
Abstract
Abstract
Introduction:
Bochdalek hernia is a congenital diaphragmatic defect that results from improper fusion of the septum transversum and the pleuroperitoneal folds. It rarely persists asymptomatic until adulthood. The reported incidence is as low as 0.17%. Surgical repair of the defect can be performed through the abdomen or through the chest, and in both cases open or through laparoscopy/thoracoscopy.
Case Report:
We present 2 cases of fully laparoscopic repair of giant Bochdalek hernia in adults. In both cases we used a GORE® DUALMESH® and we had neither complications nor recurrence. It is worthy of mention that hernia sac was not found in any of the cases. This has been described as a distinct characteristic that confirms diagnosis.
Conclusion:
Bochdalek hernia in the adult is a rare entity that requires surgical treatment to avoid complications. CT scan of the abdomen and chest with oral and IV contrast is the gold standard for diagnosis.
Introduction
B
Case Report
Case 1
Clinical presentation
This was a 36-year-old healthy woman whose surgical history was significant for mammoplasty. She did not have any history of trauma. She came to our clinic complaining of dyspepsia symptoms. She had been treated with proton pump inhibitors but reported poor response. She was evaluated initially at another institution; a posterior diaphragmatic hernia was suspected based on the chest X-ray results. Subsequently, a barium swallow, a barium enema, an esophagogastroduodenoscopy (EGD), a CT scan, and an MRI of the abdomen and chest were