
Abstract
Abstract
Introduction:
Thoracoscopic repair of a congenital diaphragmatic hernia (CDH) in the neonate is controversial due to reports of increased hernia recurrence. A multicenter review on thoracoscopic CDH repair was conducted to evaluate outcomes and to identify factors that are associated with recurrence.
Methods:
A multicenter retrospective review was conducted from 2009 to 2015 in neonates who were treated for CDH with thoracoscopic repair. Demographics, preoperative, intraoperative, including repair techniques, and postoperative variables were analyzed by using descriptive statistics. Comparative analysis was performed between those patients who were repaired entirely thoracoscopically with hernia recurrence and those without.
Results:
One hundred nine infants, of whom 57% were male with an average gestational age at time of surgery of 39.6 ± 4.6 weeks and a weight of 3.4 ± 1.1 kg, were included. The median age at repair was 5 days (range: 3–9), 61% patients required vasopressor support, and 1.8% patients required extracorporeal membrane oxygenation (ECMO) cannulation before repair. Forty-five percent were repaired on high-frequency oscillatory ventilation (HFOV). Repair was completed thoracoscopically in 83 patients (76%), 68 (82%) were repaired primarily, 15 (18%) were repaired with a patch, and 50 (60%) had extracorporeal/rib fixation sutures. Recurrence occurred in 7 (8.4%) of those completed thoracoscopically. Factors found to be significant for recurrence included: vasopressor therapy (P = .02), repair on HFOV (P = .04), and the presence of the spleen in the chest (P = .04). There was no significant difference identified between technical variations in repair.
Conclusions:
These data suggest that thoracoscopic repair of CDH is feasible in carefully selected patients. However, there is currently no evidence to support a standardized surgical approach to thoracoscopic repair.
Introduction
T
Potential advantages of the minimally invasive approach include avoidance of laparotomy, excellent visualization, and better cosmesis.3–5 However, from early experience, concerns were raised that the recurrence rate was higher than the open approach. A meta-analysis of the early experience of thoracoscopy compared with open thoracoscopy found a higher risk of recurrence with thoracoscopy. 6 Surgeons continue to develop techniques to reduce the risk of recurrence while simultaneously trying to understand which patients are the best candidates.
In this multi-institutional study, we sought to review the present state of selection of infants for CDH repair and to identify the surgical aspects that are associated with recurrence.
Materials and Methods
Seven tertiary-care pediatric hospitals from the United States, Germany, and Japan participated in an Institutional Review Board-approved (No. 1490411) retrospective analysis of infants, 3 months of age or less who underwent thoracoscopic CDH repair. To capture the contemporary experience, cases were included from August 2009 to January 2015. All consecutive cases initiated thoracoscopically were included. Each institution performed a standardized individual chart review to capture demographics, operative details, hospital course, and follow-up outcomes. Data for categorical variables are reported as number and percentage; continuous variables are expressed as mean ± standard deviation for normally distributed variables and as median with ranges for the remainder.
Cases completed thoracoscopically were separately analyzed to identify risk factors associated with recurrence. Specific technical comparisons included primary versus patch repair, type of patch and suture used, as well as the use of extracorporeal/rib fixation suturing. Variables were compared with Pearson's chi-square test and Fisher's exact test for categorical variables and with two-tailed Student's t-test and Mann–Whitney U test for continuous variables. Statistical significance was achieved at a P value of ≤.05.
Results
A total of 109 infants underwent attempted thoracoscopic repair of their CDH during the time period. The outcomes of thoracoscopic repair and conversion to open repair are outlined in Figure 1. The average gestational age at time of surgery was 39.6 ± 4.6 weeks with an average weight of 3.4 ± 1.1 kg. There was slight male preponderance (57%), and 91% infants had a left-sided hernia defect.
