
Abstract
Abstract
Background:
There are many ways to treat focal hyperhidrosis, including surgeries for palmar and axillary hyperhidrosis. However, doctors and patients tend to be reluctant to perform surgery for plantar hyperhidrosis due to misconceptions and prejudices about surgical treatment. In addition, few studies have reported the outcome of surgeries for plantar hyperhidrosis. Therefore, the objective of this study was to determine the outcome (early and late postoperative satisfaction, complication, compensatory hyperhidrosis, recurrence rate, and efficiency) of surgical treatment for plantar hyperhidrosis.
Materials and Methods:
From August 2014 to October 2015, lumbar sympathetic block (LSB) was performed in 82 patients with plantar hyperhidrosis using clipping method. Limited video-assisted LSB was performed using 5 mm ligamax-clip or 3 mm horizontal-clip after identifying L3-4 sympathetic ganglion through finger-touch and endoscopic vision.
Results:
Of the 82 patients, 45 were male and 37 were female. Their mean age was 26.38 years (range, 14–51 years). Mean follow-up time was 6.60 ± 3.56 months. Mean early postoperative satisfaction score was 9.6 on the 10th day postoperative evaluation. At more than 1 month later, the mean late postoperative satisfaction score was 9.2. There was no significant difference in early postoperative satisfaction score between clipping level L3 and L4/5. However, late postoperative satisfaction score was significantly better in the L3 group than that in the L4/5 group. Patient's age and body mass index did not affect the satisfaction score. However, male patients and patients who had history of hyperhidrosis operation showed higher satisfaction score than others.
Conclusion:
Limited video-assisted LSB using clip provided good results with minimal complications and low compensatory hidrosis, contrary to the prejudice toward it. Therefore, surgical treatment is recommended for plantar hyperhidrosis.
Introduction
P
Conservative treatment for plantar hyperhidrosis with anticholinergic pills, aluminum chloride lotions, iontophoresis, and botulinum toxin injections can improve its symptoms. However, conservative treatment does not provide long-term resolution. Percutaneous chemical lumbar sympathectomy and sympathicolysis have also been used to treat plantar hyperhidrosis. However, their long-term therapeutic effect is doubtful. 4
Lumbar sympathectomy is available as a surgical option for plantar hyperhidrosis patients. It was first described in 1924. It was initially utilized for occlusive vascular disease such as Buerger disease, Raynaud disease, and reflex sympathetic dystrophy. 5
Although thoracic sympathectomy has been well described as the surgical treatment for palmar hyperhidrosis and actively reported with systematic investigations, lumbar sympathectomy for plantar hyperhidrosis has become clinically feasible with widespread use only until recently due to previous fear of compensatory hidrosis and other possible complications such as retrograde ejaculation. 3 Moreover, it is believed that compensatory sweating can become worse when the effect of thoracic sympathectomy is added to the lumbar regions of the same patient. 5 Although high patient satisfaction with postoperative results has been proven in many other studies, 6 the outcome of lumbar sympathectomy remains unclear due to the lack of systematic investigation, especially in South Korea.
Lumbar sympathecotomy with endoscopic surgical technique was first described in 1973. 7 Because of little tissue-trauma with minimum perioperative morbidity, this method has been used widely as a standard surgical option. Recently, endoscopic lumbar sympathetic chain block (ELSB) with clamping method rather than nerve resection was introduced. It provides good results with minimal postoperative pain or other complications. 3 However, ELSB has cosmetic problem, resulting in three different sized (10 mm port and two 5 mm ports) port site wounds on each side. Moreover, it is hard to expect anatomical accuracy for surgical treatment with only endoscopic vision due to the more complex retroperitoneal anatomical structure compared to thorax. These can lead to prolonged operating time and recovery time with unexpected normal tissue trauma and a long-learning period for the surgeon.
