
Abstract
Abstract
Background:
Around 70% of children with neurodisability (ND) present pharyngeal neuromuscular incoordination and severe gastroesophageal reflux disease (GORD).
Methods:
This is a pilot study with the Robotic-assisted minimally invasive total esophagogastric dissociation (TOGD).
Results:
We included 4 patients, 2 males and 2 females, with ND and severe GORD refractory to medical treatment.
Conclusions:
Pharmacological management of GORD is often unsuccessful and antireflux surgery is common, but it has a high failure rate with symptom recurrence, requiring re-do surgery. TOGD is a good option for these patients.
Introduction
A
Patients and Methods
Three children with ND scheduled for surgery for GORD at Gaslini Children's Hospital, Genova, from November 2015 to April 2016, and one child from the Department of Pediatric Surgery of Siena were included in this prospective clinical trial. The indications for primary robotic TOGD were severe neurological impairment with swallowing difficulties, severe GORD refractory to medical treatment, recurrent respiratory “infections”, failure to thrive, and poor QoL for both the children and the caregivers. All had a preoperative upper gastrointestinal (GI) contrast study for assessing anatomy and gastroesophageal reflux. One child also had videofluoroscopy for assessment of swallowing, and 3 had upper GI endoscopy.
Surgical procedure
Under general anesthesia and epidural pain relief, the patient was positioned in the supine position with arm boards, and the abdomen inflated with 12 mmHg pressure. A 12-mm disposable camera-port was placed at the umbilicus to take a camera on a 10-mm HD 30-degree scope. Two 8-mm reusable robotic ports in the right and left upper quadrants took the four robotic arms for the da Vinci Si Model™ (Intuitive Surgical, Inc., Sunnywale, CA). Two further 5-mm disposable accessory ports were used for suction, traction, and for the LigaSure “seal and divide” device (LigaSure™ Maryland; Covidien Medtronic, MN).
Laparoscopic phase
A marker suture was placed at 20 cm distal to the duodenojejunal flexure. The jejunum was exteriorized through the umbilical port incision and divided and sealed with the LigaSure at the marker suture. A tension-free vascularized isoperistaltic Roux-en-Y jejunal loop was fashioned distally dividing the mesenteric vessels appropriately. Bowel continuity was established by end-to side jejunojejunostomy at 20–30 cm from the proximal end of the Roux-en-Y and the exteriorized bowel replaced into the abdomen.
Robotic phase
The lower esophagus was mobilized preserving paraesophageal neurovascular structures, and the esophagus disconnected from the stomach using a monopolar scissor and the LigaSure. The stomach was closed in two layers. The jejunal Roux-en-Y loop was passed through the mesocolon and behind the stomach and an end-to-end isoperistaltic esophagojejunal anastomosis undertaken manually with 5/0 interrupted sutures. A nasoesophageal tube was positioned to facilitate the anastomosis and left in situ postoperatively on open drainage until return of bowel function. The jejunal loop was tethered to the gap in the mesocolon. A Stamm gastrostomy was placed (Fig. 1A–D).

Main meaningful steps of the robot-assisted minimally invasive total esophagogastric dissociation. Magnified view of the retrogastric anatomical space associated with wrist-like movements of the robotic device enhances the laparoscopic performance. The seven degrees of freedom of the articulated instruments empowered the precision of the esophagojejunal anastomosis, minimizing esophagus retraction, and manipulation. Thanks to the high resolution of the three-dimensional view, all mesentery windows are safely closed to reduce the risk of internal hernia.
Follow-up
Before commencing, enteral feeding patients underwent a postoperative upper Gl-tract X-ray contrast study. At follow-up outpatient visits, a nutritional assessment, anthropometric and biochemical parameters, number of respiratory infections, days of hospitalization, and feeding problems were recorded.
Case Reports
Patient 1
A 1-year-old female with severe infantile epileptic encephalopathy, inability to swallow and increasing vomiting and aspiration pneumonitis presented below the fifth percentile at 9.7 kg. Videofluoroscopy and an upper GI-tract X-ray contrast study confirmed the swallowing problem and severe gastroesophageal reflux. Following informed parental consent, the child underwent a robotic-assisted minimally invasive TOGD. Bowel activity was established on postoperative day (POD) 5, initially with diarrhea that gradually resolved with dietary modification. Following confirmation on a postoperative contrast study of full healing and anastomotic patency (Fig. 2), the intravenous nutrition was gradually replaced, as of POD6, with increasing gastrostomy feeds. At 2-month follow-up her dysphagic symptoms had markedly reduced, and there was major improvement in her respiratory and nutritional status. Her caregivers reported easier feeding, less time required for overall care, and a reduction in respiratory problems, and hospital visits.

Postoperative upper gastrointestinal-tract X-ray contrast study showing the good progression of the iodinated contrast agent through the esophagojejunal anastomosis, without signs of strictures or leaks.
