
Abstract
Abstract
Background:
When hepatocellular carcinoma (HCC) was located in segment 2 (S2), segment-oriented hepatectomy was more beneficial than left lateral sectionectomy as this type of anatomical resection preserved the volume of the nontumor-bearing segment. Herein, we presented 2 cases (1 with video) of laparoscopic anatomical S2 segmentectomy by the Glissonian approach.
Methods:
The first patient was a 69-year-old woman, who had an incidentally detected liver nodule on abdominal ultrasound for systemic surveillance for her breast cancer. The preoperative liver function was Child–Pugh class A. Abdominal computed tomography showed a 2 cm low attenuating lesion in S2. Contrast magnetic resonance imaging (MRI) showed the same lesion with features more suggestive of HCC. In view of the inconclusive imaging findings, a needle biopsy was performed and it confirmed the diagnosis of HCC. The second patient was a 57-year-old man with hepatitis B and Child–Pugh class B liver cirrhosis. He had an enlarging nonenhancing liver nodule in S2 noted on MRI. Laparoscopic anatomical S2 segmentectomy was performed for these 2 patients.
Results:
The operative time for the first and second patients was 240 and 185 minutes, respectively. The respective estimated intraoperative blood loss was 50 and 250 mL and no transfusion was necessary. The patients were discharged on the fourth and fifth postoperative day without any complications, respectively.
Conclusion:
This study showed the feasibility of performing a laparoscopic S2 segmentectomy by the Glissonian approach.
Introduction
S
Methods
Case 1
A 69-year-old woman was admitted for an incidental 2 cm hypoechoic liver nodule detected on abdominal ultrasound. She had history of carcinoma of the breast with breast-conserving treatment and radiotherapy performed 5 years ago and was then put on letrozole. She also had history of diabetes mellitus. Physical examination was unremarkable. Laboratory studies showed negativity for hepatitis B and C viral markers and an elevated alpha fetal protein level of 44.4 IU/mL. The preoperative liver function tests were graded as Child–Pugh class A. Contrast computed tomography (CT) showed a 2.5 cm low attenuating lesion with peripheral enhancement in segment 2 of the liver, which could be a metastasis, intrahepatic cholangiocarcinoma, or HCC. Magnetic resonance imaging (MRI) of the liver with contrast then showed a 2 cm mass in S2 with features more suggestive of HCC. An ultrasound-guided liver biopsy was performed, which confirmed the diagnosis of HCC. We then performed a laparoscopic anatomical S2 segmentectomy.
Operative technique
Under general anesthesia, the patient was placed in the lithotomy position. A CO2 pneumoperitoneum was created through a 12 mm umbilical port, and the intraabdominal pressure was maintained below 12 mmHg. Four additional ports (one 12 mm port, one 10 mm port, and two 5 mm ports) were placed as shown in Figure 1. A flexible laparoscope (Olympus, Tokyo, Japan) was used. IOUS was performed to confirm the location of the tumor and its relationship with the adjacent structures. The left lateral section was mobilized. The Glissonian pedicle to S2 was isolated with meticulous dissection, which was then temporarily clamped. The ischemic margin of S2 was marked using electrocautery. Transection of the liver parenchyma was performed. The superficial hepatic parenchyma was transected using Harmonic Scalpel® (Ethicon Endo-Surgery, Inc., Cincinnati, OH), while the deeper portion of the parenchyma was transected using laparoscopic CUSA® (Valleylab, Boulder, CO). The hepatic vein for S2 entering the left hepatic vein was isolated and divided between 5 mm Hem-o-lock™ clips (Weck Teleflex Medical, Research Triangle Park, NC). Further dissection was performed using CUSA, exposing the left hepatic vein. After completion of the parenchymal dissection, the only remaining structure attached to the liver remnant was the S2 Glissonian pedicle. It was then divided between Hem-o-lock clips. Once the resected specimen was completely divided, it was extracted through an extension of the suprapubic scar from previous operation in a vinyl bag. Hemostasis was achieved and fibrin glue (Greenplast®; Green Cross Corp., Seoul, Korea) was applied on the raw surface. After irrigating the surgical field, a silastic drain was placed and the wound was closed in layers (Fig. 2 and Video 10 ).

Position of the trocars for patient 1.

Technical aspects of laparoscopic segment 2 (S2) segmentectomy.
Results
The operative time was 240 minutes. The estimated intraoperative blood loss was about 50 mL and intraoperative blood transfusion was not needed. On the first postoperative day, the levels of aminotransferase (AST) and alanine transaminase (ALT) were slightly elevated (AST, 119 IU/L; ALT, 107 IU/L) and they became normalized on the fourth postoperative day (AST, 28 IU/L; ALT, 60 IU/L). Postoperative pathology analysis confirmed a 2.1 × 1.9 × 0.9 cm HCC with a 4 mm tumor-free resection margin. The patient was discharged on the fourth postoperative day without any complications.
