
Abstract
Abstract
The goal of this article is to illustrate the current minimal invasive approaches to patients with epiphrenic diverticulum in terms of preoperative evaluation, surgical technique, and outcomes. Two techniques will be presented: a laparoscopic and a video-assisted thoracic repair. Indications for each technique will be discussed as well as proper patient selection and management. Current controversies in the treatment of patients with this rare disease will be addressed.
Introduction
E
Specific symptoms of regurgitation of undigested food, nocturnal aspiration, and aspiration pneumonia are more likely clinical manifestations of the diverticulum. 2 Because of potentially life-threatening complications such as aspiration pneumonia, some have argued that epiphrenic diverticula should be always resected. Most of the current literature, however, suggests that the risks of surgical management outweigh the incidence of these complications. 4 Treatment of epiphrenic diverticula is thus reserved for severely symptomatic patients.
There is additional concern that larger diverticula have an increased, although still extremely small, risk for malignant transformation of the diverticular mucosa owing to longstanding inflammation. 2 Nevertheless, most reports of concomitant cancer within a diverticulum have involved squamous cell cancer. 5
The goal of this article is to illustrate the current minimal invasive approaches to patients with ED in terms of preoperative evaluation and indications for surgery, surgical technique, and outcomes.
Materials and Methods
We performed an electronic search of the literature in PubMed and Scopus database, using the following terms: diverticulectomy, minimal invasive diverticulectomy, laparoscopic diverticulectomy, and thoracoscopic diverticulectomy (Search string: “diverticulectomy[All Fields] AND minimal[All Fields] AND invasive[All Fields] AND diverticulectomy[All Fields] AND (“laparoscopy”[MeSH Terms] OR “laparoscopy”[All Fields] OR “laparoscopic”[All Fields]) AND diverticulectomy[All Fields] AND thoracoscopic[All Fields] AND diverticulectomy[All Fields]). All reviews and case reports were excluded. The first and senior author independently reviewed all articles and checked each reference cited to minimize bias in the search policy. Inclusion criteria were (a) clinical studies, including minimally invasive laparoscopic diverticulectomy; (b) clinical studies describing the thoracoscopic approach; and (c) articles that compared both approaches.
Results
From 1994 to 2016, only 17 original articles met our inclusion criteria. Six articles described the results for video-assisted thoracoscopic performance and 11 for laparoscopic approach. No studies comparing both techniques were found. The results of operations for epiphrenic diverticula are summarized in Tables 1 and 2. Both laparoscopic and video-assisted thoracoscopic surgery (VATS) approaches have similar clinical outcomes and complication profiles. Mortality rates ranged from 0% to 10% for both procedures.
Good outcome = significant improvement or resolution of symptoms.
N, number of patients; VATS, video-assisted thoracoscopic surgery.
Good outcome = significant improvement or resolution of symptoms.
N, number of patients; VATS, video-assisted thoracoscopic surgery.
Below we review our preoperative management and our preferred technique of minimally invasive treatment of ED: a laparoscopic and a thoracoscopic approach.
Preoperative management
In our experience, the evaluation should include the severity of the patient's symptoms; dysphagia, regurgitation, and aspiration are to be considered clear indications for surgery. The current diagnostic workup for epiphrenic diverticula includes a combination of barium swallow, upper endoscopy, and esophageal manometry. 6 The barium swallow determines the size and demonstrates where the diverticulum is located, which has implications in the accessibility of the diverticulum through a laparoscopic or transthoracic approach. In fact, diverticula that are located more than about 10 cm proximal to the gastroesophageal junction or that have wide necks may require a transthoracic approach to dissect the upper portion of the diverticulum from the surrounding mediastinal structures. 2 Esophageal manometry is used to diagnose and classify the underlying motility disorder. Due to the episodic nature of some of these motility disorders, it is important to note that manometry results might not always be abnormal. 7 However, given the correlation between epiphrenic diverticula and esophageal dysmotility, normal manometry results should not be used to guide the surgical management of the diverticulum. 2
Laparoscopic approach
The patient is placed in the supine position on a beanbag. Rapid sequence intubation should be performed to minimize gastric distention and risk of aspiration. Once anesthesia has been induced, the patient is placed in stirrups and reverse Trendelenburg. The surgeon stands between the legs. The trocar that will accommodate the 30-° laparoscope is inserted into the abdomen through a 1-cm supraumbilical incision (approximately one inch above the umbilicus). Four working ports are placed according to Figure 1.
