures more difficult than open surgery.6,12 Although laparoscopic left hepatectomy (LLH) is being increasingly performed in selected patients with hepatolithiasis, open left hepatectomy (OLH) is still considered as the standard approach. Furthermore, the advantages of LLH over OLH for hepatolithiasis are still unclear, considering the limited volume in a single center. The aim of this study is to perform a systematic review and meta-analysis comparing the clinical outcomes of LLH with OLH for hepatolithiasis.
Patients and Methods
Study selection
A systematic review of the literature was performed to identify all studies published from January 1991 to May 2016, which reported data on outcomes of LLH and OLH. PubMed, EMBASE, Medline, and Cochrane Library were searched with the following search terms: “hepatectomy,” “hemihepatectomy,” “hepatic resection,” “liver surgery,” “liver resection,” “laparoscopic,” “laparoscopic assisted,” “minimally invasive,” “hepatolithiasis,” and “intrahepatic duct stones” in various combinations. The search was limited to studies involving human adults and publications in English. References of the acquired articles were manually searched again for additional studies.
Inclusion and exclusion criteria
For inclusion in the meta-analysis, a study had to meet the following criteria: (1) comparative study between LLH and OLH, including randomized controlled trials (RCTs) or observational clinical studies (OCSs); (2) description of at least one outcome of interest; (3) if more than one publication was reported from the same authors and/or institution, either the higher-quality study or the more recent publication was selected.
Abstracts, letters, editorials, expert opinions, reviews without original data, case reports, and studies lacking a control group were excluded. The following studies were also excluded: (1) those including right-sided hepatectomy in the study and (2) those evaluating patients with benign or malignant liver tumor.
Data extraction and quality assessment
Data were independently evaluated for qualification by 2 reviewers on the following data: first author, year of publication, characteristics of the study population, study design, number of subjects operated on with each procedure, operative outcomes, postoperative outcomes, and gallstone clearance. Inconsistencies were resolved through discussion until consensus was reached, or a third reviewer would take part in the discussion. The Newcastle–Ottawa scale (NOS) and Jadad standards were used to evaluate the quality of nonrandomized studies and RCTs, respectively. The total scaled scores of NOS range from 0 to 9, and studies having scores higher than 6 were deemed qualified. 13 Similarly, overall scores of Jadad standards range from 0 to 5, and scores of 0–2 and 3–5 were regarded as low and high scores, respectively. 14
Outcomes of interest
From all the selected studies, the following data were extracted: operative outcomes (operative time, intraoperative blood loss, intraoperative transfusion, and conversion rate), postoperative outcomes (overall complication, reoperation, length of hospital stay, and mortality), and gallstone clearance rate (initial gallstone clearance, final gallstone clearance, and gallstone recurrence rate).
Statistical analysis
Data analysis was performed using Stata 12.0 software. Dichotomous and continuous variables were estimated by odds ratios (ORs) and weighted mean difference (WMD) with 95% confidence interval (95% CI). Heterogeneity was evaluated by means of the χ2 test and P < .100 was considered significant. I2 values were used to evaluate statistical heterogeneity; an I2 value of 50% or more indicated the presence of heterogeneity. A fixed-effect model was initially performed for all outcomes. If the result presented significant heterogeneity, random effect analysis was used. Publication bias was examined by applying the Horbold–Egger's unweighted regression asymmetry test. Only studies that included 20 or more patients in each group were subjected to sensitivity analyses.
Results
Search results and study characteristics
The flow of reference selection is outlined in Figure 1. A total of 482 published articles were initially identified in the literature review. Then, 178 studies were excluded as duplicates and 287 articles were excluded based on the titles and abstracts for the following reasons: reviews, case reports, letters, editorials, expert opinions, and studies lacking a control group. The remaining 17 full-text studies were considered as eligible. Nine of the 17 studies were excluded because 4 studies included right-sided hepatectomy,15–18 2 studies compared laparoscopic hepatectomy with laparoscopic explorations,6,19 2 studies focused on safety and feasibility of reoperation for the treatment of hepatolithiasis by laparoscopic approach,20,21 and 1 study included benign and malignant patients. 22 Finally, eight studies were included in this meta-analysis, one study containing RCT 23 and seven studies containing nonrandomized OCSs.12,24–29 In total 739 patients met the inclusion criteria, including 316 LLHs and 423 OLHs. Study characteristics and quality assessment scores are summarized in Table 1.