Case 2
A 57-year-old man was a hepatitis B carrier receiving adenovir and lamivudine. He was noted to have deranged liver function 4 years ago. Physical examination was unremarkable. Preoperative liver function tests were graded as Child–Pugh class B with a normal alpha fetal protein level (4.2 IU/mL). Triphasic contrast CT scan of the liver showed 1.6 cm lesion in segment 8/4 and another 3 cm nodule in segment 2. MRI of the liver showed multiple dysplastic nodules in both lobes of the liver with a 3 cm dominant nodule in the left lateral section and another 2 cm high-grade dysplastic nodule in S4. In view of the multifocal disease, a combination of transarterial chemoembolization (TACE) and radiofrequency ablation (RFA) to the S4 lesion was performed. Regular surveillance in a 3-monthly interval with contrast CT or MRI of the liver did not reveal any recurrence in the ablated region. There was no evidence of lipiodol retention in the otherwise static nonenhancing lesion at S2. This S2 lesion was thus regarded as a dysplastic nodule for close monitoring. In May 2014, the surveillance CT scan showed an enlarging nodule in S5 from 1.8 to 3.7 cm. Another course of combined TACE and RFA to the S5 lesion was performed. In the MRI scan at 3 months after the second RFA, the nonenhancing lesion at S2 had increased in size from 3 to 4 cm (Fig. 3). There were no other arterial enhancing lesions in the liver. We then performed a laparoscopic anatomical S2 segmentectomy.
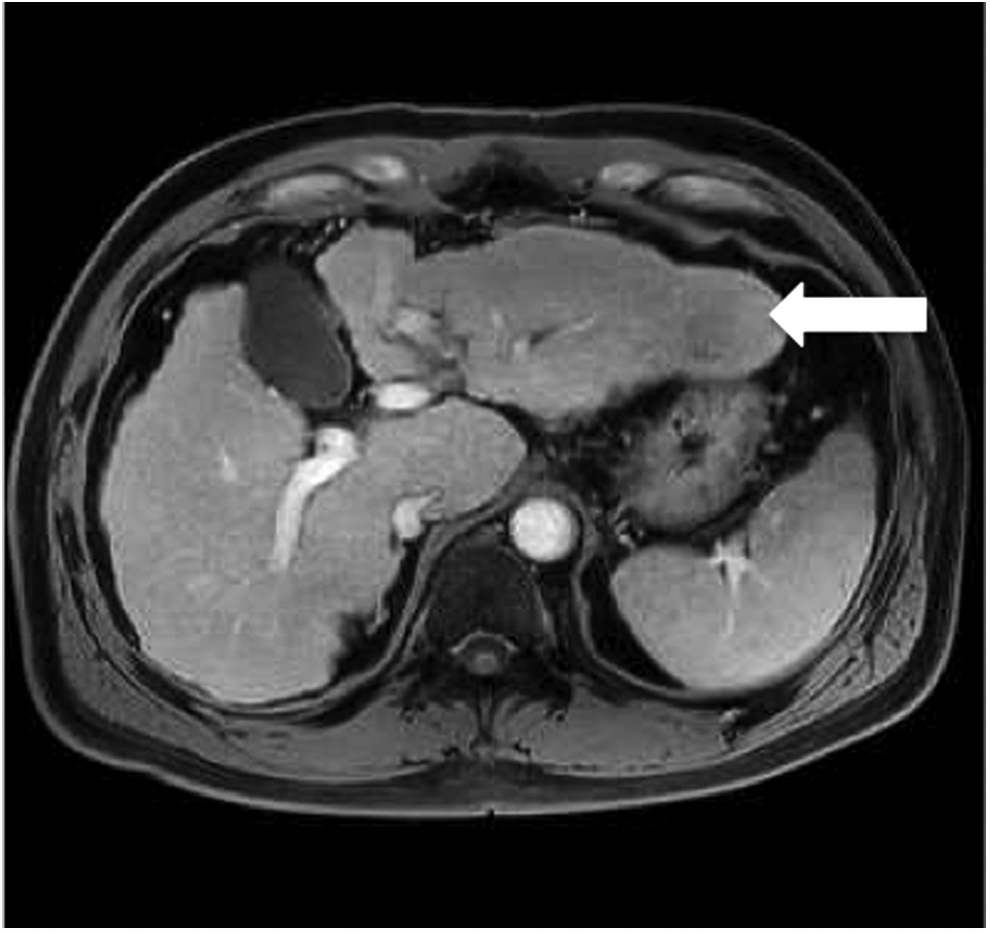
Magnetic resonance imaging of liver for patient 2.
Operative techniques
The patient was prepared and positioned as in Case 1. Six ports were inserted as shown in Figure 4. The left lateral section was mobilized and IOUS was performed. The Glissonian pedicle of S2 was isolated and controlled as already described. Intermittent Pringle maneuver was applied for two cycles of 15 minutes occlusion to reduce blood loss. The method of parenchymal transection and hemostasis was similar as in Case 1.

The trocars position of patient 2.