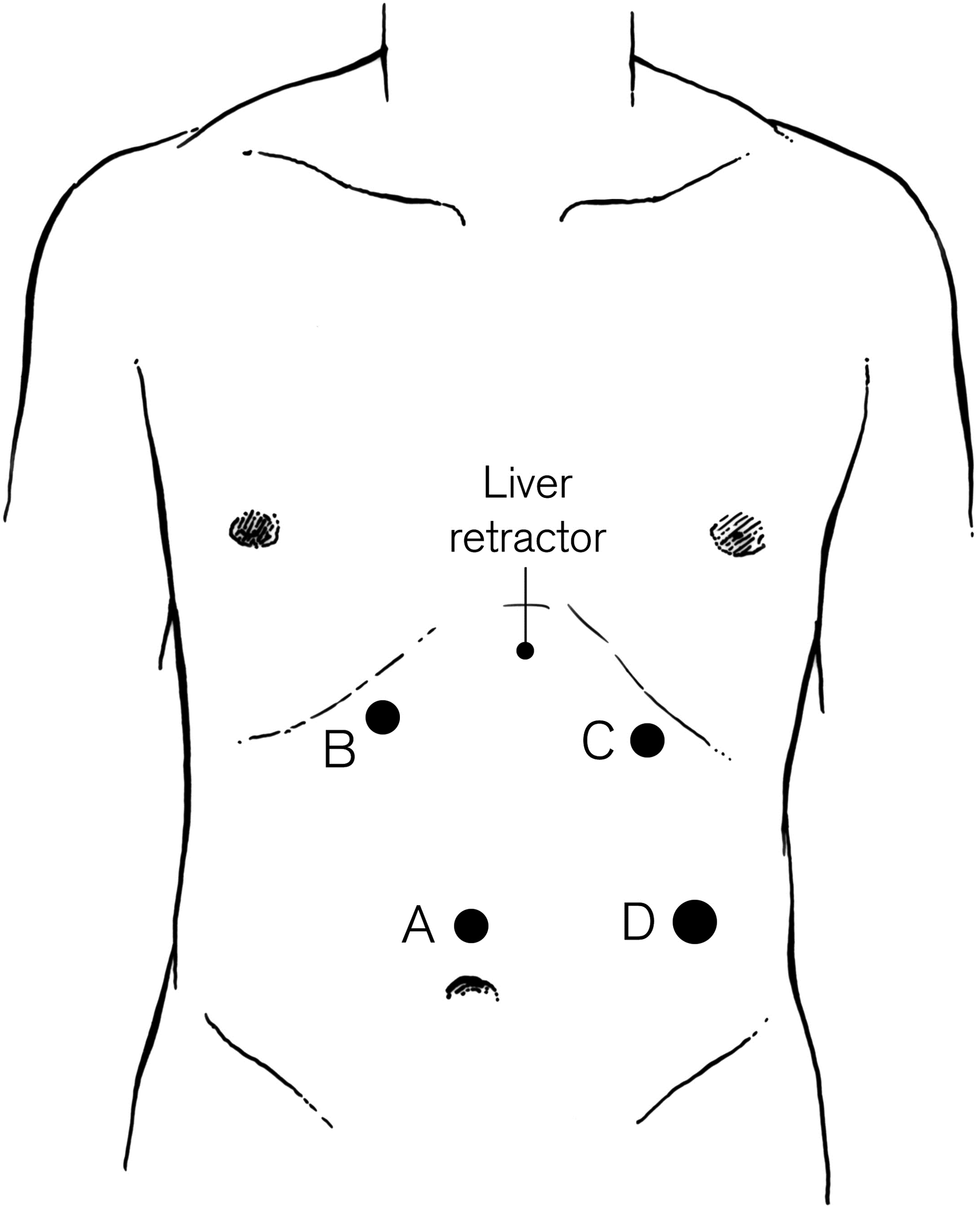
Laparoscopic Approach: port placement. Port A accommodates the laparoscope. Ports B and C are 11-mm working ports. Port D is a 12-mm port that accommodates the stapler.
Dissection starts by opening the gastrohepatic ligament. The right crus is bluntly dissected off the esophagus to gain access to the posterior mediastinum. The phrenoesophageal membrane is opened anteriorly from the apex of the right pillar to the apex of the left pillar of the crus. Both vagi should be identified and preserved. The mediastinal attachments are dissected and the diverticulum is exposed. A Penrose drain is passed around the esophagus and both vagi to allow atraumatic traction of the esophagus. Once the diverticulum is located, it should be carefully dissected off the dense adhesions to the pleura and the esophageal wall. Care should be taken to mobilize the diverticulum neck completely, especially the most cranial portion. Failure to mobilize the diverticulum completely may prompt the surgeon to perform a myotomy and fundoplication transabdominally and then convert to a thoracoscopic approach to complete the diverticular dissection and perform the diverticular resection. The resection is performed with an endoscopic stapler that accommodates a 2.5-mm vascular cartridge. The closure is reinforced by imbricating the staple line with interrupted sutures. Heavy silk interrupted sutures are used to close the hiatus before the myotomy. The myotomy onto the distal esophagus and proximal stomach is extended cranially up to the neck of the diverticulum and 2–3 cm caudally onto the anterior wall of the stomach. A partial anterior (Dor) fundoplication is preferred and prevents reflux after the myotomy. The short gastric vessels may be divided to enable a tension-free fundoplication. The gastric fundus is then sutured laterally to the apex of the left crus and the left edge of the myotomy. The stomach is folded over the myotomy and it is sutured superiorly along the diaphragmatic hiatus and medially along the right crus.
