
Abstract
Abstract
Introduction:
Morgagni hernia (MH) is an uncommon type of diaphragmatic hernia, especially in adults. Laparoscopic or thorascopic approaches have been described in adults. There are few reported cases using the Da Vinci robot in children and no previously described cases in adults. We report our early experience and technique using the robotic approach for MH repair in adults and its potential advantages.
Method:
Robotic repair of MH was performed in 3 female patients. Four trocars were used to gain access to the abdomen. The hernia contents were reduced, the sac excised, and the defect closed primarily. A 4 × 6 inch bioabsorbable coating mesh was used in 2 patients and a biologic mesh in 1 for reinforcement.
Results:
Robotic repair of MH was technically successful in all 3 patients. The average operative time was 199.3 minutes, and difficult hernia exposure in one case caused prolonged surgical time. There were no intraoperative complications. Additional interventions, including a repair of a transverse colon serosal tear during the reduction of hernia contents, occurred in 1 patient. Two of the 3 female patients were discharged on postoperative day 1, whereas the other patient was discharged on postoperative day 3. There were no postoperative complications.
Conclusion:
Robotic MH repair is an alternative minimally invasive approach for adults that allows for precise sac excision and primary tension-free repair with mesh reinforcement.
Introduction
M
The robotic system has the potential to offer advantages when performing these advanced laparoscopic techniques during MH repair. With the intuitive instrument articulation capabilities, complex operations that require intracorporeal suturing and precise dissection can be completed. 3 Being that this pathology is mostly seen in the pediatric population, there are now few reported cases using the robotic approach for the treatment of MH in children, but there are no previously described cases in adults. 4 Herein, we describe 3 cases using a robotic approach to repair MHs achieving hernia sac excision, primary tissue repair, and mesh implantation for reinforcement.
Materials and Methods
We conducted a retrospective review of patients who underwent robotic repair of diaphragmatic hernia, with a primary closure of defect and mesh implantation. Patients were identified by office scheduling records, followed by a review of office notes, operative reports, anesthesia records, operating room nursing notes, and hospital records. All patients had pulmonary symptoms at the time of diagnoses as opposed to the common belief that these patients often are symptom free at the time of diagnosis. 1 All patients underwent a CT scan of the chest as part of the preoperative workup. Age, sex, length of stay, blood loss, anatomic distribution of the hernia, perioperative complications, operative time, surgical repair technique, hernia sac contents, size of defect, and type of mesh implanted were all recorded.
