
Abstract
Abstract
Background:
Patients with gastroesophageal reflux disease (GERD) also frequently suffer from concomitant hiatal hernia. It has been described that a preoperative hiatal hernia of ≥3 cm is associated with a more than threefold relative risk for reflux symptom recurrence after fundoplication without mesh reinforcement. In this report, we describe our experience with the implantation of dual-sided composite PTFE/ePTFE meshes in a tension-free fashion during laparoscopic antireflux surgery (LARS).
Methods:
A prospective database containing data of all patients undergoing LARS and hiatal hernia repair with mesh implantation from January 2009 until December 2014 was interrogated. Ten patients with preoperative esophageal high resolution manometry and 24-hour pH impedance monitoring because of symptoms suggestive of GERD who received hiatal repair using dual-sided meshes in inlay technique were identified and included in this analysis.
Results:
There were no conversions to open surgery in the study group. Median operative time was 138 minutes (interquartile range Q1–Q3: 119–151 minutes) and average length of postoperative stay was 3.5 days (interquartile range Q1–Q3: 2.3–4.0 days). During a median follow-up period of 43.3 months (interquartile range Q1–Q3: 18.9–47.1 months), no redo operations had to be performed. Noteworthy, 2 patients complained about dysphagia (20%) during follow-up, but symptoms resolved after endoscopic interventions.
Conclusions:
Tension-free inlay repair of large hiatal hernias using dual-sided composite PTFE/ePTFE meshes during LARS provides promising results. It provides satisfactory symptom relief and prolonged control of GERD. Further studies to validate its efficiency in a larger collective are needed.
Introduction
T
During antireflux surgery and after reestablishment of a newly created barrier at the esophagogastric junction by fundoplication, reduction of the hiatal defect and crural approximation is of paramount importance to prevent recurrent herniation. This can either be achieved by direct crural closure and/or using prosthetic materials. The intent behind implantation of mesh grafts is to reduce the tension on the hiatal crura especially in those patients who suffer from poor character of the crural musculature. In addition, one has to bear in mind that hiatal hernias >3 cm at original operation represent predictors for anatomic failure 3 and are consequently associated with a more than threefold relative risk for reflux symptom recurrence after fundoplication without mesh. 4 During long-term follow-up, the use of a mesh has shown to significantly reduce the rate of postoperative intrathoracic wrap migration or hernia recurrence with a very low incidence of mesh-related complications. 5 In a systematic review about mesh in laparoscopic large hiatal hernia repair, Furnée and Hazebroek 6 also reported low complications related to mesh (<1%). Recently, a meta-analysis of randomized controlled trials comparing suture cruroplasty and prosthetic hiatal herniorraphy for large hiatal hernia described comparable complication rates for both groups. 7 However, one must not forget that mesh implantation can be associated with complications such as dysphagia, migration, shrinkage, infection, and erosion into the esophagus or adjacent structures.
We herein report our experience with the implantation of dual-sided composite PTFE/ePTFE meshes during Nissen fundoplication in patients with symptomatic GERD suffering from concomitant type I hiatal hernias of at least 3 cm.
Materials and Methods
Patients
A prospective database containing data of all patients undergoing laparoscopic antireflux surgery (LARS) for symptomatic GERD proven by manometry and pH-metry and concomitant hiatal hernia repair with mesh implantation was retrospectively reviewed to identify all patients who had undergone surgical correction of large type I hiatal hernias (>3 cm) by tension-free inlay repair using dual-sided composite PTFE/ePTFE meshes. Exclusion criteria were previous fundoplication and confirmed esophageal motility disorders. In addition, patients with a history of any kind of esophageal or gastric surgery were not included in this analysis. From January 2009 until December 2014, 380 patients had undergone surgical treatment of symptomatic GERD. Ten patients were identified who fulfilled the above-mentioned inclusion criteria. The date was chosen to ensure a minimum 12-month follow-up.
Preoperative evaluation
Besides esophageal high resolution manometry and 24-hour pH impedance monitoring, all patients underwent esophagogastroduodenoscopy. In addition, a detailed history was taken from all patients and they were asked to answer a standardized questionnaire about upper gastrointestinal symptoms before ambulatory reflux monitoring and high resolution manometry as described previously.8,9 Patients were questioned regarding the presence of upper gastrointestinal symptoms, namely heartburn, epigastric pain, regurgitation, respiratory symptoms, odynophagia, globus sensation, dysphagia, flatulence, chronic cough, hoarseness, bronchitis, and bronchial asthma. All patients' medication was also assessed, with a special focus on proton-pump inhibitors.
