
Abstract
Abstract
Introduction:
Hyperthermic intraperitoneal chemotherapy (HIPEC) is delivered after cytoreductive surgery (CRS) in selected patients with peritoneal carcinomatosis. The closed-abdomen technique, preferred by many centers, prevents heat loss and drug spillage, but does not warrant homogeneous distribution of the perfusion fluid (PF). The hypothesized formation of intra-abdominal adhesions during the closed-abdomen perfusion period has never been described.
Materials and Methods:
From March 2014 to April 2016, 10 consecutive patients with peritoneal carcinomatosis, selected for CRS, underwent the Laparoscopy-Enhanced HIPEC technique to explore the abdominal cavity during the perfusion. The aim of the study was to investigate the incidence and the extent of intra-abdominal adhesions that are formed after CRS during the perfusion period of closed-abdomen HIPEC.
Results:
During the perfusion, adhesions developed in 70% of the patients. Adhesions developed mainly in the period between the closure of the abdomen and the subsequent filling of the abdomen with the PF. After their first division, during the following perfusion period, adhesions between the bowel and the abdominal wall reformed in 3 patients (30%).
Conclusions:
Intra-abdominal adhesions are frequently formed during closed-abdomen HIPEC and can hamper the adequate circulation of the PF. The Laparoscopy-Enhanced technique enables the early detection and the division of any intra-abdominal adhesions.
Introduction
H
As the whole peritoneal surface is exposed to cancer cells, the efficacy of HIPEC relies on both warranting adequate circulation of the PF and keeping the desirable temperature inside the entire abdominal cavity.
Even if several techniques for delivering HIPEC have been proposed, they must all be considered variations between two main streams: the open (Coliseum) technique and the closed technique. 3
The open technique focuses on stirring the abdominal contents to improve the circulation of the PF, but takes with it the considerable weakness of a great thermal dispersion and the potential risk for contamination of the operating field and personnel. 4
The closed technique focuses on a better preservation of heat and a reduced risk for contamination, but may not allow the adequate exposure of the whole peritoneal surface to the PF.1–5 This inability, which is well known, is attributed to the onset of preferential flows and of intraoperative adhesions between the bowel and the abdominal wall. Both these factors could act together in creating standing pools of PF and closed peritoneal spaces that cannot be reached by the PF.6,7
The formation of intra-abdominal adhesions during closed-abdomen HIPEC (IAs) although strongly suspected has never been reported before and its incidence is still unknown.
Recently, we described a novel technique, that is, the Laparoscopy-Enhanced closed-abdomen HIPEC (LE-HIPEC), in which the abdominal cavity is explored by means of laparoscopy during the perfusion period of closed-abdomen HIPEC.8,9
The aim of our study was to use LE-HIPEC to demonstrate the formation of IAs during the perfusion period and to describe its incidence and extent.
Materials and Methods
Subjects were patients aged 18–75 years with peritoneal carcinomatosis or positive peritoneal cytology, suitable for cytoreductive surgery (CRS) with no macroscopic residual disease.
CRS was performed as described by Sugarbaker. 10 At the end of CRS, four drains were left in the abdominal cavity and the patients were prepared for LE-HIPEC.8,9 The skin was closed with four continuous locking sutures. Three balloon trocars were placed at the junction between sutures and connected, respectively, to the HIPEC inflow tube, to a heated CO2 insufflator, and to a smoke evacuator device (Fig. 1).

Placement and connections of the balloon trocars.
The abdomen was filled with the PF and a continuous flow was set. Heated CO2 was then insufflated with pressure adjusted to 7 mmHg and pneumoperitoneum was established, creating a little working space between the surface of the PF and the anterior abdominal wall.
A laparoscope was inserted and the abdominal cavity was inspected. A 10 mm laparoscopic palpator was used to stir the abdominal contents and divide any IAs eventually detected during the inspection of the abdomen.
After 5 minutes of stirring, the pneumoperitoneum was evacuated and the perfusion continued in a closed-technique manner for 10 minutes. Laparoscopic exploration was repeated every 15 minutes until 90 minutes of perfusion were reached. The temperature of the abdomen was constantly maintained at 42°C. Cisplatin and paclitaxel were the preferred drugs used for patients with gastric and ovarian cancer, while cisplatin and mitomycin were used for patients with colorectal cancer.
A video documentation of the IAs found at laparoscopic exploration was obtained. At the end of the study, video recordings were analyzed retrospectively, and the incidence, the extent, and the site of IAs were recorded. The classical division of the abdomen into nine regions was adopted for the description. All the regions of the abdominal cavity were explored, using the palpator to displace the bowel and to open the subphrenic spaces, the hepatorenal space, and the recesses of the mesentery. If IAs were found, they were completely divided by means of the palpator and the bowel was repeatedly stirred before evacuation of the pneumoperitoneum. The last laparoscopic exploration of the abdomen was always performed 15 minutes before the end of perfusion.