Patient 2
The second patient was a 24 kg (below the fifth percentile), 15-year-old boy with spastic cerebral palsy on treatment with an intrathecal baclofen pump. Enteral feeding was tolerated until his pubertal growth spurt when he developed feeding intolerance with severe vomiting and failure to thrive, which were refractory to medical management. Upper GI endoscopy and X-ray contrast studies showed a large hiatus hernia, severe esophagitis, and gastroesophageal reflux. The child underwent robotic-assisted TOGD with the informed consent of his parents. He did not require ICU admission postoperatively and recovery was uneventful. On POD6, oral and gastrostomy upper GI-tract sequences showed normal progression of contrast (Fig. 3). The nasojejunal tube was removed and gastrostomy and oral feeding (to tolerance) were commenced. He was discharged on POD13. At follow-up there was no recurrence of GORD, regurgitation or vomiting, and ease of feeding improved significantly with his mother reporting a better for the child and the family. At 1-month follow-up bolus gastrostomy feeds were well tolerated and he was also able to enjoy a small amount of oral intake without dumping. He returned to school and all activities. His parents reported a remarkable change for the better in their son's QoL as well as their own.
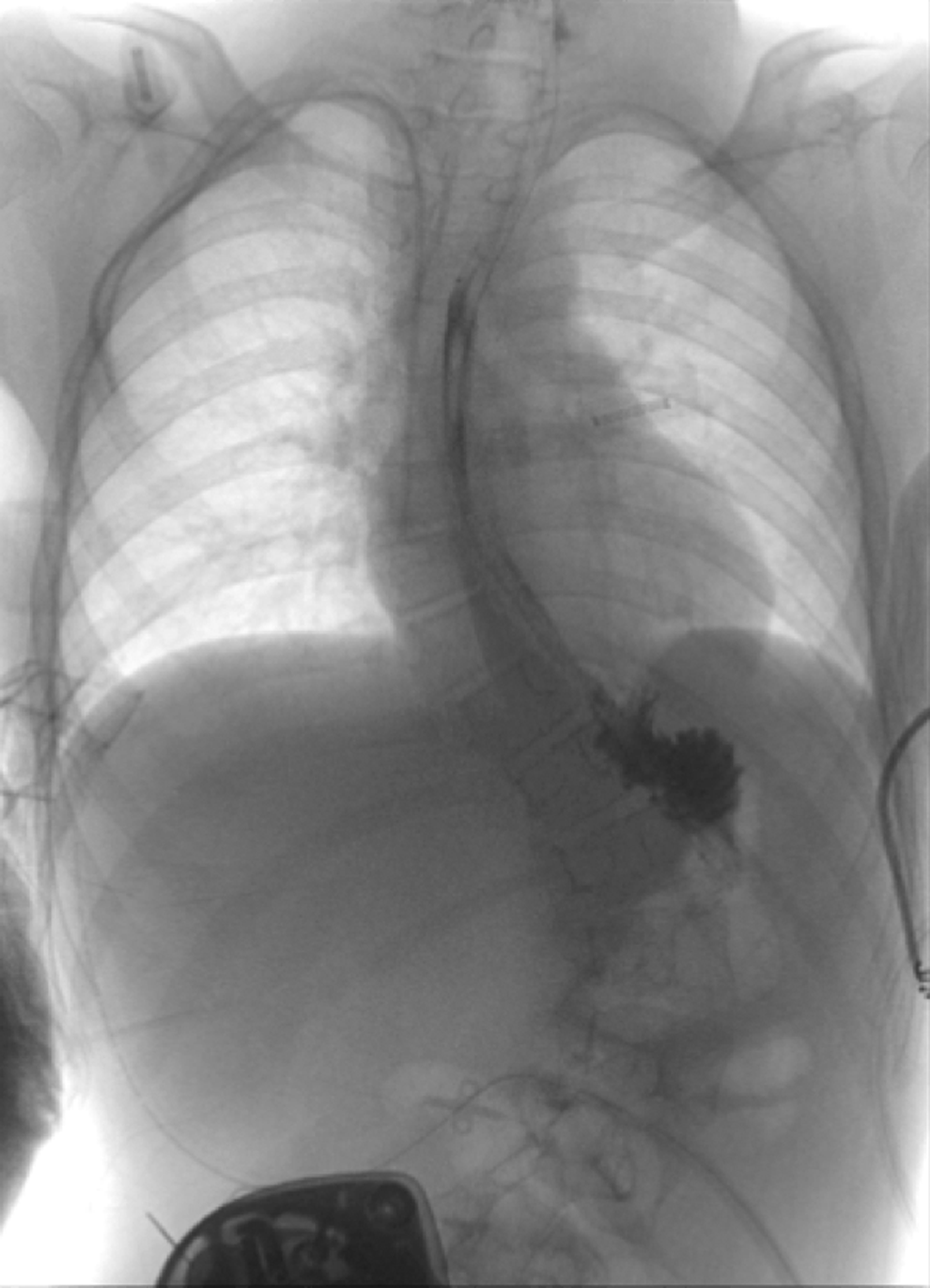
Postoperative upper gastrointestinal-tract X-ray contrast study proving the patency and the integrity of the esojejunal anastomosis.