No gastric tubes are placed at the end of the operation. The patient is admitted overnight. On postoperative day 1, a barium swallow is performed to evaluate for a possible leak, obstruction, and esophago-gastric emptying. Then, the patient is advanced to a soft mechanical diet until a follow-up in clinic when dietary restrictions will be lifted.
Thoracoscopic approach
The patient may be placed in either the right or left lateral decubitus position, depending on the location of the diverticulum. Four ports are placed according to Figure 2. Additional heavy silk, diaphragmatic traction suture may be placed through the central tendon of the diaphragm and brought out through the lower anterior chest wall to improve visualization. The assistant stands in front and the surgeon stands to the back of the patient.
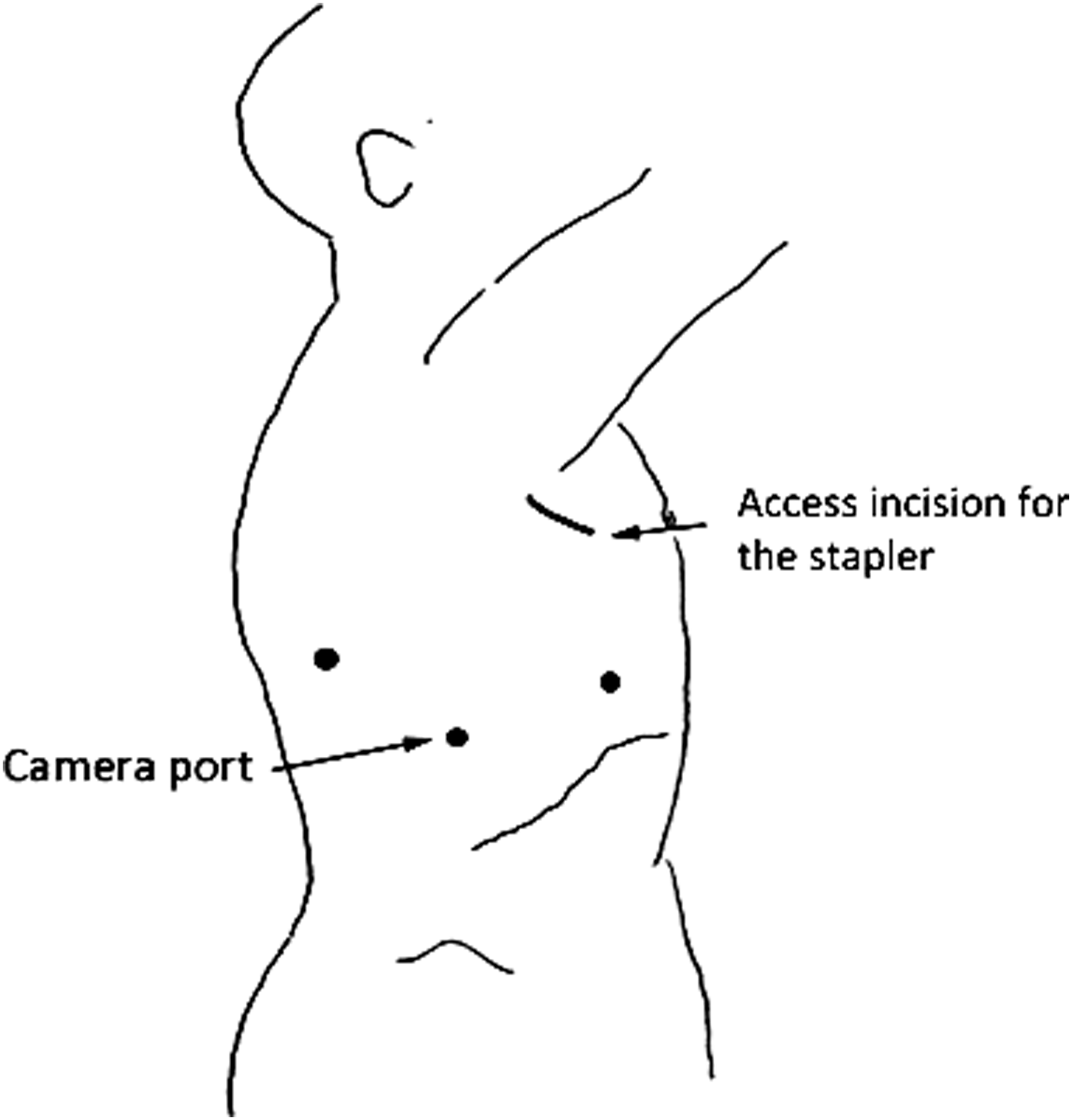
Thoracoscopic Approach: port placement. A 5-mm port that accommodates the laparoscope is placed low in the posterior axillary line. Two working ports are placed anterior and posterior to the optical port, and a 2-cm incision is placed anterolaterally in the fourth interspace for the stapler and the specimen removal.