The objective of this study was to determine whether limited video-assisted lumbar sympathetic block (LSB) using clipping method was a more effective surgical option compared to endoscopic lumbar sympathectomy (ELS) for primary plantar hyperhidrosis patients.
Materials and Methods
Between August 2014 and October 2015, 82 consecutive patients with plantar hyperhidrosis underwent limited video-assisted LSB using clipping method (a total of 164 procedures). According to the Hyperhidrosis Disease Severity Scale (HDSS), all patients were rated as HDSS 3 or HDSS 4 (sweating is intolerable, always interferes with daily activities 8 ) with reduced quality of life. These patients tried various conservative treatments for plantar hyperhidrosis without successful long-term effect.
Chest X-ray, electrocardiogram, and preoperative routine blood sampling were performed before surgery. Secondary hyperhidrosis such as hyperthyroidism, diabetes, and psychiatric problem were excluded from surgical indication. No patient suffered from relevant concomitant disease. All patients signed preoperative informed consent, including a very detailed discussion about the possibility of compensatory sweating, intraoperative and postoperative complications, and unexpected side effects such as the potential of sexual dysfunction. Data used in this study were collected by medical chart review, telephone interviews, and text message correspondence.
Operative technique
All operations were performed bilaterally under general anesthesia with single lumen endotracheal intubation. Patients were placed in supine position with pillow underneath their knee joint for relaxation of psoas muscle (Fig. 1). In cases of simultaneous palmar hyperhidrosis, ELS was performed after endoscopic thoracic sympathectomy (ETS). Skin mark (line) was extended from the navel to the lateral abdominal wall. About 2.5 cm skin incision was made in the lateral abdominal wall halfway between the anterior superior iliac crest and inferior rib cage margin of each side at the navel level. These could make surgeon to find the L3 vertebral body easily. 3

Position of patient.