ordered at an outside hospital. She was referred to our clinic for evaluation and treatment. A giant Bochdalek hernia was diagnosed, where intestinal loops, colon, greater omentum, and the left kidney could be observed in the chest (Fig 1). The stomach was in the correct location. No hiatal or parahiatal defects were observed neither in the imaging studies nor in the EGD. Surgical treatment was decided; a laparoscopic repair with mesh and drainage of the pleural cavity was performed.
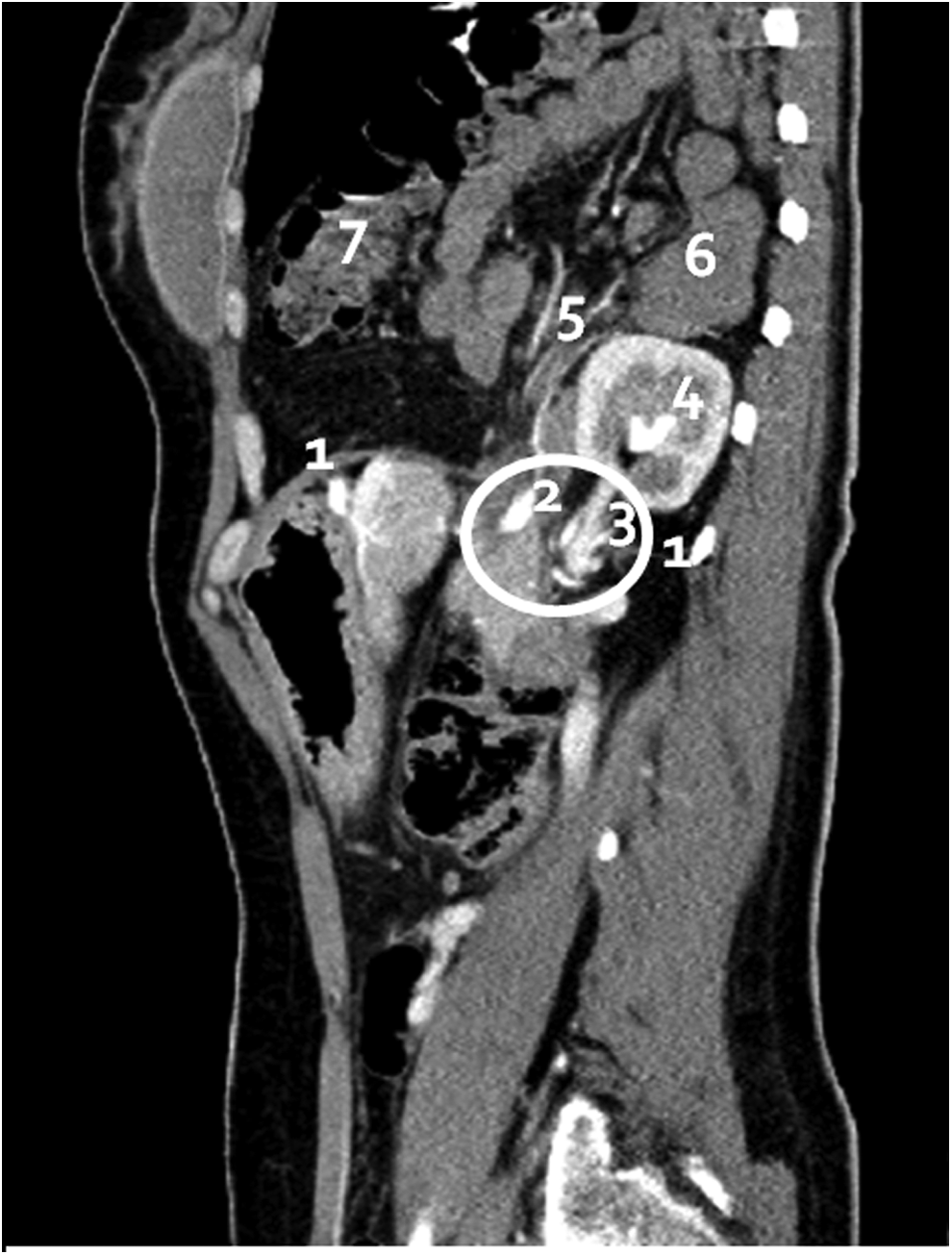
1, diaphragm; 2, hernia orifice; 3, kidney pedicle; 4, kidney; 5, mesentery; 6, small intestine; 7, large intestine.
Surgical technique
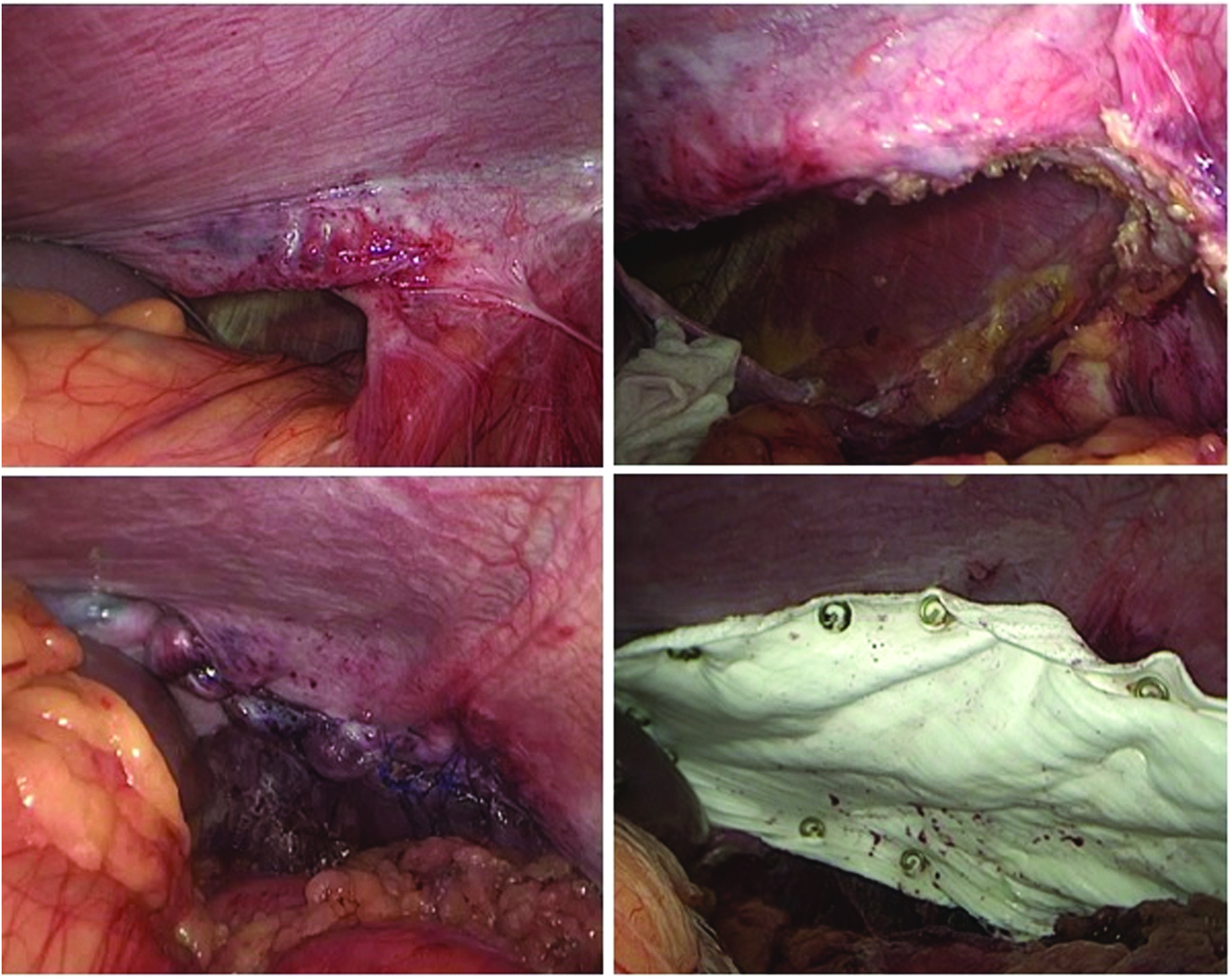
The patient was placed in a 30° right lateral decubitus position. The surgeon was positioned between the patient's legs and the assistant toward the left side of the patient. The operation was performed under general anesthesia. A double lumen endotracheal tube was used for ventilation. The skin of the abdomen was prepped and draped in the usual sterile manner. Four trocars were used: a 12-mm trocar was placed in the midline supraumbilical position under direct vision using the optiview® system, a 10-mm trocar was placed in the left flank (anterior axillary line), a 5-mm trocar was placed in the right upper quadrant, and another 5-mm trocar was placed in the left lower quadrant (mid axillary line). Once in the abdominal cavity, the stomach and the spleen were seen in place. We were able to confirm also the intraabdominal position of the