All patients underwent esophageal manometry by measuring (InSIGHT™; Sandhill Scientific, Inc., Colorado) resting and end-expiratory pressure of the lower esophageal sphincter. Total and intra-abdominal lengths of the lower esophagus sphincter were measured. Manometry data of swallow-induced contractions were assessed in the proximal, middle, and distal part of the esophagus using 10 liquid swallows of 5 mL at 30 second intervals.
Esophageal acid exposure was assessed by 24-hour pH monitoring using a combined pH and impedance portable system (Sandhill Scientific, Inc.). Proton-pump inhibitors and other medications with possible confounding interactions were discontinued for at least 10 days prior investigations. A single-use catheter was passed transnasally and positioned 5 cm proximal to the lower esophageal sphincter to measure intraluminal pH. Gastroesophageal reflux activity was monitored for 20 to 23 hours while patients were instructed to pursue their routine daily activities and adhere to their usual dietary habits. Patients recorded mealtimes and times spent in supine position. DeMeester's score was calculated from the derived data and values above 14.7 were considered as increased acid reflux.
Surgical technique
All procedures were carried out laparoscopically. Mobilization of the esophagogastric junction was performed following incision of the phrenoesophageal ligament. After the stomach could be restored completely into the abdominal cavity again, the distal esophagus located in the mediastinum was dissected free from surrounding adhesions. This dissection was felt necessary to achieve a tension-free intra-abdominal esophagus length of at least 3 cm. During this procedure, special care was taken not to open the pleurae. Following these steps, the complete circumference of the hiatus can be displayed. By elevating the esophagus in a left cephalad direction, a window behind the esophagus is visualized. Closure of the enlarged hiatus was achieved using a dual-sided composite PTFE/ePTFE mesh as it encourages tissue ingrowth to repair the defect.10,11 Meshes were cut and trimmed properly and a notch was created for the esophagus but avoiding broad direct contact. An example of mesh configuration is given in new Figure 1. They were placed into the hiatal space using an inlay technique and fixed on both crurae using interrupted polypropylene 2-0 sutures but no cruroplasty has been performed previously. As a consequence, considerable tension on the crurae by performing primary closure of the defect could be avoided. We adhered to the proposed concept of Wassenaar et al. who advocate leaving a small space between the edge of the mesh and the esophageal wall to avoid excessive contact of the mesh with the esophagus. 12 Afterward, the fundus was mobilized by dissection of short gastric vessels using a harmonic scalpel. All patients received a complete 360° floppy Nissen fundoplication with a short wrap using two or three interrupted polypropylene 2-0 sutures. The first stitch that is located around 2 cm above the esophagogastric junction is slightly passed through the esophageal musculature. The operations were carried out by one of the authors (J.M.).
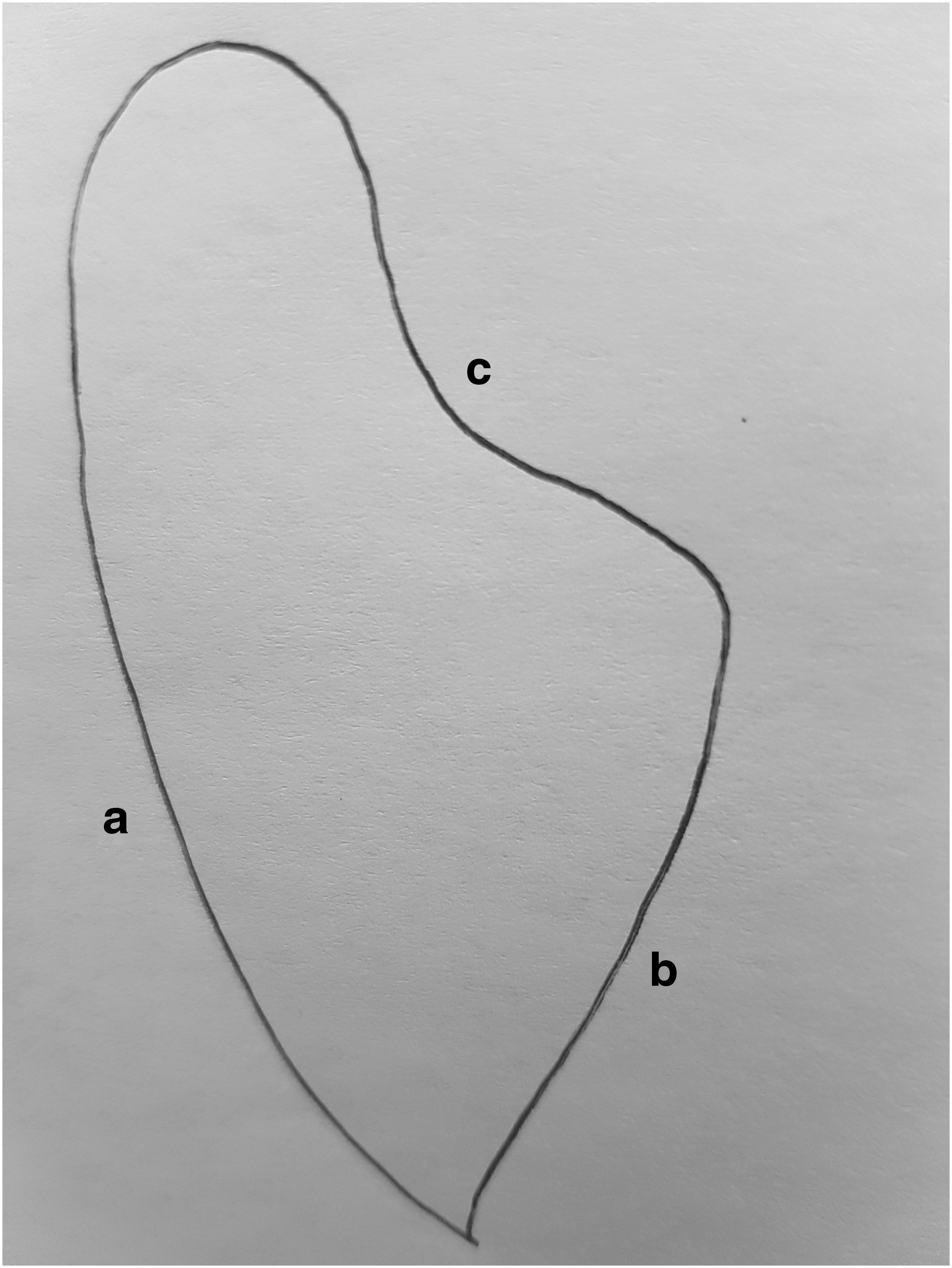