At the end of the perfusion time, the PF was evacuated through the drains, and the abdominal cavity was refilled with 3000 mL of saline solution, which was then retrieved through the drains. Finally, the wound was reopened to explore the abdomen and perform the restorative procedures, as required.
Results
From March 2014 to April 2016, 10 consecutive patients were selected. The primary tumor was gastric cancer in 4 patients, colorectal cancer in 3 patients, and ovarian cancer in 3 patients. Mean age of the patients was 53 ± 10 years. Mean peritoneal cancer index score was 7 ± 6. The mean number of peritonectomy procedures was 4 ± 1. The mean number of combined resections was 4 ± 1. Patient characteristics and operations are shown in Table 1.
Diagnosis: GC, gastric cancer; CRC, colorectal cancer; OC, ovarian cancer.
CC, completeness of cytoreduction score; PCI, peritoneal cancer index; PP, peritonectomy procedures.
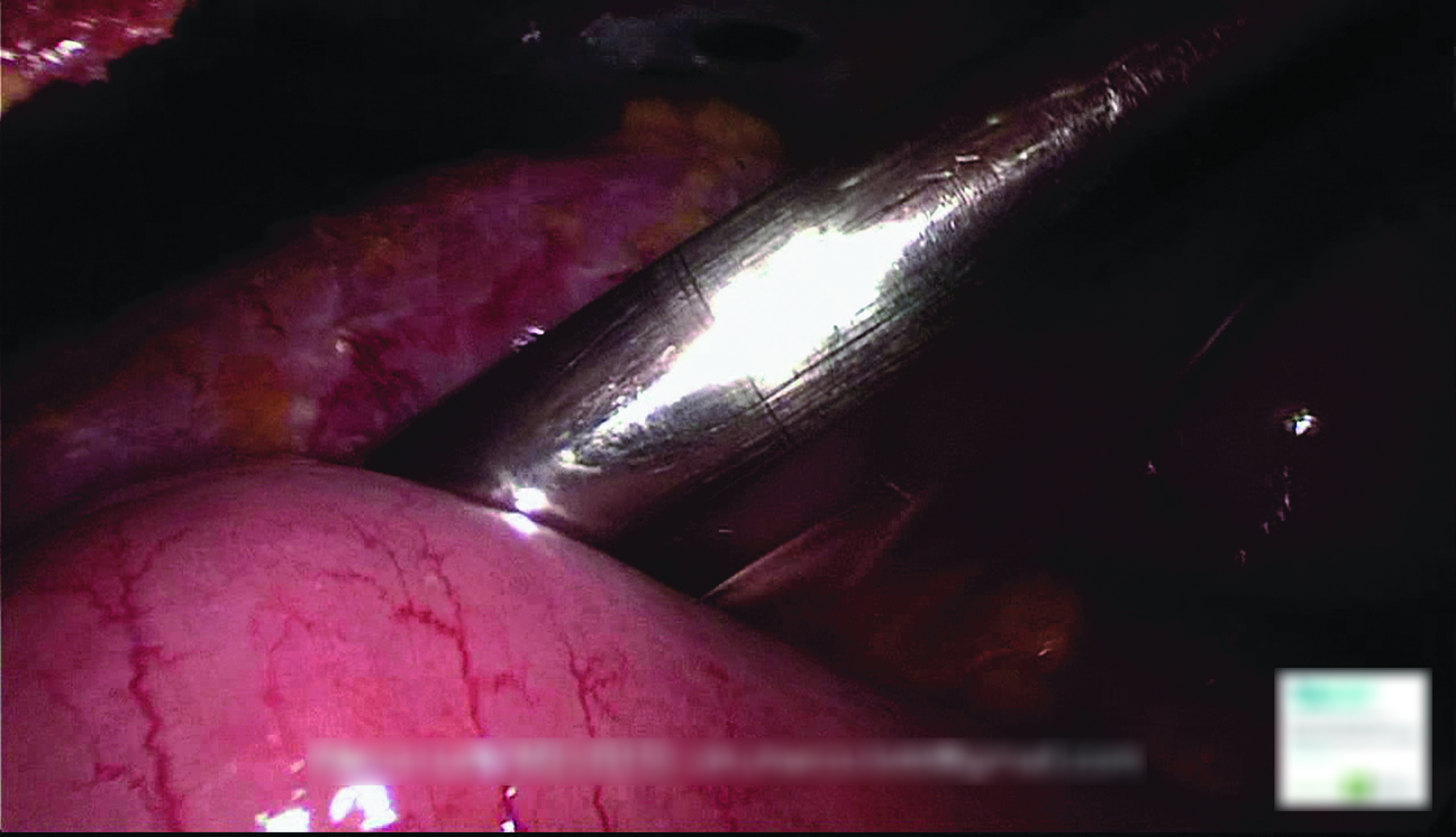
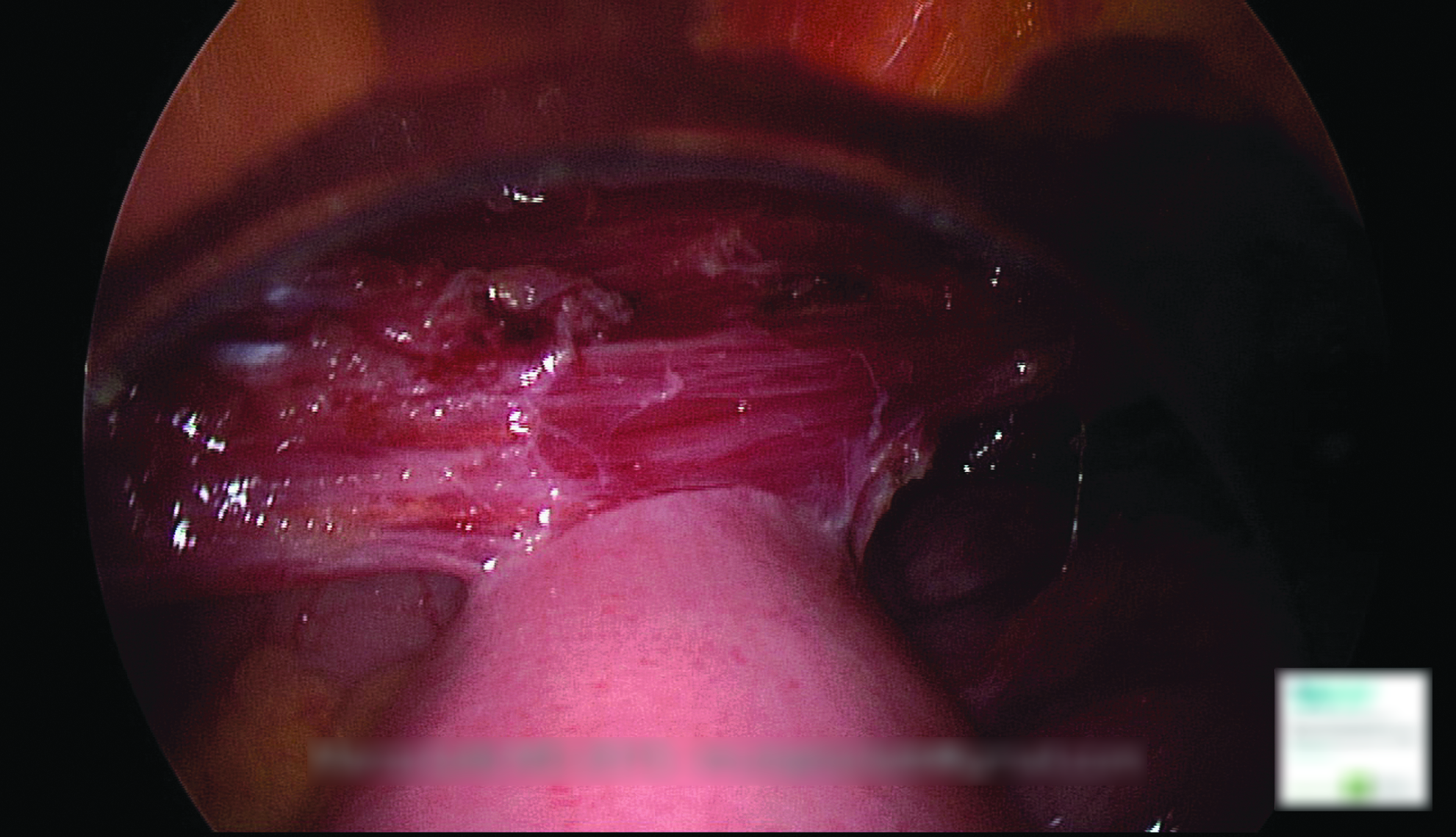
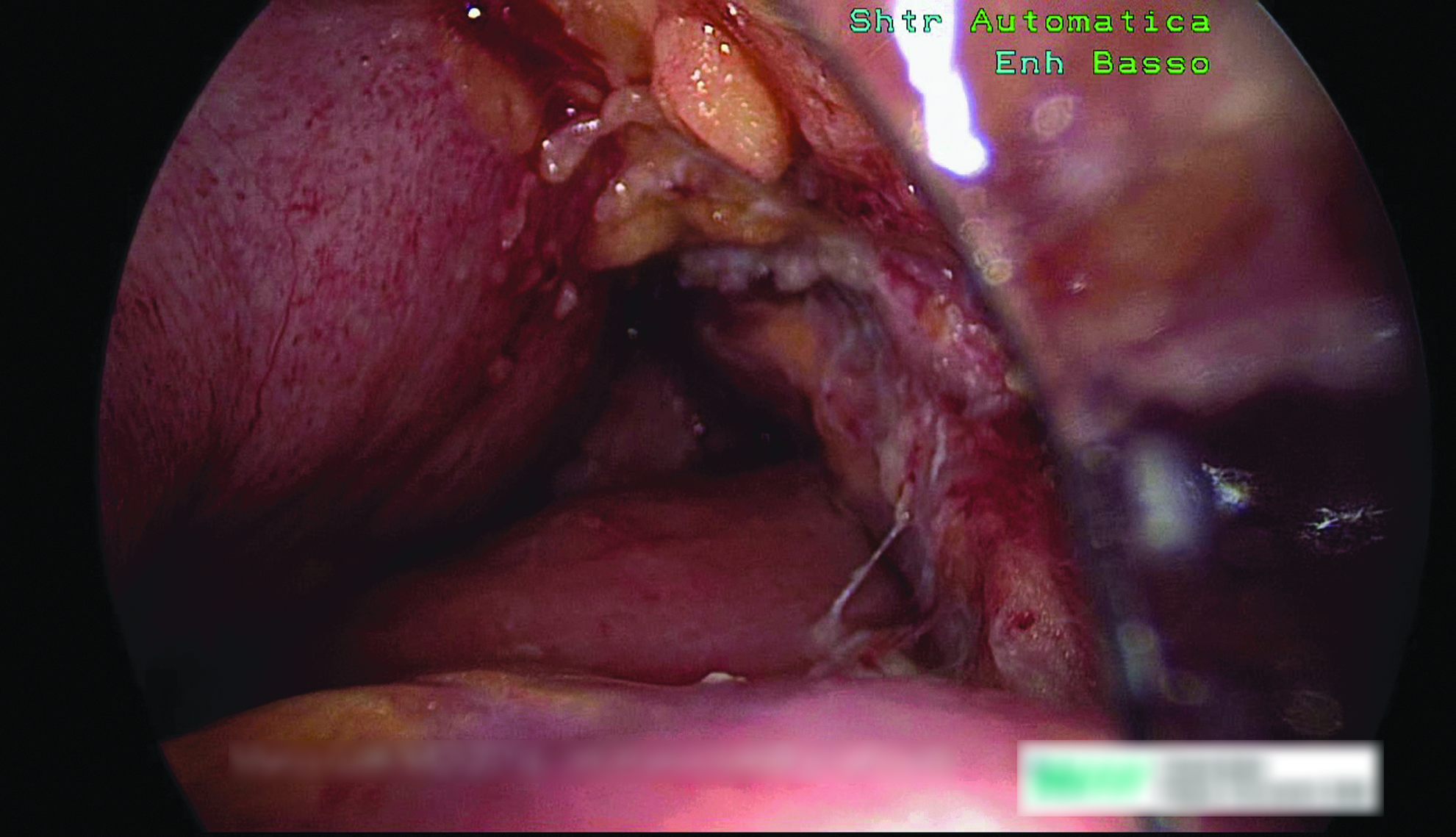
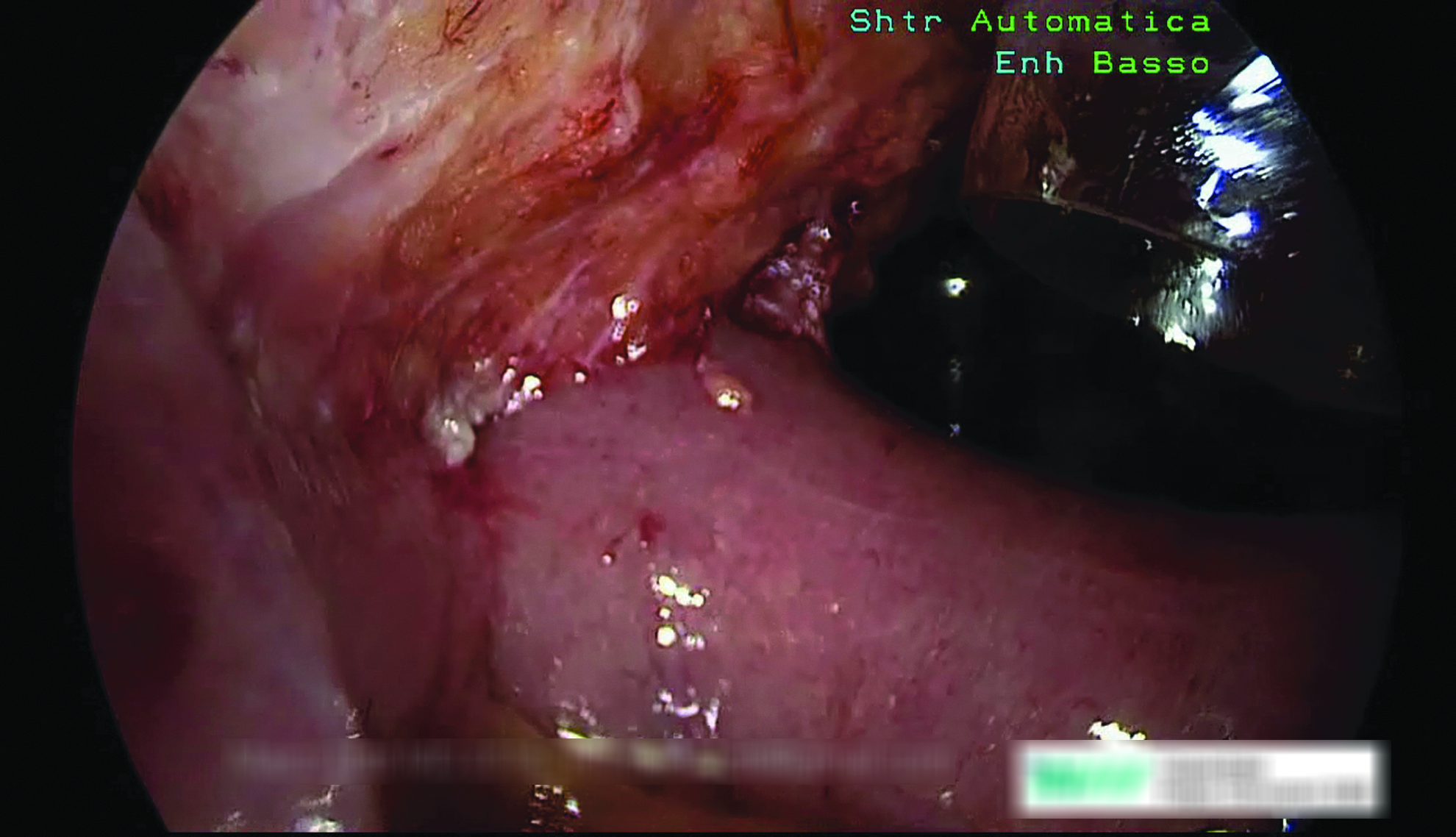
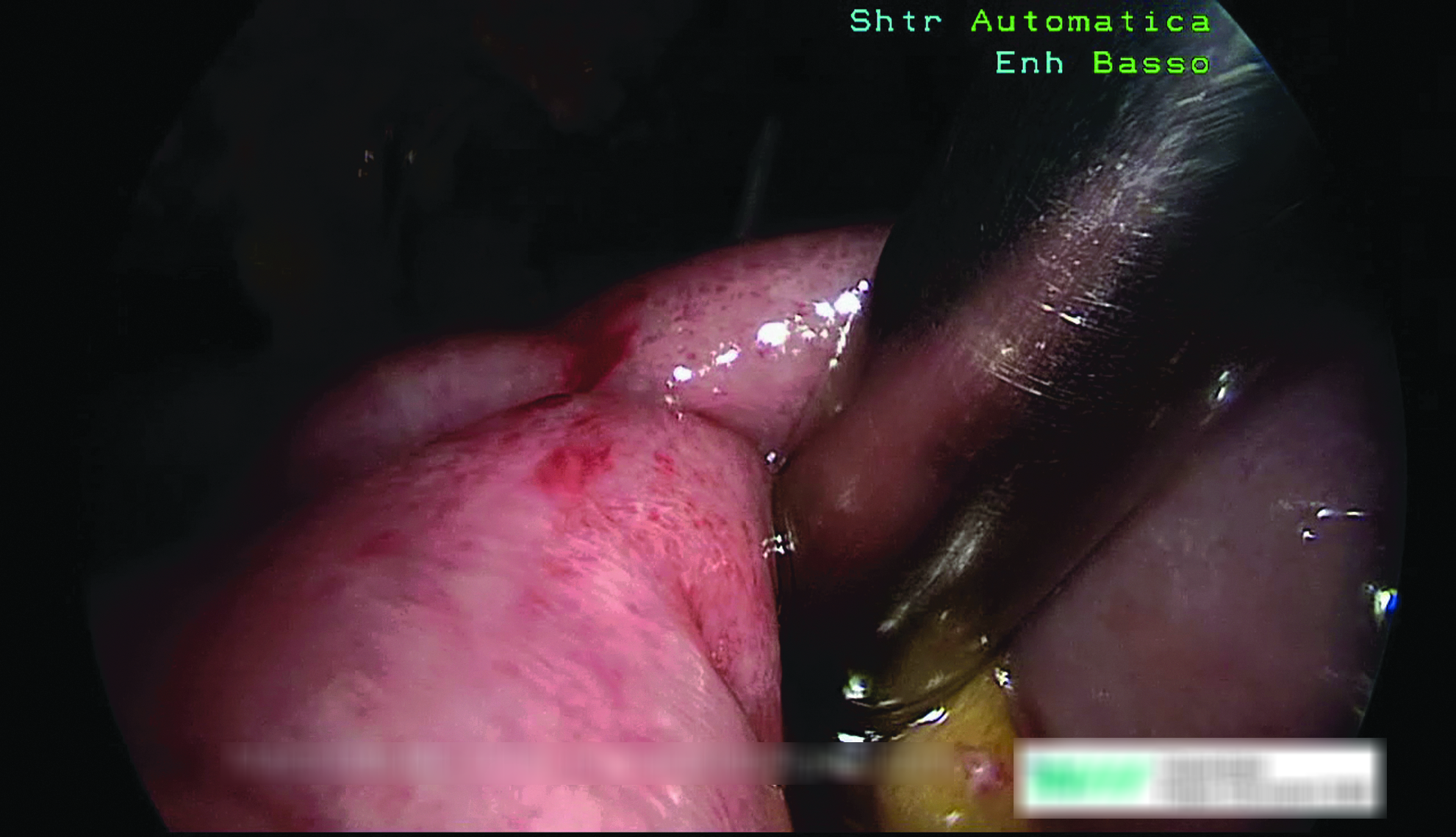