Patient 3
A 7-year-old boy with spastic dystonic quadriparesis and a history of esophageal atresia (EA) had undergone a laparoscopic Nissen fundoplication and a second procedure 1 year later to place a diaphragmatic on-lay mesh because of ongoing GE reflux. Two uneventful years later he developed night time coughing and dyspnea associated with failure to thrive and weight loss. On presentation, he weighed 13 kg at a height of 110 cm, both below the fifth percentile. An upper GI-tract X-ray contrast study showed significant hold up of contrast at the lower esophagus (Fig. 4A), and esophago-gastric endoscopy confirmed an esophageal perforation with migration of the mesh patch into the esophageal lumen. The robotic-assisted minimally invasive TOGD was complicated by adhesions between the liver, the stomach, and the colon. The Nissen wrap was taken down with considerable difficulty, and the mesh was removed. On POD5 a right pleural effusion required a chest drain, and a contrast study on POD6 showed a small leak at the esophagojejunal anastomosis that was treated conservatively (Fig. 4B). The unexpected development of fecal discharge from the medial aspect of the abdominal wound led to exploration with identification of a perforation of the transverse colon possibly related to an inappropriate suture during abdominal closure. The perforation was repaired and a temporary defunctioning ileostomy was placed. Delay in gastric emptying slowly resolved over several weeks.

Patient 4
A 3-year-old girl weighing12 kg (5th–10th centile) with a hypoxic brain injury from birth, presented to the Department of Pediatric Surgery of Siena with swallowing and feeding difficulties, repeated vomiting, and failure to thrive, for which a feeding gastrostomy had been placed. An upper GI contrast study confirmed marked gastroesophageal reflux and delayed gastric emptying. Following parental counseling and consent, the child underwent a robotic-assisted minimally invasive TOGD and a pyloroplasty (Fig. 5) to ensure gastric emptying. Postoperative parenteral nutrition was maintained until POD9 when a contrast study showed good GI transit with no anastomotic leaks (Fig. 6). Progressive enteral nutrition, mainly through the gastrostomy, was commenced and she was discharged on POD15 in good condition and a weight of 14 kg.
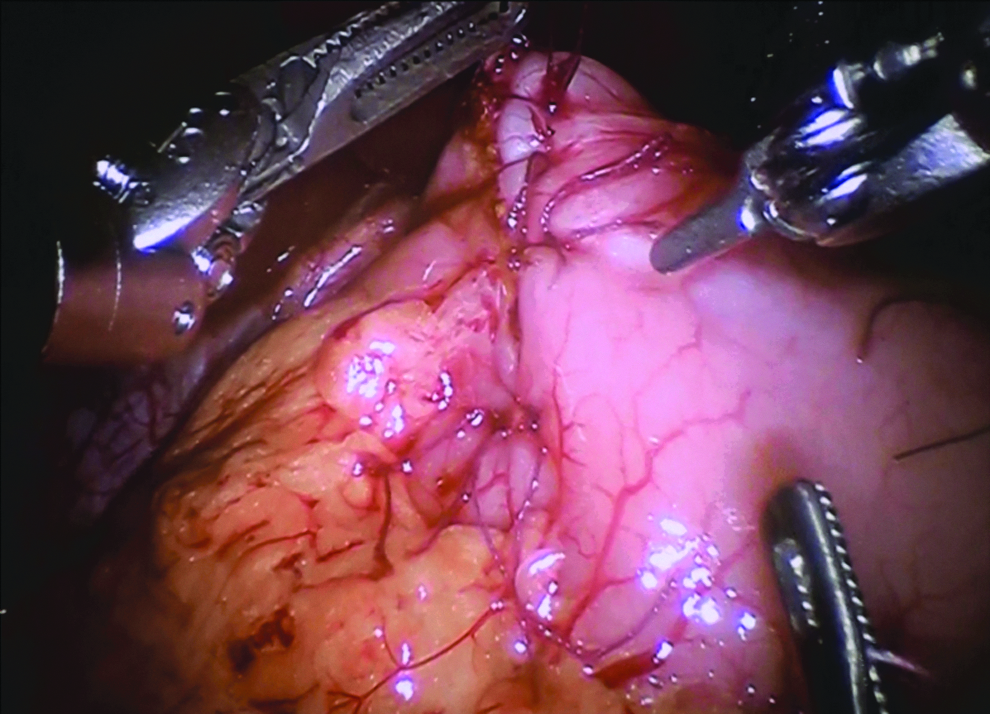
Case 4: Performing a pyloroplasty to improve gastric emptying.

