
Abstract
Abstract
Introduction:
Diagnostic laparoscopy is well accepted in the management of penetrating abdominal trauma (PAT). Therapeutic laparoscopy, on the other hand, remains controversial. In patients with multiple hollow viscera injuries, laparoscopy is usually converted to laparotomy. We aim at describing the laparoscopic-assisted technique in the management of patients with PAT. Using our experience with laparoscopy, we tailored the technique to the setting of PAT.
Methods:
The laparoscopic-assisted approach (LAA) was adapted to a trauma setting and prospectively evaluated. The technical details and indications for the technique were investigated. The distinctive steps of the technique were identified and described descriptively. The decision-making process was described as a separate step in the technique.
Technique:
After having established pneumoperitoneum and ports placement, the source of bleeding is identified and controlled. Systematic inspection of intraperitoneal and retroperitoneal organs is done. In the case of multiple injuries, the hollow viscera are exteriorized via the 4–8 cm incision and extracorporeal inspection, repair, resection, and anastomosis are performed. The other part of the procedure is completed intracorporeally. Over a 2-year period, 23 patients were managed with LAA, 13 patients with stab wounds, and 10 patients with gunshot wounds. Commonly performed procedures were hollow viscera repairs, resections, and anastomoses. There were neither missed injuries nor conversion among patients managed with LAA.
Conclusion
: The LAA is underutilized for PAT. This technique can be successfully used as a diagnostic and therapeutic tool in the management of stable patients. It offers the advantages of minimally invasive surgery and the speed and versatility of an open procedure.
Introduction
L
Despite the evolution of equipment and improvement in the laparoscopic technique, its therapeutic role in trauma is still debated. A recent systematic review reports the rate of therapeutic laparoscopy (TL) at 13.8%. 1 However, Choi and Lim reported 83% of TL. 3 TL demands adequate technical support and high performance by the trauma team. In some technically challenging cases, and where advanced laparoscopic skills are lacking, the laparoscopic-assisted approach (LAA) may be used.
The aim of this study was to describe the laparoscopic-assisted technique in the management of stable patients with PAT.
Methods
The LAA was adapted to the trauma setting and prospectively evaluated. The perioperative setting and the standard instruments and equipment requirements were identified. The technical details of each case were discussed with the operating surgeon. The indications for the technique were established, and the distinctive steps of the technique were identified and described descriptively. The decision-making process was described as a separate step of the technique. The case illustrating the use of the technique was presented, and our experience with LAA in a trauma setting was summarized.
The study was approved by the Medunsa Research and Ethics Committee of the University of Limpopo and the authorities of Dr. George Mukhari Academic Hospital. Written consent for the laparoscopic procedure with possible laparoscopic-assisted or conversion to open procedure was obtained from all patients.
Equipment
The camera should provide good visualization with two viewing screens for a surgeon and an assistant. The 30° telescope is preferred. The instruments include two atraumatic bowel graspers, Maryland dissector, laparoscopic scissors and needle holder, liver retractor, and suction-irrigation device. Laparoscopic vascular clamps and gastrointestinal staplers should be on standby. Although diathermy is sufficient, advanced energy source devices are preferable. An adjustable operating table allows quick and safe patient position changing for gravity retraction. The laparotomy set is required for ports placement, should conversion to laparotomy be necessary.
Personnel
The trauma team consists of the following: anesthetist, anesthetic assistant, trauma surgeon, at least 1 surgical assistant, operating sister, and circulating nurse. It is crucial that the entire team be familiar with the laparoscopic procedure and equipment. The trauma surgeon assumes the leadership throughout the procedure.
During the procedure
On induction of general anesthesia, the patient's physiology is assessed. Hemodynamic, respiratory, and metabolic parameters are used to define the patient's stability. In our experience, the systolic blood pressure below 90 mmHg and the mean inspiratory pressure above 30 mmHg are the most common values used to consider laparotomy. If the patient is stable after induction of anesthesia, the team continues with laparoscopy.
Procedure
LAA follows the standard steps:
1. Access, pneumoperitoneum, and ports placement: Open Hasson technique is preferred for intraabdominal entry and establishment of pneumoperitoneum. We use carbon dioxide at a pressure of 12–15 mmHg. The camera port is placed preferably at the umbilicus. In some cases, the left upper quadrant or injury site is used, depending on the situation. Two working ports (5 or 11 mm) are placed in the right and left iliac fossae. Additional trocars may be necessary, and commonly used sites are depicted in Figure 1. 2. Quick assessment of the abdomen and bleeding control: Blood and gastrointestinal content are suctioned out to identify injury or active bleeding. Bleeding is controlled with atraumatic forceps followed by vascular clamp, clips, energy source, oversuturing, or ligation. In cases where bleeding cannot be controlled promptly, or attempts of definitive control have failed, the procedure is converted to laparotomy. 3. Systematic inspection of intraperitoneal and retroperitoneal organs: Having controlled the bleeding, the surgeon proceeds to a laparoscopic systematic examination of the intraabdominal organs.