Skin incision was carried out through forcing the scarpa's fascia down to the external oblique fascia. External oblique, internal oblique, and transveralis muscle were then continuously dissected with splitting by bovie. The transversalis muscle was separated from the peritoneum. Retroperitoneal space was opened with blunt finger dissecting movements cephalad and caudally. The surgeon should make sure that there was no peritoneal rupture.
The retroperitoneal space was extended until psoas major muscle fascia was identified. Dissection was carried out on the anterior surface of the psoas major, pushing all structures anteriorly, such as retroperitoneal fat pad and ureter by Long Kelly- peanut. Genito-femoral nerve could be observed on the psoas muscle. Care must be taken not to confuse the genito-femoral nerve with the sympathetic chain. The sympathetic chain lies over the base of the third and/or fourth lumbar vertebral body, medial to the psoas major muscle, and is covered by a capsule formed on the right side of the vena cava and on the left side of the para-aortic fat and para-nodal tissue (Fig. 2).
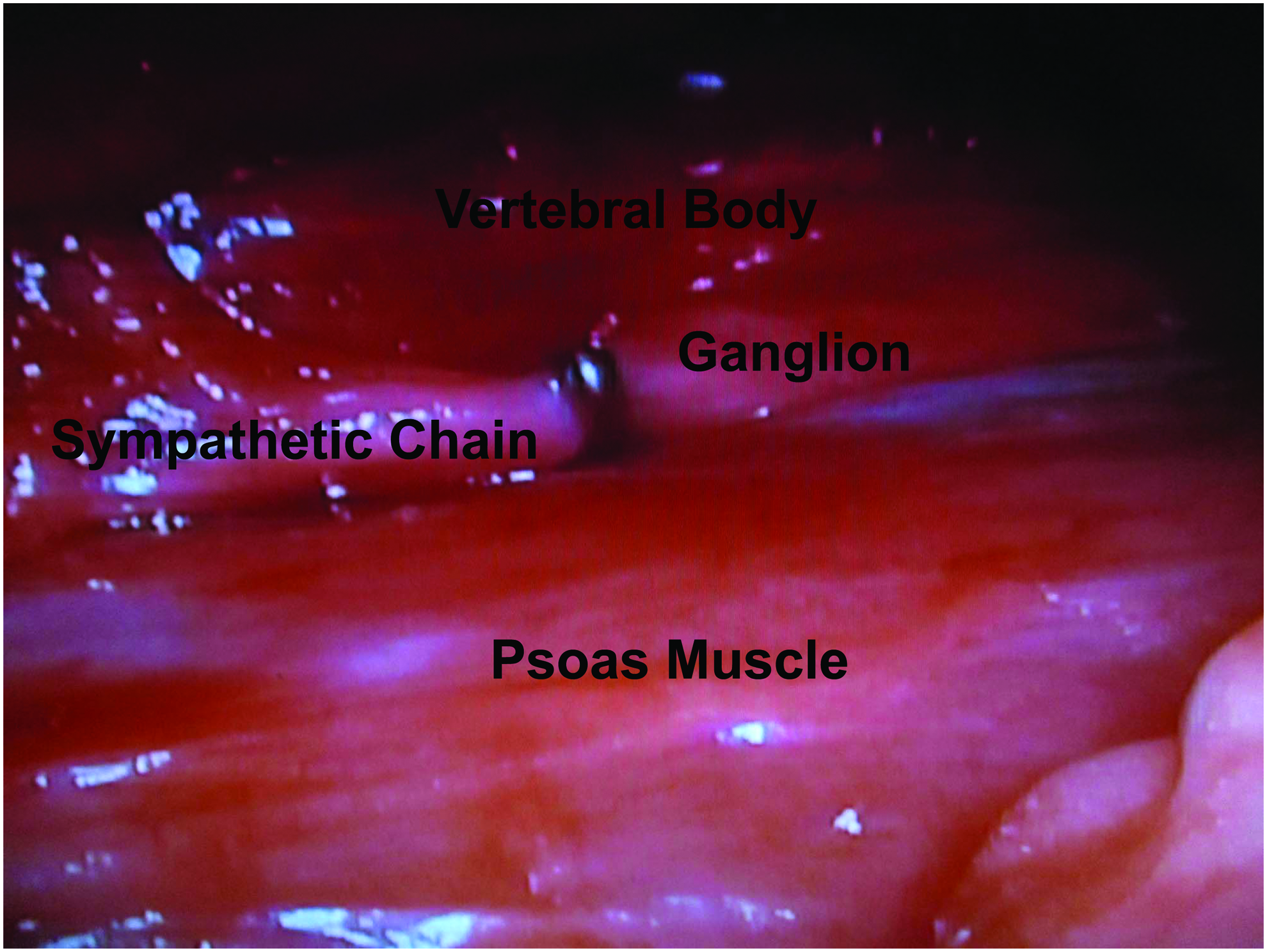
Anatomical identification of vena cava, genitofemoral N. spinal body, ganglion and chain, Psoas muscle, ureter, and reteroperitoneal fat pad.
After identifying lumbar sympathetic ganglion by finger touching and endoscopic direct vision, the sympathetic nerve was carefully dissected, dividing all the rami communicants. Then, the sympathetic chain was clamped at the level of L3–L4 using 5 mm endoscopic titanium clips (Ethicon®, LIGAMAX) or 3 mm titanium clips (Weck®, HORIZON). Anatomical variation such as the lumbar vein or big lymphatic vessels must be considered and avoided to ligation. If there was any anatomical question about the position of the sympathetic ganglion, two to three multiple clipping was performed on suspected sympathetic chain. After checking hemostasis and making sure that the clips encompassed the whole nerve by endoscopic or direct vision, the same procedure was repeated on the opposite side. The internal muscle, external muscle, and wound were closed using subcuticular stitches without placement of drains (Fig. 3). Before discharge, the level of sympathetic block by clips was confirmed on radiograph of the lumbar spine.