Case 4: The gastrointestinal-tract contrast study performed on postoperative day 9 with no evidence of leak of anastomosis.
Discussion
In addition to pharyngeal neuromuscular incoordination children with ND have a 70% incidence of gastroesophageal reflux 4 that is refractory to conservative medical treatment, and a worse outcome for fundoplication than those who are neurologically normal.9,12,13,16–18 In 1997, Bianchi proposed TOGD (Fig. 7) to definitively eliminate GE reflux and food aspiration. Through a transverse left hypochondrial incision, the lower esophagus was mobilized taking down any residual fundal wrap and transected above the gastroesophageal junction. The stomach was oversewn in two layers and drained by a Stamm gastrostomy. A vascularized isoperistaltic segment of jejunum, fashioned as a Roux-en-Y on a tension-free blood supply, was brought through the transverse mesocolon and behind the stomach to form a wide oblique anastomosis with the esophagus. Bowel continuity was established by an end-to-side jejunojejunostomy at 20–30 cm (age dependant) from the esophagojejunal anastomosis. Postoperative gastrostomy and nasojejunal tube drainage were maintained until return of bowel activity (Fig. 7). 8 TOGD resolved all gastroesophageal symptoms, allowing both enteral feedings and oral supplementation with no significant complications. Food aspiration was eliminated and respiratory problems were reduced such that hospitalization episodes were far less frequent. The children's well being improved with resumption of weight gain and a better QoL for both children and caregivers. There have been several reports on experience with TOGD2,19 with variable complication rates. Dall'Oglio et al. 16 and Gatti et al. 11 found that, when compared to fundoplication, TOGD offered better nutritional rehabilitation, a reduction in respiratory infections, and improved QoL with low rates of surgical morbidity and mortality. This was subsequently confirmed by Goyal et al.5,6,19 Such was the change that it was no longer possible to limit TOGD to “rescue following a failed fundoplication” and primary TOGD was recommended. Morabito et al. 7 described their 10 years' experience with TOGD as a primary (16 patients) and a “rescue” procedure (10 patients). There was no instance of recurrence of gastroesophageal reflux and the children's nutritional status improved statistically in both groups. De Lagausie et al. 18 extended the indications of TOGD to children with severe esophageal dyskinesis complicating EA, esophago-coloplasty, and tracheo-esophageal cleft. No complications were reported in the immediate postoperative course, and the procedure was recommended for definitively eliminating reflux in children with other severe malformations.

Patients with delicate neurologic, respiratory, and nutritional status benefit from the advantages of laparoscopy with reduced postoperative pain, better respiratory function, and less adhesions. 12 In a study of 7083 patients, 10 the laparoscopic approach had only 12% complications when compared with 25% for open surgery. There are few reports on the laparoscopic TOGD3,4 because of the difficulty with mobilization of the distal esophagus and the esophagojejunal anastomosis. 3 The robotic-assisted technique overcomes these difficulties. In our second case, the use of the robot allowed easier access despite the severe scoliosis and the baclofen pump (Fig. 8A–C). The three-dimensional view of the surgical field, the seven degrees of freedom, the stability of the operative field with magnified view, the scaling and filtering functions, and the wrist-like movements markedly enhance the laparoscopic intervention. A better view of the surgical field allows careful preservation of the posterior vagus nerve, meticulous suturing and anastomoses, and appropriate closure of all mesenteric windows. As in our fourth patient, when vagal nerve integrity is in doubt because of previous esophageal surgery, we routinely recommend a pyloroplasty as an integral component of the TOGD procedure. Gratifyingly, none of our patients encountered any of the major published complications, 17 most of which related to surgical expertize rather than the actual procedure. Our 4 patients, in common with the series reported in the literature showed complete resolution of vomiting and retching and a greater ease of feeding. As reported in other study, 19 parents and caregivers commented on the marked improvement in the children's' physical well being with a major reduction in respiratory “food aspiration and infections” and hospitalization episodes, “surpassing their expectations”. However, we agree that many others studies by validated QoL survey are needed to support these parental comments.

Surgical area strictly limited by the baclofen pump and the severe scoliosis.
In conclusion, TOGD has a positive impact on the physical well-being of children with ND and GORD. Our pilot study leads us to suggest that robotic-assisted minimally invasive laparoscopy overcomes the difficulties with access encountered with open or laparoscopic TOGD and has less postoperative complications, rendering the procedure eminently suitable for children with ND.
Footnotes
Disclosure Statement
This article has not been published in other journals. The authors did not receive financial support. The authors have no conflicts of interest.