Surgical technique
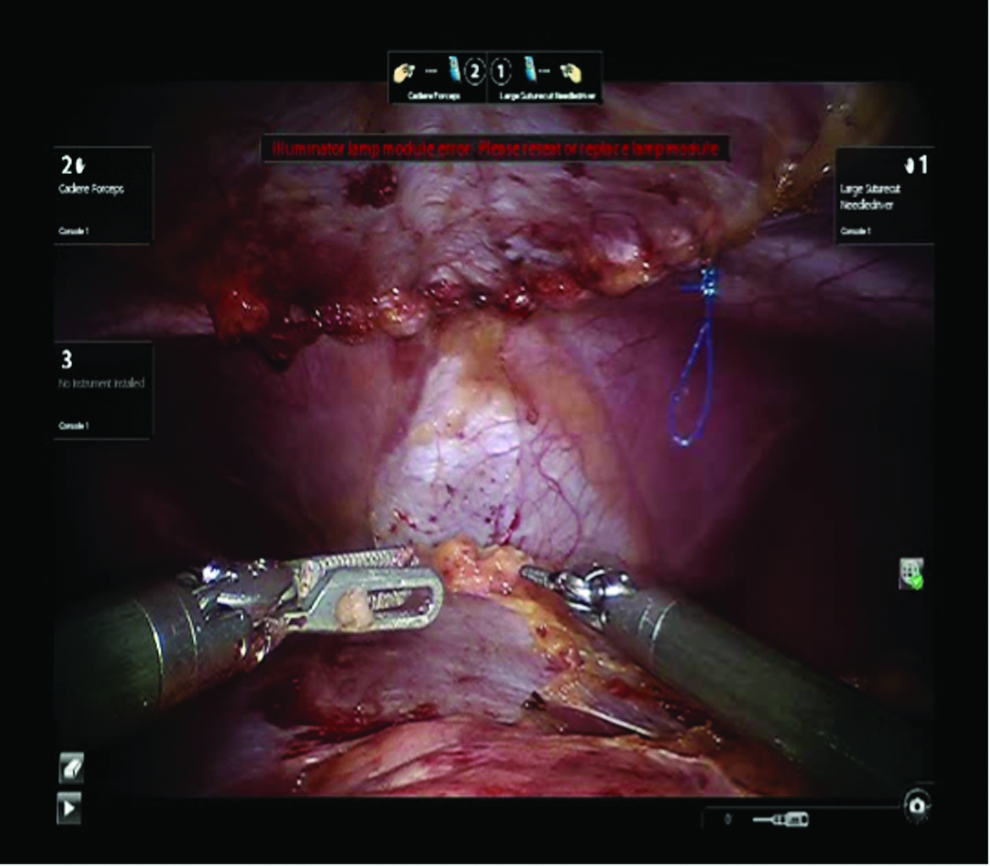
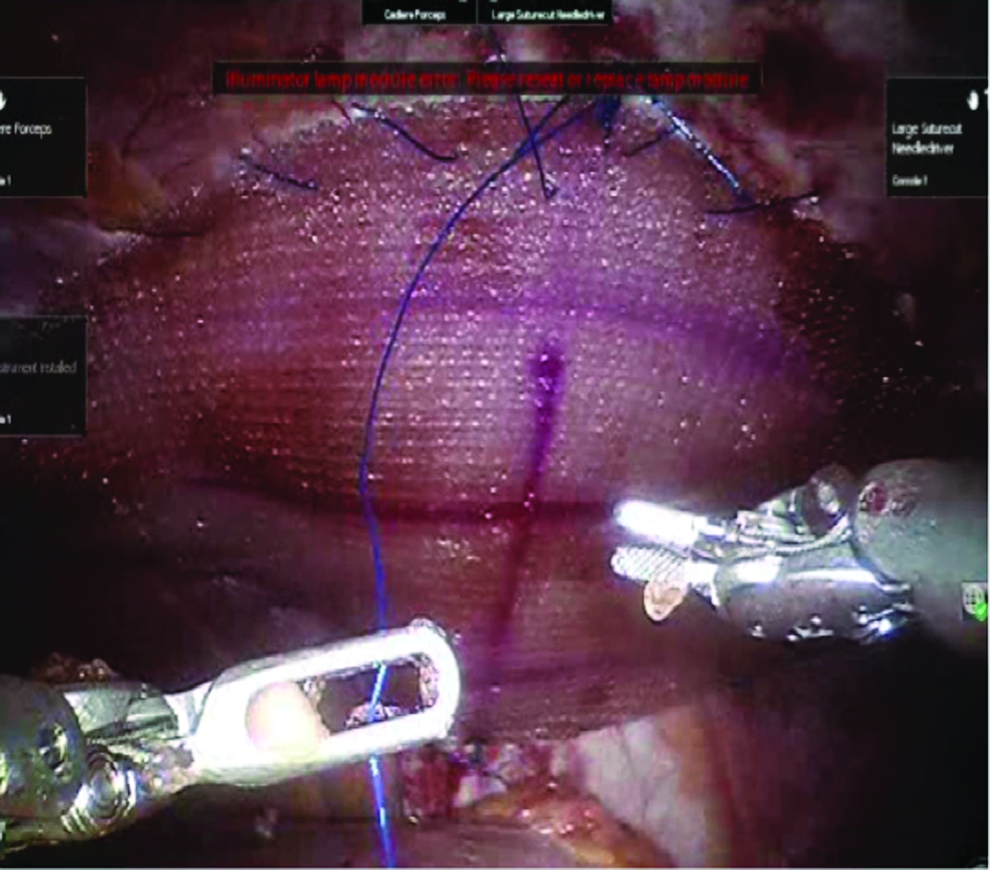
The patient is positioned supine on the operative table. Both arms are tucked. Preoperative prophylactic antibiotics are given and an Ioban tape is placed in an attempt to minimize the risk of surgical site infections and any contamination of the mesh with skin flora. Pneumoperitoneum is achieved through a Veress needle in the left upper quadrant at palmers point and the abdomen is insufflated to 15 mm Hg. Next, a 12 mm plastic trocar is placed in the superior umbilical crease to accommodate the laparoscope; careful inspection of the diaphragm is performed to localize the anatomic distribution of the hernia, size, and its contents. Under direct vision, one 8 mm trocar is placed in the left upper quadrant at the anterior axillary line slightly above the level of the umbilicus for arm 1, and a second 8 mm trocar is placed in the right mid clavicular line at the level of the umbilicus for arm 2. Arm 3 is placed along the anterior axillary line almost at the same level. A fourth trocar was placed between the camera and arm 1 as the assistant port. This is usually an 8 mm trocar although it can be replaced for a 12 mm to accommodate the ultrasound probe if needed (Fig. 1). Subsequently, the patient is placed in steep reverse Trendelenburg position, allowing gravity to help reduce the hernia contents after which the robot is brought in over the patient's head and docked. However, if the hernia contents do not reduce spontaneously, they are reduced into the abdominal cavity with gentle traction using Cadiere forceps in arm 1 to retract the hernia contents and fenestrated bipolar forceps in arm 2. A small grasping retractor is used for arm 3 (Fig. 2). The hernia sac is dissected circumferentially meticulously separating adhesions between the hernia sac and pleura. This is done with Cadiere forceps in arm 2 and monopolar curve scissors in arm 1 to free any intrathoracic adhesions. The primary diaphragmatic defect is then measured and closed primarily with a running 0 Prolene V-lock suture. This is done using a large suture cut in arm 1 and Cadiere forceps in arm 2 (Fig. 3). If the defect is >8 cm, it can be closed starting laterally and medially and tied in the middle of the hernia defect to reduce tension. For left-sided diaphragmatic hernia, we mobilized the upper pole of the spleen to accommodate placement of the mesh, while still allowing the spleen to lie anterior to it. Identification of the left diaphragmatic crus is necessary, as the primary closure of the defect can cause widening of the hiatus. Before closure of the hernia defect, the anesthesiologist would give a few deep breaths to evacuate any CO2 that was in the lung before closing the fascial defect.