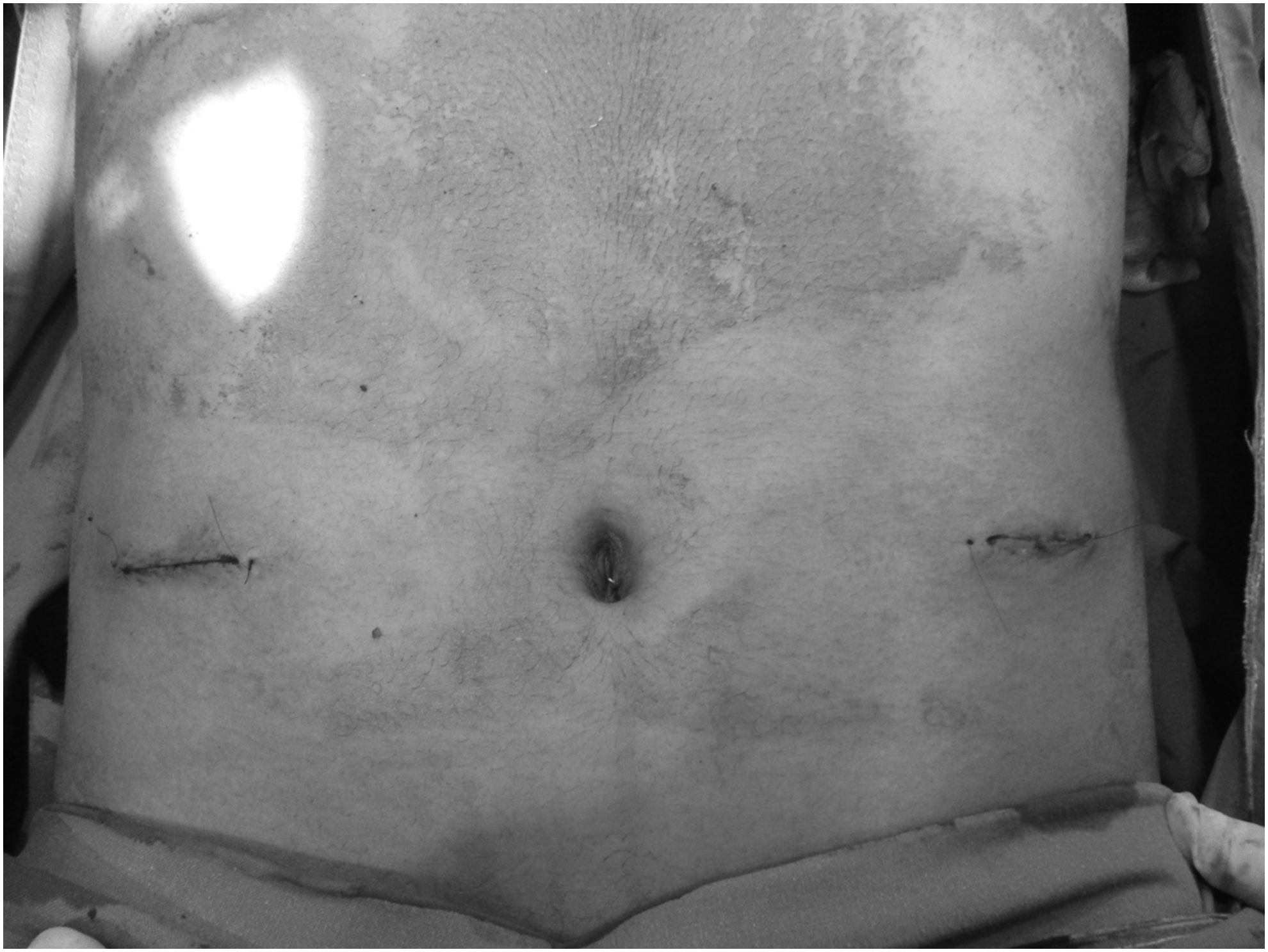
Postoperative wound.