2
The greatest challenge is the management of the small bowel (SB) and colon injuries. Usually, the SB is examined by spreading and rotating it with two atraumatic forceps. In this way, the SB is walked from the ligament of Treitz to the ileocaecal valve and back. The ascending and descending colon is mobilized to inspect its retroperitoneal portion, if indicated. We apply the lateral approach to mobilization, as retroperitoneal hematoma makes appreciation of the anatomy more difficult. Such an inspection is accurate and is performed within reasonable time. 4. Decision to proceed with LAA: Isolated injuries may be repaired intracorporeally. But laparoscopic management of multiple bowel injuries, such as those sustained from gunshot and stab wounds, may unnecessarily prolong the operation. LAA is indicated in this situation. 5. Assisted access and extracorporeal process: The SB or laparoscopically mobilized colon is exteriorized via the 4–8 cm incision, extracorporeal inspection, and either repair or resection and anastomosis may be performed. The laparoscopic-assisted incision is usually placed in the midline supraumbilically, incorporating the periumbilical port site (Fig. 1). This location over the root of mesentery allows maximal exposure of the SB and the colon. The surgeon may consider placing the incision suprapubically or over the injury site, depending on the clinical situation. Care is taken not to pull too hard on the mesentery to avoid iatrogenic injury. The exteriorized multiple bowel loops may cause mesenteric compression with venous congestion that results in prolonged postoperative ileus. Iatrogenic serosal injuries may also occur. 6. Intracorporeal completion of inspection and intracorporeal therapeutic procedures: After inspection and repair, the viscera are placed back into the peritoneal cavity. The incision is temporarily closed incorporating the 11 mm port. Pneumoperitoneum is re-established for final exploration, washout, and drain placement. The assisted incision can also be used to facilitate the intraperitoneal washout. 7. Extracorporeal repair of port sites, site of injury, and assisted incision: The assisted incision, port sites, and sites of injury are closed with nonabsorbable or long-term absorbable sutures.
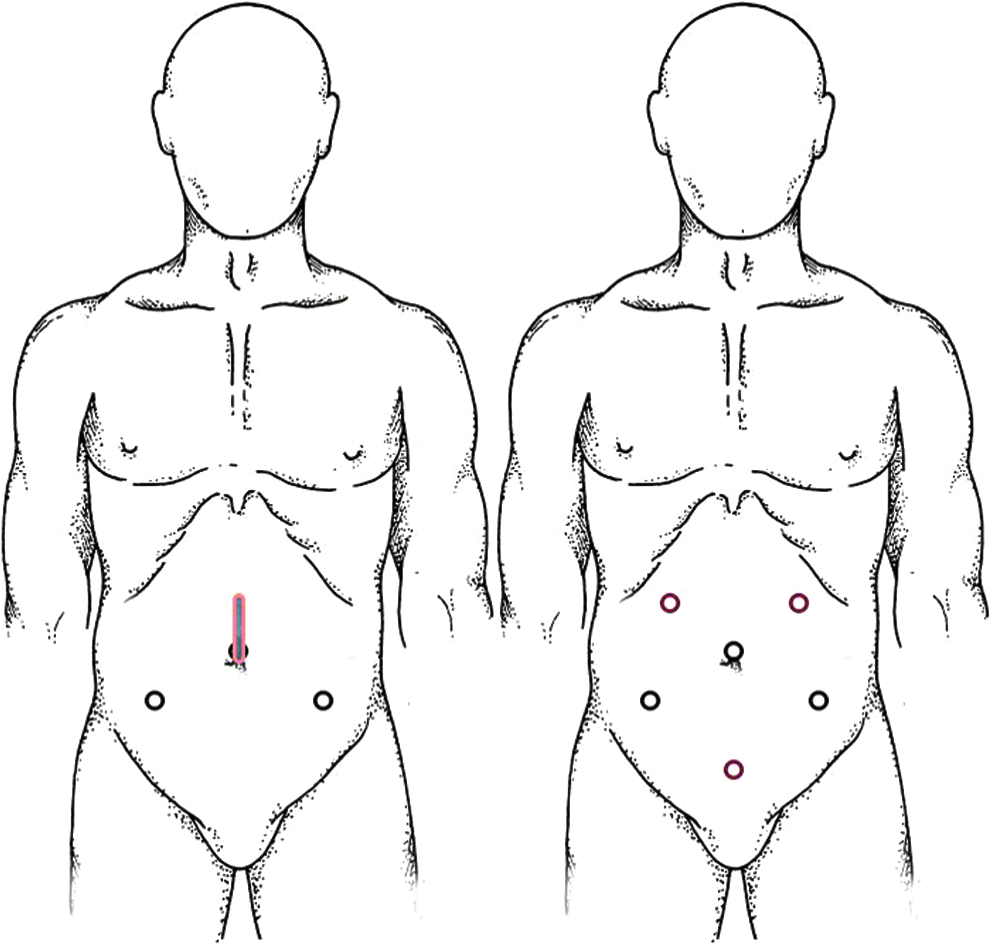
Ports and assisted access placement sites. Most common ports are in black. Additional ports are in red.