Trocar placement (colored circles) and robot docking (arrow).

Hernia sac reduction.
Primary closure of the hernia defect.
Once primary closure of the defect has been completed, the closure is reinforced with a duo layer mesh or a biologic mesh, sutured in place with 0 Prolene placed at four quadrants, and subsequently sutured in a running manner around the circumference of the mesh (Fig. 4). Care must be taken not to injure the pericardium if the dorsal side of the mesh is within proximity to it. Once this is secured, the hernia sac is then removed through the 12 mm port site.
Mesh placement.
Results
Three female patients underwent the robotic repair of MH with sac excision, primary closure, and mesh placement between May 2014 and June 2016. Patient ages were 21, 23, and 78 years old. All the patients had respiratory symptoms described predominantly as shortness of breath with activity subsequently followed by slight chest pressure. Preoperative imaging included chest X-ray and chest CT (Fig. 5). As a result, 1 patient had been treated for pneumonia from an infiltrate seen on a chest X-ray. The anatomic distribution of the hernias is such that two were located in the right diaphragm and one in the left. The average time for the right-sided diaphragmatic hernia was 149 minutes, and that for the left-sided hernia was 300 minutes. The estimated blood loss was minimal and no patient required transfusions for bleeding. Hernia defects had a greater transverse dimension than the anteroposterior dimension, the former ranging from 6 to 8 cm, respectively. The patient with the left-sided MH required a concurrent procedure, intraoperative upper gastrointestinal endoscopy, and primary closure of the hiatus. The types of mesh for reinforcement included dual layer mesh for the right-sided hernias and gore BioA for the left-sided hernia. There were no postoperative complications and the average length of stay was 1.6 days. The 2 younger patients were discharged in postoperative day 1. The follow-up ranges from 2 to 24 months. There were no 30-day postoperative complications and their respiratory symptoms have improved.
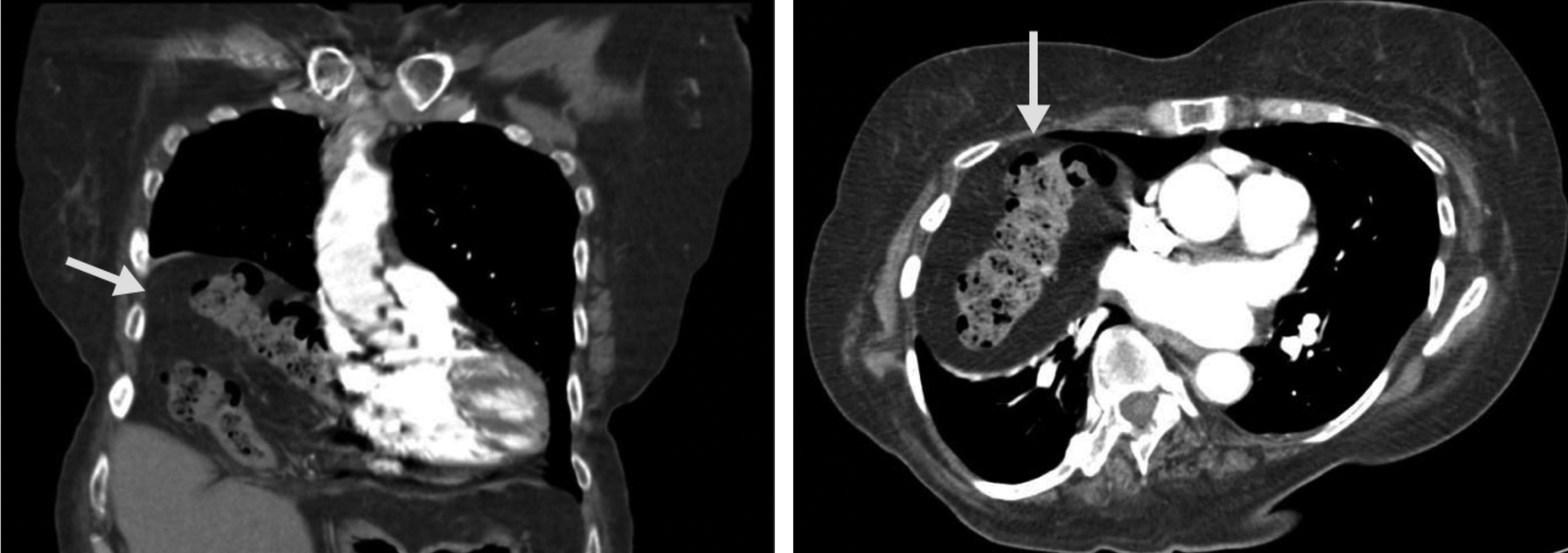
Computer tomography of the chest. Right side coronal section and left side axial section. Arrow pointing toward the Morgagni hernia.