Postoperatively, patients were given intravenous prophylactic antibiotics and nonsteroidal anti-inflammatory analgesics. They started oral diet after 5 hours. Basically, all cases in this series did not stay overnight in the hospital except special situation.
These patients were interviewed and examined after 1 and 10 days as early postoperative follow-up through outpatient monitoring in an attempt to identify their impression about the surgery (1–10 satisfaction scale) and record the development of compensatory hyperhidrosis and any side effects. Late postoperative follow-up questionnaires were given to them 1–16 months after the surgery by phone interview.
Characterization of compensatory hyperhidrosis in other regions of the body was performed by direct questions. The severity was graded as “none” (compensatory sweating is not noticeable), “mild” (compensatory sweating is tolerable and barely or sometimes interferes with daily life), “severe” (It is intolerable and always interferes with daily activities, which lead to regret for taking this surgery). Satisfaction scale in each patient was recorded from 0 (totally dissatisfied) to 10 (perfect and very satisfied).
Statistical analysis
Data were analyzed with SPSS for Window 21.0(IBM, Armonk, New York). A P-value of less than .05 was considered as statistically significant. Descriptive statistics were presented as mean ± standard deviation, median and interquartile range, numbers (n), and frequencies (%) for categorical variables. Differences between continuous variables were measured by independent t-test. Multiple linear regressions were used to determine influential factors of postoperative patient's satisfaction.
Results
Patients' characteristics are summarized in Table 1. Of the 82 patients, 45 were male and 37 were female. Their mean age was 26.38 years ranges from 14 to 51. Of the 82 patients, 8 had previously undergone ETS, 18 patients had isolated plantar hyperhidrosis, 56 had palmar hyperhidrosis, and 8 had axillary hyperhidrosis. Last follow-up with these patients ranged from 2 weeks postoperative to 16 months, with a mean follow-up time of 6.60 ± 3.56 months. A total of 164 procedures of the limited video-assisted LSB with clip were carried out in these 82 patients. The mean total operation time was 76.02 ± 15.25 minutes. It was decreased over time. For the right side, 54 patients were clipped on L3 level, 27 were on L4, and 1 was on L5. For the left side, 58 patients were clipped on L3 level, 24 were on L4, and no patient was on L5 level (Table 2). Major postoperative complications are listed in Table 3. Sixty-eight patients (77.1%) were completely satisfied (score 10) in the 10th postoperative day evaluation. More than 1 month later, 53 (64.6%) were completely satisfied. However, the early and late satisfaction scores were 9.6 and 9.2, respectively. There was no significant difference in early postoperative satisfaction score between clipping level L3 and L4/5 (Table 4). However, late postoperative satisfaction score was significantly better in the L3 group than that in the L4/5 group. Patient's age and body mass index did not affect satisfaction score. However, male patients and those who had history of hyperhidrosis operation showed higher satisfaction score than others (Table 5).
BMI, body mass index; ETS, endoscopic thoracic sympathectomy; LSB, lumbar sympathetic block; SD, standard deviation.
LVB, lumbar vertebral body.
SD, standard deviation.
BMI, body mass index.