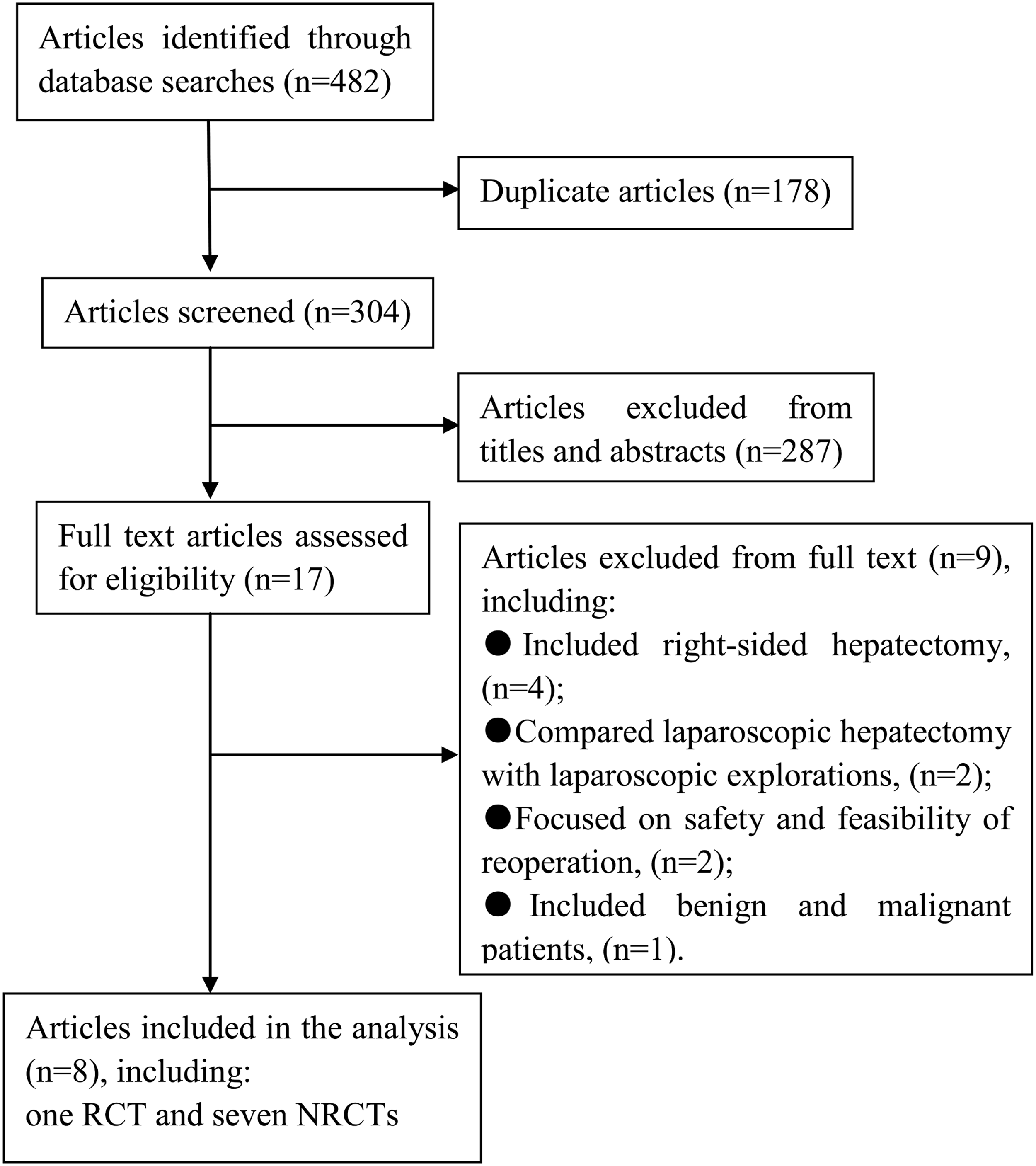
Study identification flowchart.
Jadad standards.
NOS.
Median with range.