Results
The operative time was 185 minutes. The estimated intraoperative blood loss was about 250 mL and intraoperative blood transfusion was not needed. On the first postoperative day, the levels of AST and ALT were slightly elevated (AST, 141 IU/L; ALT, 135 IU/L) and they normalized on the fifth postoperative day (AST, 37 IU/L; ALT, 71 IU/L). Postoperative pathology analysis confirmed a 4.1 × 3.9 × 3.5 cm HCC with a 17 mm tumor-free resection margin (Fig. 5). The patient was discharged on the fifth postoperative day without any complications.
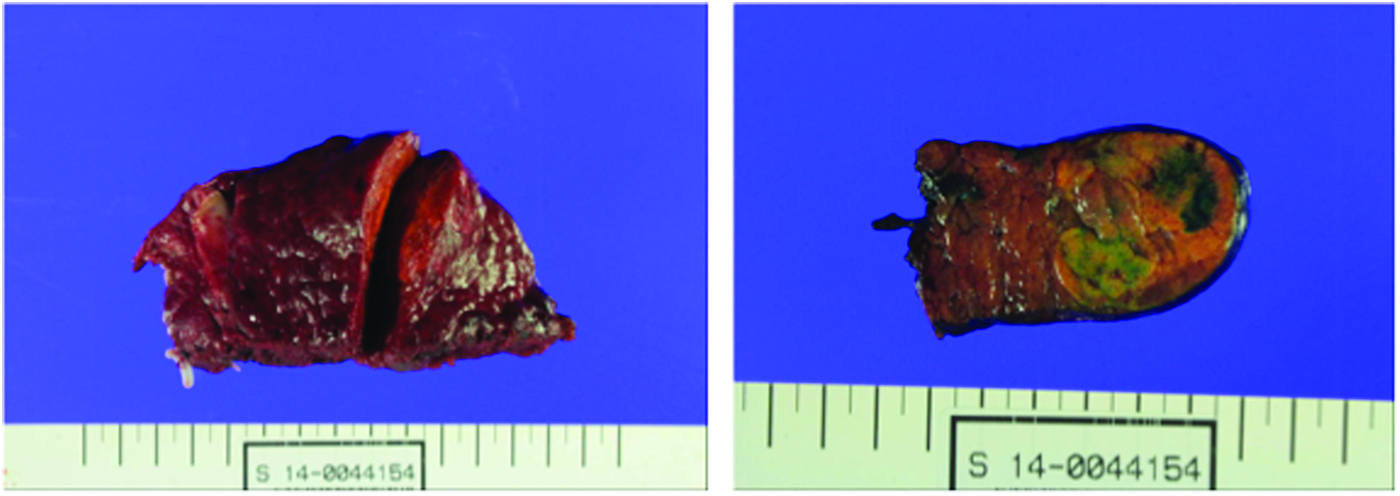
Photograph of the resected specimen in patient 2.
Discussion
Laparoscopic liver resection has evolved over the last few decades. Systemic reviews have shown that laparoscopic liver resection was associated with less blood loss, less wound pain, and shorter hospital stay. The resection margin and the oncological outcomes in terms of overall and disease-free survival were comparable with open liver resection.8,9,11,12 These benefits were also shown in patients with cirrhosis and HCC.13,14
Among the 950 laparoscopic liver resections performed from January 2003 to December 2015 in our center, we have done two laparoscopic anatomical S2 segmentectomies for 2 patients with HCC in S2. Although there was ongoing debate on the superiority in anatomical resection over nonanatomical resection,5–7,15–18 anatomical resection was still the preferred surgical option whenever possible as it followed the oncological principle by removing all the liver parenchyma that was potentially involved by tumor spreading into the segmental portal venous branch. Furthermore, the resection margin could be more easily secured in anatomical resection.5–7 Anatomical resection could be performed in both major resection and minor resection. We have reported on the safety and feasibility for laparoscopic monosegmentectomy for S4 and S519–21 and there are reports on laparoscopic segmentectomy for S7 and S8 in the literature as well.22,23 We could perform either S4a or S4b anatomical resection for lesion located in S4. 21 When the tumor was located in S2, laparoscopic left lateral sectionectomy would be the usual choice of procedure. However, patients with HCC often had underlying liver cirrhosis. Laparoscopic S2 segmentectomy carried the additional advantage of preserving the nontumor-bearing liver parenchyma and thus decreasing the likelihood of postoperative liver insufficiency in a cirrhotic liver with small right lobe.
To perform an anatomical resection, identification of the intersegmental plane and maintaining the proper transection plane were paramount to ensure a safe resection margin and to safeguard the vascular structures and biliary drainage of the liver remnant. The Glissonian pedicle approach has been shown to be useful in this regard.24,25 In our center, meticulous dissection was performed to isolate the Glissonian pedicle, which was temporarily clamped. The ischemic demarcation line was then demonstrated and served as the guide for the transection. Furthermore, the inflow control achieved by the Glissonian pedicle approach could reduce intraoperative blood loss.24–26
Conclusion
This study demonstrated the feasibility and the technical aspects of laparoscopic anatomical S2 segmentectomy. This surgical option offered the benefits of parenchyma-preserving anatomical resection with decreased risk of posthepatectomy liver insufficiency. Careful dissection and control of the Glissonian pedicle made laparoscopic anatomical monosegmentectomy possible as in open surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.