Discussion
MH is a congenital diaphragmatic hernia and its main state of treatment is surgical management. As surgical technology has evolved, new techniques for repairing this defect have been developed such as laparoscopic, thorascopic, and robotic assisted methods. These approaches have been employed when treating MH in children and described mainly in the pediatric surgical literature. Nevertheless, laparoscopic approaches have also been described for adults but only since 1992. 5 Furthermore, no robotic approach has been previously described in the surgical adult literature yet. Due to the relative rarity of MH present in the adult population, no appropriate or widely accepted technique for its repair currently exists. This article discusses the different surgical techniques currently employed in MH repair, and proposes a new surgical approach for the treatment of MH in adults using the Da Vinci robot.
There are three main controversies described in the literature for the repair of MH in adults: whether hernia sac should be excised, whether the defect should be closed primarily, and/or the use of mesh for bridging or reinforcement. Out of 46 laparoscopic cases reported in the literature, the hernia sac is resected in 31% of the cases, primary closure of the defect is in 29% of the cases, and mesh placement is in only few of the cases (7%). 1 Taking into account the different techniques in the repair of MH, the Da Vinci robot offers several advantages and allows for a more efficient way to handle any of these techniques. The laparoscopic approach for MH repair, although difficult, lengthy, and not totally without risk, could account for the controversies that currently exist regarding the surgical repair. The robotic approach offers the advantage of improved dexterity, 3D observation, seven degrees of freedom, and elimination of physiologic tremors, which are paramount during the sac excision. 6 Moreover, it provides a favorable ergonomic position for these lengthy procedures.
All of our cases had excision of the hernia sac, which coincides with the conventional surgical principle of not leaving behind a loculated space lined by peritoneum to avoid residual cyst formation.7,8 Given that intrathoracic adhesions are likely to be encountered in this procedure, it could present limitations if the laparoscopic approach is employed due to the unfavorable angle between the instruments. 9 Contrary to the laparoscopic approach, robotic instruments offer superior capability for intracorporeal articulation of the surgical instruments and easy access to the right upper quadrant.
Primary repair of MH defect can lead to significant tissue tension. 10 This fact translates from other surgical procedures such as inguinal and hiatal hernia repairs. However, most MHs appear on the right side of the diaphragm and theoretically, in this location, there are less pericardial attachments. 11 Thus, the defect can be repaired primarily without undo tension.
Mesh placement decreases paraesophageal hernia recurrences. However, this is now debatable with newer data.12,13 Even though MH occurs in a less dynamic area of the diaphragm than the hiatus, this area is still predisposed to forceful contractions, which can yield to hernia recurrence. Similarly, erosion of sutures placed in muscle fibers leads to the same results. 14 To mitigate these risks of hernia recurrence, we reinforced the primary repair with a dual layer mesh in both of our patients.
As it is well understood, minimally invasive procedures for MH repair result in decreased hospital stay, decreased pain, and quicker recovery. We were able to replicate these data using the robotic approach. Two of our patients were discharged on postoperative day 1 and the other was discharged on postoperative day 3 with no perioperative complications.
Conclusion
In conclusion, we report the first 3 cases in the literature of robotic repair of MHs in the adult population, using a hybrid technique of primary closure and mesh reinforcement, while capitalizing on the advantages of the articulating instruments of the robotic device. It is difficult to advocate a robotic approach over the laparoscopic approach when there is scarce literature about MH repair in adults. Overall, using the advantages of the Da Vinci robot may be an important addition to the armamentarium of minimally invasive surgeons undertaking this challenging group of patients.
Footnotes
Disclosure Statement
No competing financial interests exist.