F, female; LLH, laparoscopic left hepatectomy; M, male; NA, not available; NOS, Newcastle–Ottawa scale; OLH, open left hepatectomy; RCT, randomized controlled trial.
Operative outcomes
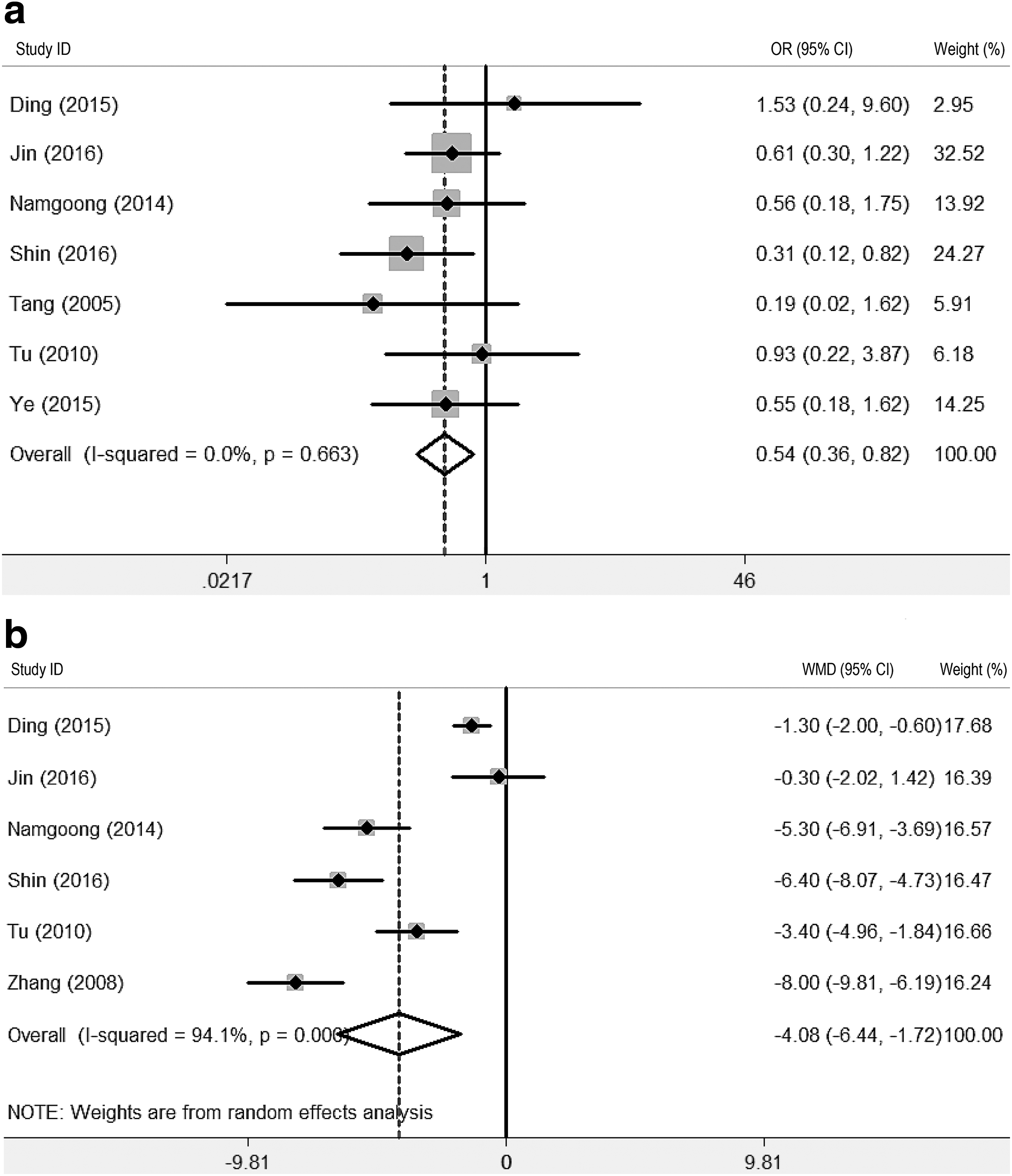
All eight studies reported operation time and six studies23–26,28,29 indicated the standard deviation (SD) of mean. The furnishing data showed that there was no significant difference between LLH and OLH with respect to operation time (WMD = −0.32, 95% CI: −1.26 to 0.62, P = .51; Fig. 2a), with significantly heterogeneity (I2 = 96.2%). Five studies23–26,28 reported operative blood loss with the SD of mean. The data showed that operative blood loss of LLH was remarkably lower than that of OLH (WMD = −87.56, 95% CI: −158.12 to −17.00, P = .015; Fig. 2b), and this finding was associated with significantly heterogeneity (I2 = 94.0%). In total six12,23–26,28 studies reported intraoperative transfusion, which was significantly lower in LLH (OR 0.32, 95% CI 0.18–0.57, P < .001; Fig. 3c). Conversion to laparotomy was reported in 19 cases in four studies.12,23,24,27 The mean conversion rate of LLH to OLH was 9.5% (2.2%–15.6%, Table 1). The common reasons of conversion were intraoperative bleeding24,27 and adhesion.12,23,24

Forest plots illustrating the results of operative outcomes:
Forest plots illustrating the results of postoperative outcomes:
Postoperative outcomes
All studies reported overall complications and the pooled data showed a significant difference favoring LLH (OR 0.46, 95% CI 0.31–0.69, P < .001; Fig. 3a). The pooled data of seven studies12,23–28 indicated that the surgical wound infection rate of LLH was dramatically lower than that of OLH (OR 0.31; 95% CI 0.15–0.66; P = .002). However, there was no obvious difference in the incidence of bile leakage (OR 0.84; 95% CI 0.37–1.91; P = .682) and abdominal collection with infection (OR 0.71; 95% CI 0.38–1.34; P = .291).