Discussion
Primary focal hyperhidrosis is believed to affect about 1.5%–2.5% of the general population. 3 Hereditary factors cannot be ruled out. The prevalence of primary focal hyperhidrosis in the United States is 2.8%. 9 Its prevalence is reported to be 1% in a population of Israeli adolescents. 10 Onset of its symptoms is usually in childhood or adolescence. A 2010 Korean study has reported that 34.1% of primary hyperhidrosis patients have positive family history. 11 They have a younger onset age than those with negative family history. 11 The involved focal areas are most often palms, soles, face, and axillae in addition to the crown and inguinal region. Most common combined sites are palmar, plantar, and/or axillary regions. 11
Clinical presentation of plantar hyperhidrosis is similar to that of palmar hyperhidrosis. However, clinical presentation of plantar hyperhidrosis is more likely to start later in life possibly because of later maturation of the eccrine sweat glands in the plantar region. 3 Both plantar and palmar hyperhidrosis can significantly interfere with social, emotional, professional, and daily activities. Plantar hyperhidrosis patients especially have consequences including unstable foothold in shoes (high-heels, slippers), problems with walking barefoot, frequently coldness of feet, painful skin lesions, and bromhidrosis (due to bacterial decomposition of sweat that leads to a penetrating odor). 12
Nevertheless, these patients are not aggressive in treatment due to the lack of acknowledge about the curability of surgery and misconception about postoperative compensatory hyperhidrosis and complications. Because the precise pathogenesis of hyperhidrosis is not yet fully understood and its symptoms are subjective, treatment should be carefully decided. In addition, the patient must make an informed decision concerning the best management strategy. 13
The first line of therapy is conservative treatment such as pedal hygiene, topical applicants, iontophoresis, intradermal injection of botulinum toxin, and systemic anticholinergics. However, these can only have temporary effect with many inconvenient problems. Another treatment option is percutaneous sympatheticolysis by transdermal injection of alcohol or phenol under radiological guidance. Such method can result in unwanted tissue damage with uncertain therapeutic effect. In a study on percutaneous sympathectomy with alcohol, 90% of patients have experienced recurrence after 8–24 months. 14
Permanent cure of primary hyperhidrosis can be achieved by lumbar sympathectomy. Surgical treatment for plantar hyperhidrosis is not common for primary hyperhidrosis until recently. It is not as well-known as thoracic sympathectomy for palmar hyperhidrosis. ELS has become more widespread recently after a learning period.5,12
According to article of Hoorens published in 2012, 13 there are three different terms for surgical treatment of hyperhidrosis as sympathetic denervation. The first one is sympathectomy or ganglionectomy. It is performed by a transection above and below the ganglion or by resection or ablation of the actual ganglion. The second one is sympathotomy or sympathicotomy. It is performed by interrupting the rami interganglionares between the stellate ganglion and ganglion. The third one is ramectomy. It results in the interruption of the rami communicantes. Sympathetic chain blocking by using a clip is the analog of sympathectomy and/or sympathicotomy because the nerve is eventually going to be severed as time goes by.
Sectioning the lumbar sympathetic chain from the upper border of the third lumbar vertebra to the lower border of the fourth has been recommended. 15 If a large enough segment is not removed, it can result in failure to achieve anhidrosis due to the regeneration of the preganglionic nerve fibers or the presence of collateral nerve tracts.12,15
Usefulness and advantage of just clipping method versus resection has already been reported by others. Postoperative results of clipping are similar to those with resection.16,17 Furthermore, the clips can be a permanent marker with interruption of side branch and less postoperative neuralgia. In case of mistaken nerve identification or severe compensatory hyperhidrosis, the clip can be removed with little side effects. 3 In addition, nerve resection can cause postsympathecomy neuralgia, which is described as spasmodic and piercing localized to the anterior surface of the thigh, in the inguinal region, the buttock, or the back. 12
In this article, limited video-assisted LSB was performed using 5 mm liga-clip or 3 mm horizontal-clip. During the last decade, ELS has been performed on a routine basis globally. However, this conventional endoscopic approach also has cosmetic wound problem (10 mm port and two 5 mm ports), especially for unmarried young men or women. Li et al. have reported the case of laparo-ELS using homemade 25 mm single port in each side as an ideal solution for cosmetic problem. 18 Its operating time is 110 minutes for the left side and 80 minutes for the right side. In another report, bilateral ELS by unilateral access on left side was performed in 5 women. 19 The mean operating time and hospitalization time were 59 minutes and 12.8 hours, respectively. 19
Here, we described our technique with 25–30 mm single wound with the same or more favorable outcome. Three muscle layers and peritoneal separation from transversalis by blunt finger dissection were required to make main port creation in ELS procedure. Postoperative wound pain is usually caused by muscular origin. Neuralgia itself is associated with mobilization or dissection of nerve rather than incisional wound because sensory innervation is very rich around the vertebral body. 3 In the same manner, manipulation in the retroperitoneal space was done by only working instruments without any cautery in our technique. This method can reduce unnecessary tissue damage. Therefore, postoperative neuralgia can be dramatically decreased.