The site of the diverticulum is identified. Dissection starts with division of the inferior pulmonary ligament. The mediastinal pleura, which overlies the diverticulum and the adjacent esophagus, is incised. The esophagus is mobilized circumferentially to permit exposure of the neck of the diverticulum. Care should be taken to avoid injury to the vagus nerves, which should be identified. A Penrose drain may be used to encircle the adjacent esophagus to facilitate retraction. The diverticulum is bluntly and sharply dissected free from the surrounding structures until its neck is completely visible. After the diverticulum is sufficiently dissected, an assessment is made as to whether resection of the diverticulum is needed. Small wide-mouthed diverticula may be left in situ, eliminating a risk of perforation or suture line breakdown. An endostapler is positioned at the base of the diverticulum and parallel to the esophagus. More than one firing of the stapler may be used in sequence; care should be taken to ensure that they are in line with each other. The muscular layers over the mucosa are approximated with running or interrupted absorbable suture. This reinforces the staple line and helps prevent contamination of the pleural space should a leak from the stable line occur.
To perform the myotomy, the esophagus is rotated 90–180° away from the site of the diverticulectomy. The myotomy extends from the origin of the diverticulum inferiorly onto the cardia. A pleural drainage tube is placed. A nasogastric tube is not required. A contrast swallow study is performed the following day if there is concern about possible mucosal injury. In the absence of such concerns, a diet is started on the first postoperative day and gradually advanced.
Discussion
Surgical management of the patient with a diverticulum includes three elements: myotomy, partial fundoplication, and possible diverticulectomy. The goal of the surgery is to address the underlying motility disorder, remove the diverticulum when appropriate, and prevent postoperative gastroesophageal reflux. Historically, a transthoracic approach through a left thoracotomy incision has been the standard of care. This allows optimal visualization and access to the distal esophagus and provides the best exposure for diverticulum resection, oversewing of the esophageal musculature, and myotomy. In the last decade, however, laparoscopy has become a reasonable approach for surgical management in most cases and has been shown in numerous clinical studies to be effective in providing symptomatic relief. 8 Regardless of whether treatment is done through an open, thoracoscopic, or laparoscopic approach, morbidity and mortality may be considerable. The most serious complication is esophageal leak either from the staple line or from missed mucosal disruption during the myotomy. Sepsis, pneumonia, empyema, and abscess have lethal potential and should be addressed quickly when identified. Failure to perform an esophageal myotomy may result in high-pressure zone distal to the resected diverticulum staple line, which can cause a leak with disruption of the staple line. 9
Given its strategic location in the lower thoracic cavity, an ED can be approached both from the chest and from the abdomen. Laparoscopy allows an easy approach to the upper abdomen, accessible creation of the myotomy, and partial fundoplication, while it spares the need for one-lung ventilation. 10 However, these advantages may be limited in cases of a large size of the diverticulum, long distance between the diverticulum and the hiatus (∼8–10 cm), and dense adhesion in the mediastinum.11,12 In these circumstances, VATS may be more suitable as either single or combined procedures with laparoscopy. In these combined procedures, some authors suggest that a laparoscopic procedure should be performed before VATS to prevent loss of air into the dissected pleural space.12,13
Conclusions
Minimally invasive surgery for the treatment of ED is reliable with satisfactory results, both with thoracoscopic and laparoscopic approaches. Unfortunately, as of today, there are no studies that evaluate these two techniques simultaneously. Moreover, the variety of surgical techniques used, differences in outcome measurements in each report, and disparities in patient selection for each operation make the studies we have found in literature difficult to compare. In our current practice, we consider laparoscopic myotomy with or without diverticulectomy, the preferred method for most EDs.
Footnotes
Disclosure Statement
No competing financial interests exist.