Six studies23–26,28,29 reported the length of postoperative hospital stay. Meta-analysis showed that patients with OLH had a significantly longer hospital stay than patients with LLH (WMD = −4.08, 95% CI −6.44 to −1.72, P = .001; Fig. 3b), with significantly heterogeneity (I2 = 94.1%). There was no operation-related mortality in all the studies of both groups.
Gallstone clearance rate
Five studies12,24–26,28 reported initial residual stone and the pooled data showed that no obvious difference was found between LLH and OLH (OR 0.74, 95% CI 0.39–1.43; P = .373; Fig. 4a). Similarly, there was no significant difference in the incidence of stone recurrence (OR 0.82; 95% CI 0.29–2.35; P = .712; Fig. 4b). Five studies12,24–26,28 reported final residual stone and just two studies24,26 showed that their patients had residual stone. Therefore, systematic review was performed. In Jin et al's 24 article, there were 3 (3/96) and 4 (4/105) patients with final residual stone in the laparoscopic and open group, respectively, and only 3 (3/54) cases in the open hepatectomy were found in Shin et al's study. 26 The sensitivity analysis results that excluded studies with fewer than 20 patients in each group are listed in Table 2.
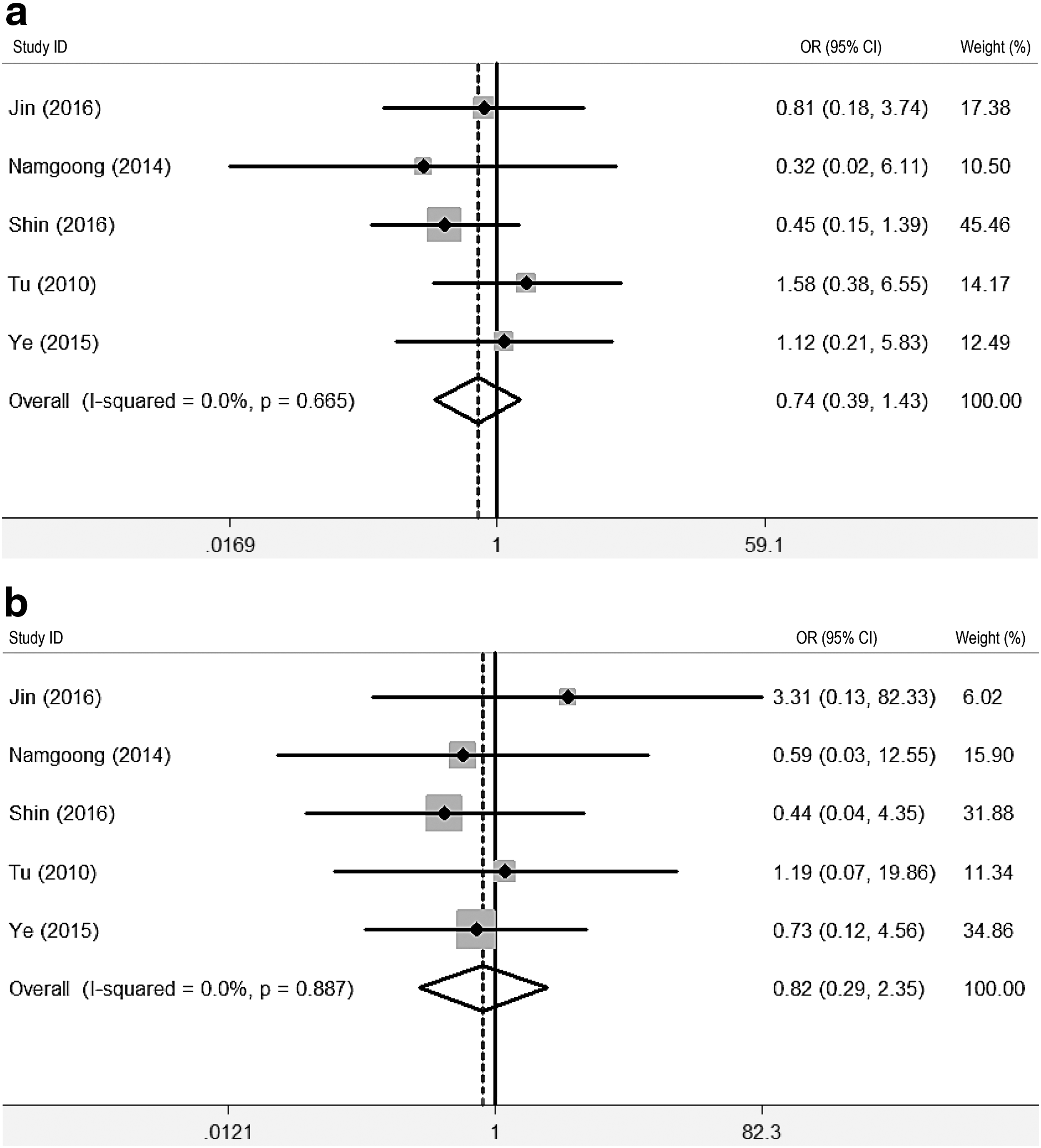
Forest plots illustrating the results of gallstone clearance rate:
Statistically significant results are shown in bold.
CI, confidence interval; LLH, laparoscopic left hepatectomy; OLH, open left hepatectomy; OR, odds ratio; WMD, weighted mean difference.
Publication bias
Publication bias was assessed, whereas the interpretability of the findings was limited by the low power with just eight studies.
Discussion