Case example and our experience with LAA
To illustrate the practical implementation of LAA, we present a stable male patient who sustained gunshot wounds (GSWs) to the left abdomen and was approached laparoscopically.
Mesenteric injury, multiple SB, and colon injuries were discovered during systematic inspection. Due to his multiple bowel injuries, the decision to use LAA was made. The 7 cm incision incorporating the periumbilical camera port was made supraumbilically in the midline for assisted access (Figs. 2 and 3). The SB was exteriorized through the incision and inspected. The mesenteric and SB injuries were repaired, and the other severely injured part of the SB was resected and anastomosed extracorporeally. The mobilized laparoscopically left colon was exteriorized through the incision, and a segmental resection and anastomosis was performed extracorporeally (Supplementary Video S1; Supplementary Data are available online at www.liebertpub.com/lap). The patient had an uneventful recovery and was discharged on postoperative day 5.
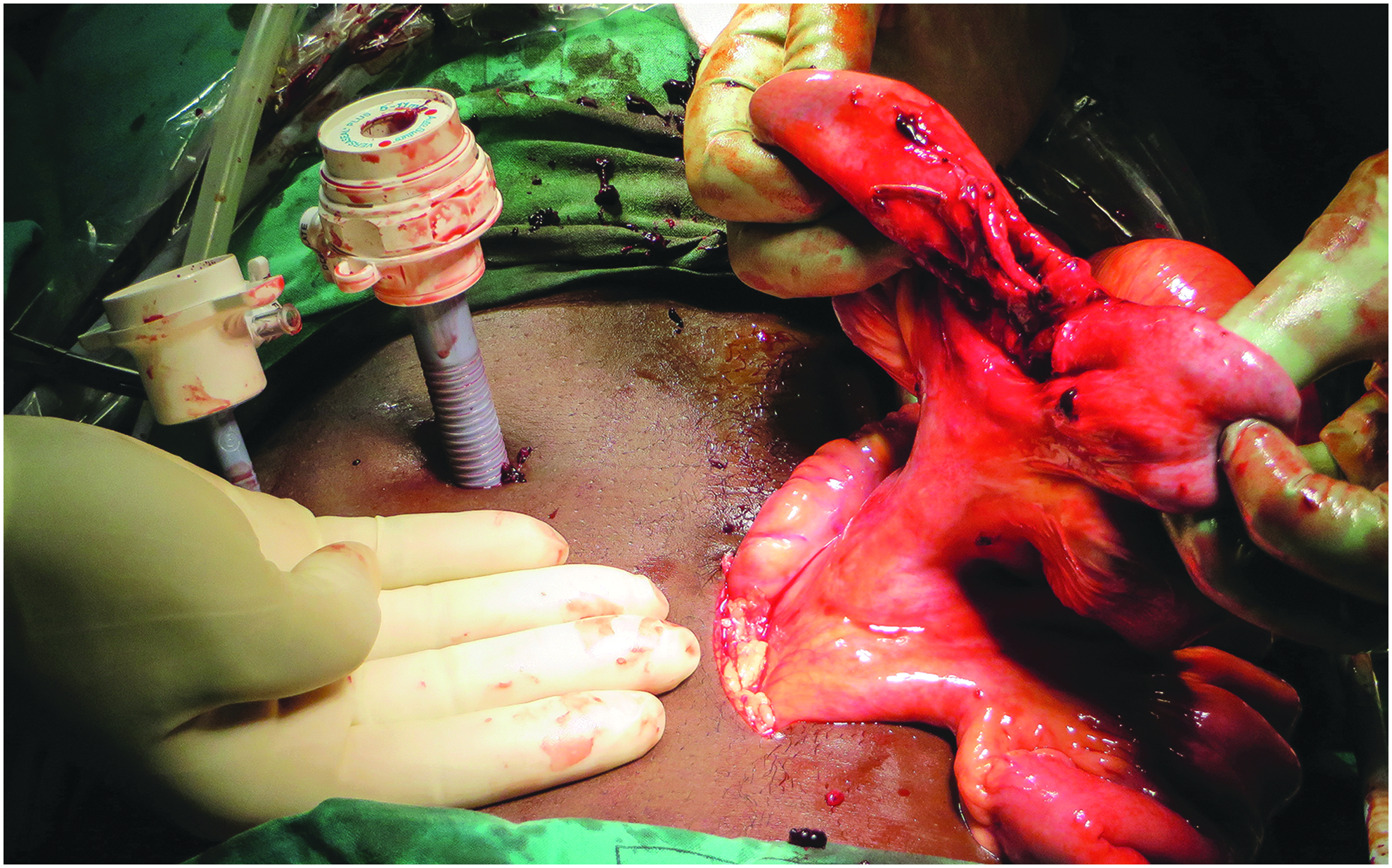
Laparoscopic-assisted approach: intraoperative view.