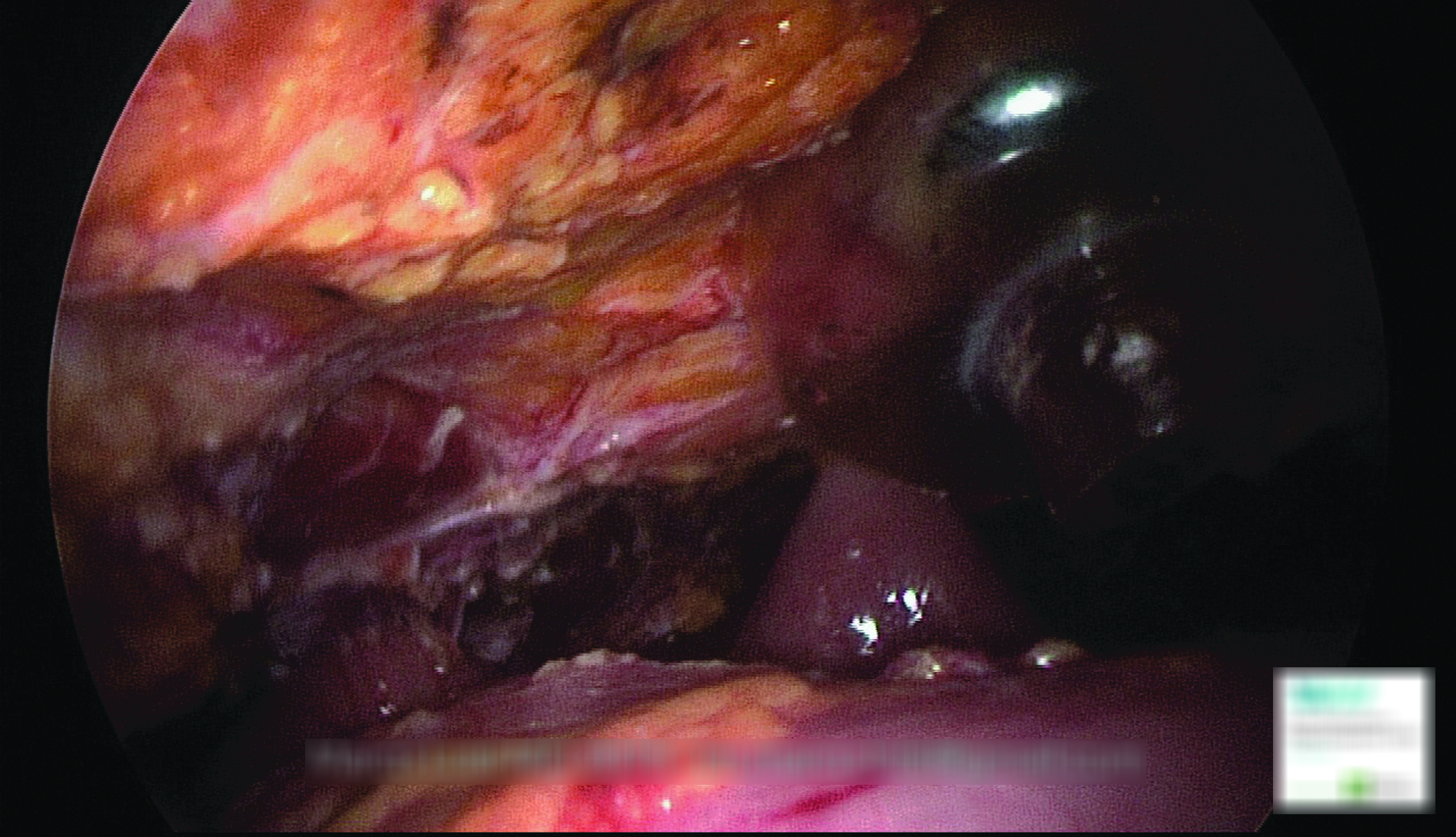
During the first laparoscopic exploration, IAs were found in 7 patients (70%): IAs formed among the loops of the small bowel in 2 patients, between the small bowel and the colon in 3 patients (Fig. 2) and between the bowel and the anterior abdominal wall in 6 patients (Figs. 3 and 4). IAs between the bowel and the abdominal wall involved one abdominal region in 1 patient, two abdominal regions in 1 patient, three abdominal regions in 3 patients, and seven abdominal regions in 1 patient. This last patient required extensive division of IAs to access his whole abdominal cavity and was also found with IAs in-between the bowel loops (Figs. 5, 6, and 7).
Adhesion between a jejunal loop and the transverse colon.