Symptomatic hepatolithiasis usually leads to intractable clinical courses, including recurrent gallstones and cholangitis, biliary strictures, hepatic parenchymal atrophy, and even malignant change. Therefore, partial hepatectomy is the best definitive modality for the treatment of hepatolithiasis. Traditionally, open hepatectomy is considered as the standard surgery for hepatolithiasis. 30 With the development of laparoscopic approaches, laparoscopic hepatectomy is being increasingly performed in selected patients with hepatolithiasis. 27 Recently, Ciria et al. 31 reviewed 9527 LLR cases worldwide, which contained 6190 malignancies and 3337 benign diseases. And the indication for intrahepatic lithiasis accounted for 8%. Cai et al. 32 reported 855 cases of laparoscopic hepatectomy, including 256 (29.9%) cases of hepatolithiasis. In this study, laparoscopic left-sided hepatectomy including left lateral segmentectomy and left hemihepatectomy accounted for 52.3%. In general, it is considered that LLR may improve the short-term outcomes of patients, including complications, transfusions, blood loss, and hospital stay compared with open liver resection.11,31 However, data validating the outcomes of LLH compared with those of OLH are scarcely reported. In addition, no systematic review and meta-analysis comparing LLH versus OLH for hepatolithiasis have been performed to our knowledge. In this meta-analysis, a comparison between LLH and OLH for hepatolithiasis was made and the results showed that LLH was as safe and efficient as OLH with no significant difference in operation time, mortality, residual stone, and recurrent stone rate. Moreover, LLH was more favorable with respect to intraoperative blood loss, intraoperative transfusion, overall complication, wound infection, and days of hospital stay. Sensitivity analyses that excluded studies with fewer than 20 patients in each group confirmed the aforementioned results. However, high statistical heterogeneity was found in some data, including operation time, operative blood loss, and postoperative hospital stay. Therefore, these data should be interpreted with caution.