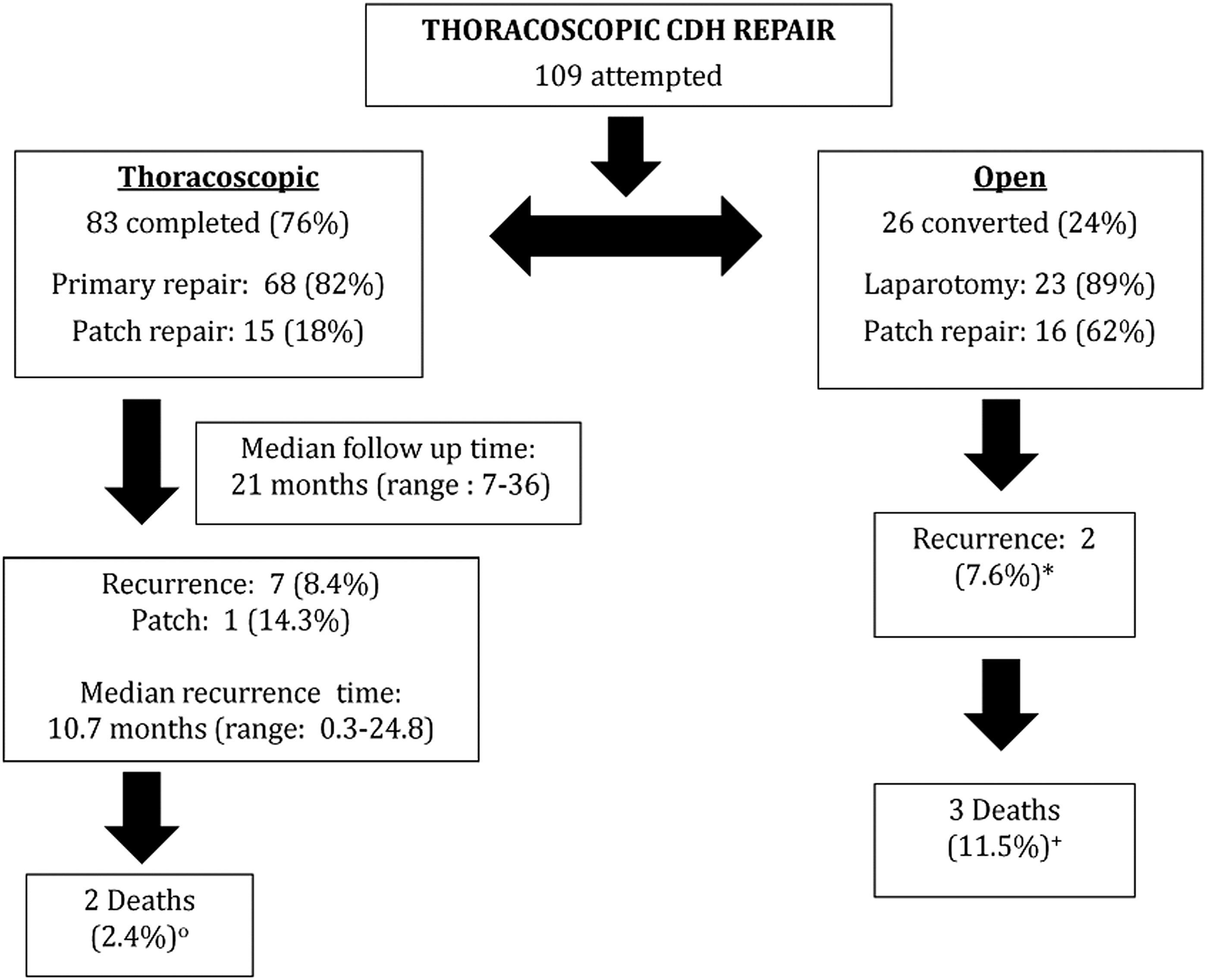
Flow diagram of study subjects who underwent attempted thoracoscopic CDH repair. *These recurrences were in the same patient who also required ECMO before repair. All repairs were with a patch. ○Neither patient had a recurrence before death. +One patient required ECMO before repair, and none had a recurrence before death. CDH, congenital diaphragmatic hernia; ECMO, extracorporeal membrane oxygenation.
Eighty-one infants received prenatal imaging before delivery; 67% (54) had ultrasound; and 33% (27) had both ultrasound and MRI. From this imaging, 12% (10) identified the liver, and 27% (22) identified the stomach to be within the chest. The prenatal lung area to head ratio in the 13 (12%) neonates with predicted values was an average score of 1.9 ± 0.9.
Preoperative adjunct comorbidities identified within the neonate group included structural cardiac anomalies in 12 (11%), with the majority having either dextrocardia or dextroposition with levocardia [n = 8 (7%)]. Pulmonary hypertension was diagnosed in 24 (22%) neonates; 6 (5.5%) neonates suffered from either an intraventricular hemorrhage or brain atrophy. Four (3.7%) had renal ectopia or hydroureteronephrosis, 8 (7.3%) had undescended testis or inguinal hernia, and two (2%) had an imperforate anus.