Another advantage of our method is that it can result in accurate identification of sympathetic ganglion and chain by finger detection and ancillary endoscopic vision. An accurate dissection of sympathetic chain without any interruption of complex network of nerves and other structures is important to avoid postoperative neuralgia and complications. It is not always possible to identify the ganglia with only camera vision due to retroperitoneal anatomical complexity, unlike thoracic cases. Moreover, in obese patients who have high body mass index (BMI) with more adipose tissue in the retroperitoneal and subcutaneous layer, the identification of the sympathetic chain can be more difficult. 19 In these cases, only camera vision may not be good enough. Furthermore, the nature and location of sympathetic ganglia on either side could be different from individual to individual. Therefore, we should consider uncertain location of arterial, venous, and lymphatic structures.
To perform this technique adeptly, learning period is needed. In this study, the total operation time was more than 100 minutes for the early seven cases. After that, the operation time was reduced to less than 60 minutes for most cases.
Clamping of the sympathetic trunk at the L3 level will interrupt the sympathetic innervation from that level to caudally located L4 to S3 levels, thus reducing sweating on the feet. 3 During this procedure, the possibility of mismatched clip location bilaterally must be kept in mind. In our series, there was no significant difference in outcome between clipping at L3 and at L4 level in the early postoperative period. However, the satisfaction score in the L3 group was significantly better than the L4/5 group at late postoperative period. Therefore, identifying and clipping L3 sympathetic trunk is recommended.
The possibility of retrograde ejaculation should be concerned postoperatively in male patients. In a recent study, retrograde ejaculation can be avoided when lumbar sympathectomy is performed at L3 or L4. 12 The navel can be used as a guide to L3. There was no case of such complication in our series.
Compensatory sweating was originally thought to be a mechanism of excessive sweating to maintain a constant rate of total sweat secretion. 14 However, recently it is believed that this mechanism represents a reflex action by an altered feedback at the level of the hypothalamus depending on the level at which sympathetic denervation occurs. 13 Severe compensatory sweating after ETS can occur in about 3%–5% of patients.20,21 After lumbar sympathetomy alone, severe compensatory sweating has been found to be rare. 12 Severe compensatory sweating is primarily limited to the lower leg areas. 3 On the other hand, lumbar sympathectomy promotes an increase in compensatory sweating in the dorsal and abdominal regions of patients who have previously undergone ETS. 5 In another study, there was little change in the levels of compensatory sweating in those patients with prior ETS. 3 Interestingly, the greater the BMI, the worse the compensatory sweating development after ETS. This could be related to BMI in lumbar cases.5,22 However, in our study, BMI did not affect patient's satisfaction during the late postoperative period. Therefore, further studies with more cases should be followed.
In our study, male patients showed better satisfaction than female patients. This might be due to the possibility that women might have suffered more from excessive sweating than men.
Postoperative temporal hyperhidrosis usually occurs within 3–4 days or a week. According to the report of Reisfeld, 3 the prevalence of this phenomenon is about 11% in patients after lumbar sympathectomy. After ETS, the prevalence is ∼40%. 3 It is known that sweat production is neurotransmitter mediated. This process might have already begun before the blocking of nerves. 3
Footnotes
Conclusions
ELS is universally applicable as a surgical treatment for plantar hyperhidrosis. Limited video-assisted lumbar sympathectomy as another modality is a feasible procedure that can greatly facilitate the identification of sympathetic ganglion via single wound. Through limited video-assisted LSB using clip without nerve resection, lessened complication and higher success rate can be achieved for plantar hyperhidrosis.
Disclosure Statement
No competing financial interests exist.