Mesh design. (a) Edge facing right crural pillar; (b) edge facing left crural pillar; (c) recess for the esophagus.
Follow-up
Patients were contacted at 1, 3, and 6 months in addition to 6 monthly thereafter with the last contact time in July 2015. Symptom recurrence was defined as relapse of heartburn and/or regurgitation more frequently than once a week and/or the need for proton pump inhibitor treatment to control reflux symptoms. Dysphagia was considered significant in case swallowing difficulties were severe enough that the patient accepted either upper gastrointestinal endoscopy with or without dilatation. 13
Results
Demographics and baseline characteristics of patients are presented in Table 1. In addition, data regarding durations of GERD symptoms with and without deterioration in quality of life are given. Four patients (40%) were on double dose proton pump inhibitor (PPI) therapy at the time of surgery. Noteworthy, 60% of patients had a preoperative hiatal hernia size of ≥4 cm. Overviews of upper gastrointestinal GERD-related symptoms are given in Table 2. The most frequent complaints (80%) were heartburn and belching in upright position. Data from esophageal manometry and 24-hour pH-metry including DeMeester's score are presented in Table 3.
Q1–Q3 indicates interquartile range.
BMI, body mass index; GERD, gastroesophageal reflux disease; PPI, proton pump inhibitor.
Q1–Q3 indicates interquartile range.
There were no conversions to open surgery in the study group. Mean operative time was 131 minutes (median: 138 minutes, interquartile range Q1–Q3: 119–151 minutes). Patients were allowed to take liquids and pulpy food starting on the first postoperative day. The only postoperative complication observed within the initial hospital stay was a pneumomediastium in conjunction with bilateral pneumothoraces in 1 patient. Both entities were completely resolved after 24 hours and the patient could be discharged on the second postoperative day. The average length of postoperative stay was 3.3 days (median: 3.5 days; interquartile range Q1–Q3: 2.3–4.0 days).
During a mean follow-up period of 34.6 months (median: 43.4 months; interquartile range Q1–Q3: 18.9–47.1 months), no redo operations had to be performed. Noteworthy, 2 patients complained about dysphagia (20%) during follow-up. Once, it was observed within 30 days postoperatively but completely resolved after diagnostic endoscopy. The second patient suffering from dysphagia experienced temporary symptom relief after balloon dilatation, which had been performed 6 months after the laparoscopic operation. Another 4 weeks later, the 71-year-old woman had to undergo a repeat endoscopy including dilatation using the Starck apparatus. Afterward, no recurrence of symptoms has been observed.
Discussion
LARS has proven to be effective in treating patients suffering from GERD being refractory to conservative measures. Compared to earlier years in which only conventional open surgical fundoplication was available, the minimal invasive laparoscopic approach is associated with reduced postoperative pain and morbidity. In addition, shortened length of hospital stay and recovery in conjunction with sufficient symptom control led to an increase in referral of GERD patients for surgical treatment.