Preoperative
Vasopressor support was utilized preoperatively in 61% (66) infants for an average of 4 ± 3.7 days. Two neonates (1.8%) required extracorporeal membrane oxygenation (ECMO) cannulation before surgical repair, and none was repaired on or required ECMO after CDH repair. More than half (55%) of the neonates remained on room air or simple nasal cannula before repair, 16% (17) remained on conventional ventilation, and 29% (32) required escalation to high-frequency oscillatory ventilation (HFOV).
Perioperative
Median age at repair was 5 days (range: 3–9), and it was conducted by using HFOV in 45% infants (49). Intraoperative documentation identified hernia contents to include colon and/or small bowel in 92% (99), spleen in 51% (55), stomach in 21% (23), and liver in 13% (14). The size of the hernia defect was estimated in 86 neonates, with 19% (16) reported as a small defect (<2 × 2 cm), 58% (50) as moderate (2 × 2–4 × 4 cm), and 23% (20) as large (>4 × 4 cm).
CDH repair was successfully completed thoracoscopically in 76% patients (83), of which 82% (68) were repaired primarily with sutures only and 18% (15) were repaired with the use of a patch. Of those converted to open repair (n = 26), 89% (23) did so via laparotomy with 62% (16) repaired with a patch, as shown in Figure 1. The intraoperative complication rate was 4.6% (5): gastric perforation (1), mesenteric hematoma (1), splenic injury (2), and accidental extubation (1). Overall, the mean operative time was 139 ± 52 minutes.
Postoperative
The median time required for mechanical ventilation postprocedure was 5 days (range: 2–9 days), and the median time to start enteral feeds after repair was 4 days (range: 3–7 days). Postprocedure complications included: failed extubation attempts in 9.2% (10), tension pneumothorax or chylothorax requiring chest tube placement in 6.4% (7), small-bowel obstruction or ischemic bowel in 2.8% (3), and infection (central venous line or wound) in 3.7% (4). It took a median of 23 days (range: 13–34) after repair for the patient to meet discharge criteria, with a median length of follow-up of 21 months (range: 7–36 months). Hernia recurrence occurred in a total of eight patients (7.3%), with seven (8.4%) of those completed thoracoscopically. The median time of hernia recurrence in those seven was 10.7 months (range: 0.3–24.8 months).
Thoracoscopic CDH repair comparison
Table 1 summarizes the comparison of demographics between neonates with and without recurrence who were repaired thoracoscopically. There was no significant association identified in terms of gender, birth weight, hernia side, or preoperative comorbidities. All recurrences (n = 7) were left-sided defects, and the most common preoperative comorbidity was pulmonary hypertension [3/7 (43%)].
Values are presented as number (%) or mean ± SD.
ASD, atrial septal defect; PPHTN, persistent pulmonary hypertension of the newborn; VSD, ventral septal defect.
Table 2 shows the comparison in preoperative and perioperative variables between infants with and without recurrence who were repaired thoracoscopically. The use of vasopressors during the infant's hospital course was found to have a significant association between those who had a recurrence and those who did not [7/7 (100%) versus 39/76 (51%); P = .02]. In those infants who had a recurrence, almost twice as many days of vasopressor therapy was required (6.1 days versus 3.4 days; P = .06). There was no significant association found regarding the mode of ventilation before surgery, although this trended toward significance with a large effect size since more than half [4/7 (57%)] of those with recurrence required HFOV.
Values are presented as number (%), mean ± SD, or median (range).
Significant value.
Resected hernia sac out of those found to be present.
HFOV, high-frequency oscillatory ventilation.
Comparing peri-operative factors, there was a significant association found in those infants who had a recurrence and were repaired on HFOV [6/7 (86%) versus 29/76 (38%); P = .04] as well as in those whose hernia contained the spleen [6/7 (86%) versus 29/76 (38%); P = .04]. The size of the hernia defect, the presence of a hernia sac and whether resected or not, as well as the hernia contents of liver, colon/small bowel, or stomach were all found to have no significance in hernia recurrence.
Table 3 shows the comparisons of postoperative variables and complications between neonates with and without recurrence who were repaired thoracoscopically. There was no significant association found when it came to postsurgical duration of ventilation, enteral feed initiation, time to discharge, length of follow-up, or survival. The only complication identified as significant in infants with a recurrence on postoperative follow-up evaluation was a small-bowel obstruction and/or an ischemic bowel [3/7 (43%) versus 1/76 (1%); P = .01].
Values are presented as mean ± SD, median (range), or number (%).
Significant value.