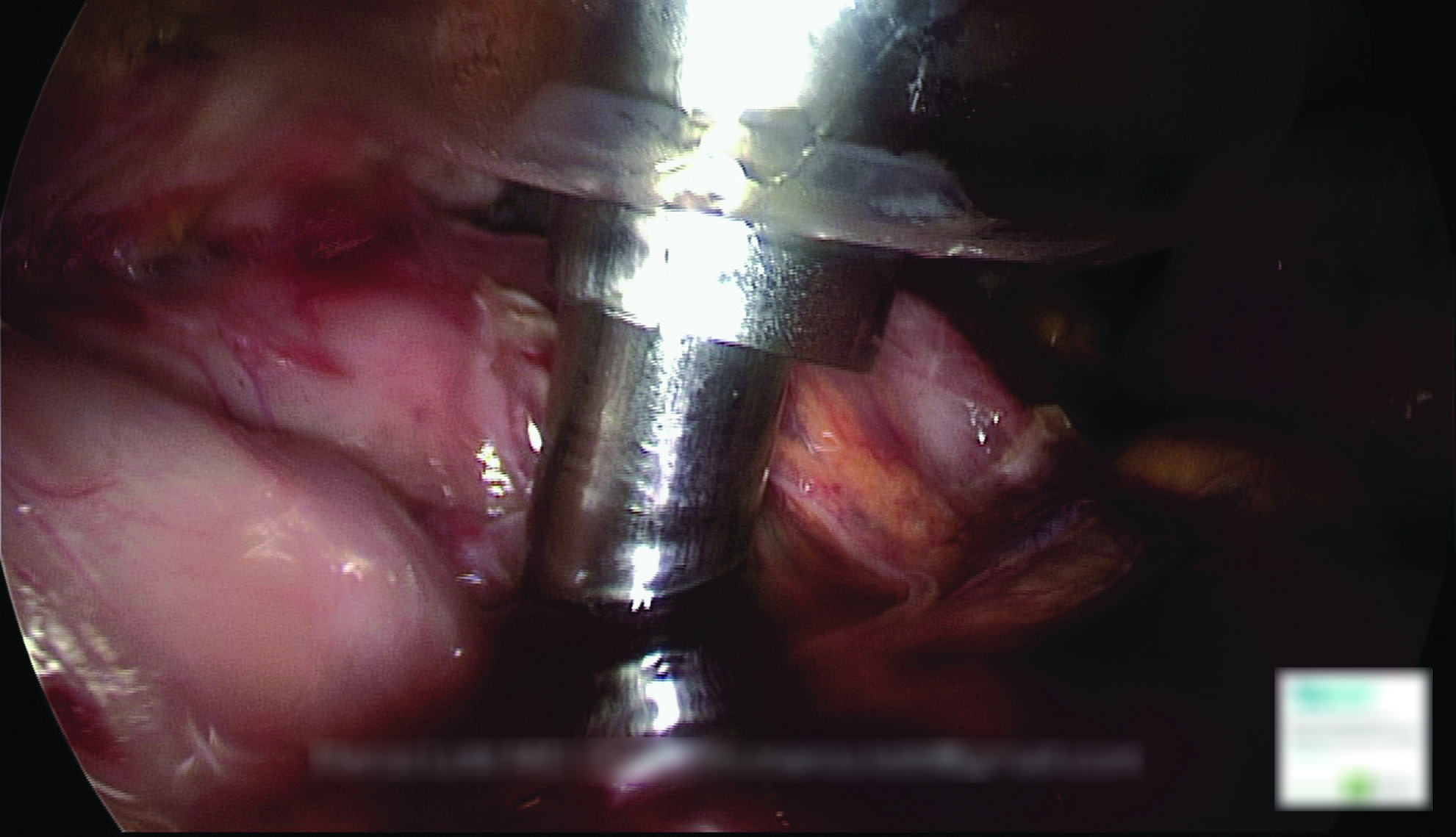
Adhesions between the bowel and the anterior abdominal wall.
Adhesion between a jejunal loop and the rectus abdominis muscle.
Extensive adhesions between the bowel and the anterior abdominal wall.
Extensive adhesions between the bowel and the anterior abdominal wall.
Extensive adhesions among the loops of the bowel.
All the IAs observed at the first access were firm enough to resist the tension generated by the pneumoperitoneum and their complete division was achievable only by means of the laparoscopic palpator.
Once the division of any IAs was completed at the first laparoscopic access, during the following perfusion period, IAs between the bowel and the abdominal wall reformed in 3 patients. IAs were observed in 2 patients at the second access (after 15 minutes), in 3 patients at the third access (after 30 minutes), and in 1 patient at the fourth access (after 45 minutes). Those adhesions were always limited and weak (Fig. 8). No IAs among the loops of the bowel reformed after their division. No IAs were observed beyond 45 minutes of perfusion. The details on IAs are shown in Table 2.
Adhesions found after the first division.
15–30–45 Minutes, laparoscopic exploration after 15–30–45 minutes.