Laparoscopic-assisted approach: postoperative view. Black arrows, assisted incision wound; red arrow, GSW. GSW, gunshot wound.
In our initial series, 4 over a 2-year period, LAA was applied in 23 patients, 37% of all TL. Thirteen patients sustained stab wounds, and 10 patients weathered GSW. Commonly performed procedures were hollow viscera repairs, resections, and anastomoses. There were neither missed injuries nor conversions among patients managed with LAA.
Discussion
Laparoscopic inspection and therapeutic procedures for the SB and colon injuries are challenging. Many surgeons would use laparotomy as a first choice; some would attempt to repair the isolated bowel injury laparoscopically, but would switch to laparotomy for multiple bowel injuries. 5 A recent review by El-Bendary et al. described laparotomy as a preferred approach in the case of multiple bowel injuries. 6 We propose LAA as an alternative to full laparotomy. The LAA offers the advantages of minimally invasive surgery and at the same time it provides the benefits of laparotomy. Bowel injuries are managed extracorporeally as during laparotomy. The inspection and management of other intraabdominal organs that are not accessible via assisted incision are done laparoscopically. In our series, 23 patients were successfully managed with LAA and avoided laparotomy. 4
The LAA for PAT is not widely applied. Choi and Lim reported the assisted approach in 20 patients. 3 SB was exteriorized through the 34 cm incision, and extracorporeal resection and anastomosis was carried out. Lin et al. reported resection and anastomosis of SB through the assisted 3–5 cm incision in 1 patient. 5 In our experience, SB repair through the small (3–4 cm) incision is feasible; however, it does not allow complete inspection and is not suitable for colonic surgery. We also noted venous congestion of the viscera managed through the small incision. The incision of 4–8 cm allows easy exteriorization of the bowel without compressing the mesentery.
The LAA can be utilized in case of multiple bowel injuries instead of conversion to laparotomy. The lack of dexterity in intracorporeal suturing may also be considered an indication for LAA. This can be debated, as laparoscopy for trauma requires a high level of proficiency with an advanced laparoscopic technique.
In the porcine model of GSW with multiple SB injuries, the fully laparoscopic technique for isolated injuries and LAA for multiple injuries were compared with laparotomy and showed a significant reduction in the length of incision (5.27 cm versus 15.73 cm) as well as an average recovery period for bowel function. The vital appearance was improved, and patients resumed food intake earlier after laparoscopy. Although the time to diagnosis was longer in the laparoscopy group, the therapeutic time was not statistically different. 7
In the published literature, LAA for management of PAT is rarely reported and is not compared with fully laparoscopic procedures or with laparotomy. LAA was compared with laparotomy in elective colorectal surgery. It was not inferior to laparotomy and was associated with a statistically significant smaller incision length (6 cm versus 18 cm), a shorter hospital stay, and decreased analgesics requirement. 8
Conclusion
The LAA is a safe procedure for PAT. It can be successfully used as a diagnostic and therapeutic tool in the management of stable patients. It offers the advantages of minimally invasive surgery and the speed and versatility of an open procedure. Further studies are needed to confirm its role in the management of patients with PAT.
Footnotes
Acknowledgments
Study conception and design (M.K. and O.M.); literature search, data collection (O.M.); data analysis, data interpretation (M.K. and O.M.); article preparation (O.M.); critical review and revision of the article (M.K. and C.A.); and mentoring throughout the article preparation (M.K.).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.