When evaluating the technical variations in repair in the thoracoscopic group (n = 83), those repaired with a patch (n = 15) predominantly used it as an onlay repair (n = 11, 73%), with only three (20%) using it as a diaphragm replacement and one (7%) using the patch for both replacement and onlay. Extracorporeal/rib fixation sutures were used in 50 repairs (60%). Table 4 shows the comparison of these variations between infants with and without recurrence who were repaired thoracoscopically. There was only a single recurrence that was repaired with the use of a patch. Despite this finding, there was no significant association identified regarding type of repair, type of patch or suture used, and whether or not extracorporeal/rib fixation sutures were employed. The duration of the surgery for each group was also found to be similar.
Values are presented as median (range) and number (%).
Total number out of those repaired with patch.
Discussion
The role for thoracoscopy in CDH repair has been controversial as was shown in a recent IPEG survey, which found that 50% of respondents were of the opinion that thoracoscopy does not equal the open repair. 2 Some literature suggests a higher risk of recurrence with thoracoscopic repair when compared with open repair,6–8 whereas other authors fail to detect this.9,10 Because study results conflict, it has been difficult to determine whether the increased recurrence rate is secondary to patient selection, technical variation, surgical experience, or a combination of all that has been mentioned earlier.
This multi-institutional study attempted to evaluate the technical variation of thoracoscopic repair of CDH and to identify any associations with recurrence. Previous studies have described strategies for thoracoscopic repair, but none have done a side-by-side comparison.11–14 Primary versus patch repair, type of patch and suture applied, the technique of patch placement, and the use of extracorporeal/rib fixation suturing were compared. There was no statistically significant technical factor related to recurrence to currently recommend a standardized surgical approach to thoracoscopic repair.
In this series, surgeons might be selecting infants with more cardiopulmonary compromise. We found that the use of vasopressors and HFOV were significantly associated with recurrence, as well as with the presence of the spleen in the chest. Some authors have recommended the following thoracoscopic criteria: weight >2 kg, liver in the abdomen, no structural heart defects, no intestinal malformations causing obstruction, and no requirement for HFOV or ECMO. 11 This study, however, reveals a more liberal use of thoracoscopy at the present time.
It is unclear why HFOV use was associated with recurrence, but it may indicate a decreased total lung volume and some degree of pulmonary hypertension. These factors are usually associated with larger defects. Although no specific technical factors were identified as associated with recurrence in the side-by-side comparison, this may be secondary to sample size without enough recurrences yet detected to show technical differences.
The use of vasopressor therapy was associated with hernia recurrence, and the duration of therapy was almost double that of those without recurrence. In our cohort, 43% infants had documented pulmonary hypertension, but disease severity in each infant was not evaluated. Similar to our series, a recent study evaluating the influence of pulmonary hypertension (PHN) and re-herniation in children with thoracoscopic CDH repairs, managed without ECMO, found a significant increase in recurrence in those children who required HFOV and preoperative vasodilators. 15
None of the infants in this series was repaired on ECMO or subsequently required it. However, two infants who required ECMO preoperatively were converted to open repair via laparotomy. One had two hernia recurrences. The second infant died of recurrent pulmonary hypertension.
Technical difficulties experienced in this cohort included two splenic injuries that necessitated conversion. Of those completed thoracoscopically, 86% (6) of infants with a recurrence had spleen in the chest, which also may be a surrogate for a larger, more challenging hernia defect.
In the 83 patients from our series repaired thoracoscopically, the overall recurrence rate was 8% with a median follow-up period, for those who had a recurrence, of 29 months (range: 23–35 months). The median time to recurrence was 10.7 months after surgery. Three recurred during the initial hospital stay, and three recurred after 1 year of age. A recent two-center experience also reported an 8% (5) recurrence with a mean follow-up time of 23 ± 9 months. 16 Two from that series had a recurrence within the first 3 months, and three others were identified >1 year after the operation.
There are several limitations to this study. First, this is a retrospective cohort study from multiple institutions with possible variations in data recording. The follow-up is also somewhat limited for a portion of the population. The defect size cannot be recorded precisely from a retrospective review of operative reports. Most importantly, due to the small number of recurrences in our series, logistic regression analysis of factors was not possible and technical factors could not be adequately investigated.
In conclusion, the thoracoscopic approach in this series appears feasible for CDH repair, as the majority of patients do not have a recurrence. Infants with a more systemic illness, such as those who require vasopressor therapy or HFOV, may be at a higher risk of recurrence.
Footnotes
Acknowledgments
The authors would like to thank Dr. Joanne Baerg from Loma Linda University Children's Hospital for presenting this abstract at the International Pediatric Endosurgery Group 25th Annual Congress in Fukuoka, Japan, in May 2016.
Disclosure Statement
No competing financial interests exist.