E, epigastric region; FA, first access; H, hypogastric region; LH, left hypochondriac region; LI, left iliac region; LL, left lumbar region; RI, right iliac region; RL, right lumbar region; Sb, small bowel; U, umbilical region.
Discussion
Closed-abdomen HIPEC is preferred by many surgical teams for safety reasons.1,11,12
The closure of the abdominal wound minimizes heat loss and allows for a better thermal stability of the abdomen, but prevents the surgeon from intervening in the flow of the PF.
Uneven distribution of the PF with the closed technique and the onset of preferential flows between catheters have been reported by many authors.1,6,7,11,12 These evidences led some authors to propose their modified closed techniques, to allow the manual stirring of the PF, or to increase the turbulence of the PF by means of recirculating CO2.11,12
Despite the attention given to the stirring of the PF (which is the hallmark of the open Coliseum technique), manual agitation of the PF could have little effect on the distribution of heat and the cytotoxic drugs, because the abdominal cavity is not comparable to an empty basin, but it is filled with the abdominal contents.
The presence of the bowel, the mesenteric recesses, the liver, and the spleen create barriers that hinder the circulation of the PF and retain the PF into closed paths. As a consequence, the flow of the PF is split into several streams with different flow speed, flow rate, and turbulence. Therefore, the most effective way to intervene in the circulation of the PF could be to repeatedly change the position of the abdominal contents, to create new paths in which the PF can flow. In the closed technique, this is usually pursued by changing the position of the patient.
Unfortunately, tilting the operating table, which is very effective in displacing the bowel during a standard operation, could have a limited effect in displacing a bowel that is floating in the PF during HIPEC and no effect at all in displacing a bowel that is fixed by IAs.
Even if CRS can account for considerable risks for the formation of early IAs, the impact of early IAs on the circulation of the PF during closed-abdomen HIPEC has never been reported and their incidence is unknown.
The results of our study show that the relatively short period between the closure of the wound and the filling of the abdominal cavity with the PF is critical for the formation of IAs. During this period, many factors that promote the formation of IAs are working: after CRS, the abdominal wall is cauterized, the deeper muscular layers are exposed, and areas of ischemic tissue are created; and the serosal surfaces of the bowel and the residual parietal peritoneum are dried, crushed, and cooled. All these risk factors are known to induce inflammation and the formation of a fibrinous exudate, which is responsible for early adhesion of the involved surfaces. 13
Our findings show that early IAs are frequent after CRS and firm enough to resist the tension produced by filling the abdomen with the PF and creating the pneumoperitoneum. A 60% incidence of IAs was observed between the abdominal wall and the bowel; those IAs involved more than one abdominal region in half of the patients. Furthermore, 30% of the patients were found with IAs among the loops of the bowel: these adhesions could be particularly dangerous because they create closed spaces among the mesenteric surfaces, which are not reached by the PF.
We hypothesize that even limited IAs can interfere with the circulation of the PF, because the adherent loops of the bowel act as a barrier and create lateral vortexes among which the PF is restrained, leading to the formation of pools of stagnant PF behind them. 14 Therefore, the adherent surfaces between the bowel and the abdominal wall are not reached by the PF and some areas of the abdomen behind them could be underexposed to heat and cytotoxic drugs.
In our series, relapse of IAs after their first division was less frequent and only limited and weak adhesions were formed during the following perfusion period. Thus, it is reasonable to think that the progressive heating and moistening of the serosal surfaces and the abdominal wall, together with the reduction of ischemic areas due to the vasodilatation induced by heating, prevented any further formation of IAs. 15 During the laparoscopic exploration, an intense evaporation is easily observed in the working space, even if a small amount of dry CO 2 is insufflated (Fig. 9). The abdominal cavity quickly becomes a warm environment that is saturated by humidity, a condition known to reduce the formation of IAs.15–18

Evaporation occurring in the working space during LE-HIPEC. LE-HIPEC, Laparoscopy-Enhanced closed-abdomen hyperthermic intraperitoneal chemotherapy.
Conclusions
According to our findings, the formation of IAs during closed-abdomen HIPEC seems to be more frequent than expected and should be addressed. LE-HIPEC provides the surgeon with a tool to detect and divide any IAs, preventing their further formation during the perfusion period. While it may be true that the formation of IAs limits circulation of the perfusate and the efficacy of HIPEC, our study is not designed to test this hypothesis. Our preliminary data suggest that addressing any IAs could be decisive to avoid the inadequate circulation of the PF during closed-abdomen HIPEC, but further studies with larger case series are needed to confirm this assumption and to clarify whether the LE-HIPEC technique with the division of IAs has any clinical impact and is more beneficial than other HIPEC techniques.
Footnotes
Acknowledgments
The authors thank Dr. Richard Naspro for his help with editing.
Authors' Contributions
L.M. conceived the Laparoscopy-Enhanced technique, designed the study, analyzed and discussed the data, and drafted the article. M.G.C. contributed to the study design, data interpretation, and made critical revisions to the article. All the authors contributed to the acquisition of data and revision of the article.
Disclosure Statement
No competing financial interests exist.