Patients with left-sided hepatolithiasis usually suffer from underlying inflammation, severe perihepatic adhesions, deformed biliary anatomy, and fibrotic parenchyma, which may have the risk of serious intraoperative incidents and postoperative morbidity. Therefore, technical safety and efficiency of laparoscopic hepatectomy for hepatolithiasis should be tested, although the Louisville statement, mainly for solid liver tumor resection, proposes that laparoscopic hepatectomy is a safe and effective treatment for surgical liver disease in the hands of experienced surgeons. 11 In this meta-analysis, LLH was as safe and efficient as OLH with no mortality, and LLH was favorable in the field of intraoperative blood loss, intraoperative transfusion, overall complication, wound infection, and hospital stay. The mean conversion rate of LLH to OLH was 9.5%. In the case–control study of Zhou et al., 16 however, they found that laparoscopic hepatectomy was associated with a higher risk of intraoperative vascular incidents and a longer operation time in hepatolithiasis patients than open hepatectomy. The reason may be that they included four pairs of right posterior segmentectomy and two pairs of right hemihepatectomy in their study, and laparoscopic right-side hepatectomy is more difficult than LLH in surgical skills. In addition, there were 30 patients who underwent multiple episodes of biliary surgery before liver resection in the laparoscopic group of Zhou et al's study, which may also make liver resection more difficult. Hence, additional carefully designed studies are required to provide surgical safety of laparoscopic hepatectomy, especially laparoscopic right-sided hepatectomy, for hepatolithiasis in the future.
The main concerns about the use of the laparoscopic procedure for hepatolithias are the residual and recurrent stone rate. In this meta-analysis, there was no significant difference in the number of initial residual stones between LLH and OLH, although the pooled estimate tended to favor LLH. Similarly, the rate of stone recurrence was satisfactory in both groups without obvious difference. The reason for the low residual stone rate may be the removal of segment IV, which eradicates one of the major sites for residual stones after left lateral segmentectomy.15,24 In addition, some studies included in this meta-analysis used intraoperative ultrasonography, which compensated for the loss of tactile sensation and was also more accurate than tactile sensation in detecting and locating stones deep in the liver parenchyma.22,25 Similarly, with intrahepatic biliary strictures eradicated by left hepatectomy, the rate of stone recurrence was low in both groups. 24
This study has several limitations, which should be taken into account when interpreting the results. First, the biggest limitation is that only one RCT was included. Nonrandomized controlled trials (NRCTs) may exaggerate the effect of the approaches, either by external factors or by intrinsic flaws. It is a debated topic in the field of meta-analysis to pool data from NRCTs. However, several pieces of evidence have proved that the data of well-designed NRCTs may be reliable. 33 In this study, the included studies are high quality NRCTs in the standard of NOS. Second, the characteristics of populations, the definition of the outcomes, and the learning curve of the surgeons vary considerably among the reviewed articles. These factors may result in heterogeneity and have a potential impact on our results. Finally, from a clinical standpoint, we are interested in comparing LLH with OLH for further parameters with regard to the position of hepatolithiasis, liver stone size, intraoperative incidents, and cost. However, it is impossible to generate a more in-depth comparative result because the studies are either not reported at all or just have covered some descriptive statistics.
In summary, this meta-analysis suggests that LLH is as safe and efficient as OLH for hepatolithiasis. Given that much of the evidence comes from NRCTs, the conclusion is still limited. More prospective, multicenter, and RCTs are needed to further define the real role of the laparoscopic technique in hepatolithiasis.
Footnotes
Disclosure Statement
No competing financial interests exist.