Several causes of failure after LARS have been described including the too-tight or too-long fundoplication and disruption of the wrap. Another failure pattern represents the intrathoracic migration of the fundus wrap. Hunter et al. reported in their series of 100 consecutive patients who had undergone fundoplication revision that transdiaphragmatic herniation of the fundoplication was responsible for 84% of revision procedures. 14 The authors concluded that thorough esophagogastric mobilization is essential to reduce laparoscopic fundoplication failure.
Another key role in prevention of GERD symptom recurrence is the secure diaphragmatic closure of the hiatal defect. Possible reasons for inadequate crural closure are excessive tension following primary sutured repair leading to disruption or poor character of the crural musculature.
To take this into account, meshes can be placed on the esophageal hiatus to decrease the tension on one hand and reinforce the hiatal crurae on the other hand. As early as 1999, Carlson et al. 15 reported that the use of mesh reinforcement resulted in a lower rate of recurrent herniation compared to primary repair alone. Soricelli et al. 5 also concluded in their long-term follow-up analysis that the use of a mesh proved to be effective in reducing the rate of postoperative intrathoracic wrap migration or hernia recurrence. Regarding the constitution of the mesh, absorbable and nonabsorbable ones are available. An internet-based survey tool on the use of mesh for hiatal hernia repair by members of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) revealed that absorbable meshes are most commonly used (67%). 16 Nevertheless, biomaterial tended to be associated with failure, 17 whereas nonabsorbable meshes tended to be associated with complications affecting the esophagus. These include intraluminal mesh erosion, fibrosis, and esophageal stenosis or stricture. Management of these complications is complex and may ultimately lead to (partial) gastrectomy or esophagectomy.
In an analysis of severe complications following laparoscopic mesh hiatoplasty, it was concluded that composite meshes should be preferred to increase safety. 18 These meshes generate tissue ingrowth on the porous diaphragmatic side inducing local fibrosis and subsequent reinforcement.10,11 To prevent possible adhesions to visceral organs, the ePTFE layer is oriented toward the abdominal cavity leading to neomesothelialization and therefore separation from the adjacent esophagogastric structures. The above-mentioned effects could be proven in an animal model of large hiatus hernia. 19 Several human studies analyzing the outcomes following laparoscopic repair of large hiatal hernias with dual-sided PTFE/ePTFE mesh reinforcement are available. Hazebroek et al. 20 concluded that this type of hiatal closure represents a durable repair in long-term endoscopic follow-up. Recently, a series with a mean follow-up period of 65 months has reported symptomatic improvement and patient satisfaction in 88% of patients. 21 Similar results are described by Chilintseva et al. 22 who summarized that the addition of double-sided mesh reinforcement in surgical repair of large hiatal defects is safe and beneficial in terms of quality of life. Other authors also concluded that this approach results in satisfactory symptom control 23 and represents an effective and safe procedure. 24 No signs of mesh erosion, ulceration, or perforation had been described in these studies, which overview a total of more than 160 patients.20–24 Nevertheless, transmural gastric mesh migration of dual-sided meshes has been occasionally observed.
Repair of large hiatal hernia should be effective and durable. Closure of the hiatal defect can either be achieved by direct suture or by mesh implantation of different types. However, equipoise exists regarding whether mesh cruroplasty improves symptomatic outcomes compared with suture repair as recently stated by Tam et al. 27 A meta-analysis and European survey study analyzing almost 700 patients summarized that synthetic and biological meshes reduce rates of recurrence compared to direct suture repair, with synthetic meshes proving most effective. 26 Another recently published article dealing with the issue of mesh-augmented versus standard crura repair during long-term outcome concluded that crural reinforcement with a synthetic mesh is safe and may protect from early anatomical recurrence. 27 However, the use of prosthetic material during large hiatal hernia repair cannot be endorsed routinely and the decision for the placement of mesh needs to be individualized based on the operative findings and the surgeon's recommendation. 7
The limitations of this study include its retrospective design, the small number of cases, and the manageable duration of follow-up. However, the presented data regarding satisfactory symptom relief and prolonged control of GERD warrant further investigations to validate its efficiency in a larger collective.
Conclusion
Defect closure of large hiatal hernias using dual-sided composite PTFE/ePTFE meshes in a tension-free fashion during LARS is safe and effective. It provides satisfactory symptom relief and prolonged control of GERD but postoperative dysphagia still represents an important issue. Early dysphagia occurring within 30 days postoperatively resolved after diagnostic upper gastrointestinal endoscopy. The second patient suffering from dysphagia could be treated successfully with endoscopic interventions without the need of reoperation. The presented data are promising and together with the good tolerability of the mesh warrants further studies to validate its efficiency in a larger collective.
Footnotes
Disclosure Statement
No competing financial interests exist.