gastroesophageal junction by retracting the left triangular ligament. The Bochdalek foramen was seen; the orifice measured about 10 × 7 cm. The superior edge was retracted. The colon was brought into the abdomen using atraumatic graspers. Subsequently, the greater omentum, the small bowel, and the left kidney were restored into the abdominal cavity. Reduction of the herniated organs was then completed. There was no hernia sac. The Bochdaleck foramen was completely freed up. The posterior edge of the foramen was liberated to facilitate its closure. Dissection was extended up to the spine. The left triangular ligament was transected and the spleen mobilized with the same purpose. We were able to obtain ∼6 cm of free margins. The defect was closed using a 2.0 Prolene running suture. Measurements were taken to place the mesh and cover the defect correctly. A 14 × 8 cm expanded polytetrafluoroethylene (ePTFE) material (GORE® DUALMESH®) was used. The mesh was fixed with nonabsorbable helicoidal tackers (Fig. 2). Next, a thoracic trocar was inserted and the lung was insufflated. The running suture closing the defect could be observed from above. A chest tube was left in place. The patient remained in the intensive care unit for the first 3 days on noninvasive positive pressure ventilation. She was started on liquids on post-op day 1. The chest tube was removed on post-op day 5 and she was discharged home on post-op day 7. At 12 months follow-up, she remained asymptomatic. A CT scan of the abdomen and chest showed no evidence of recurrence (Fig. 3).
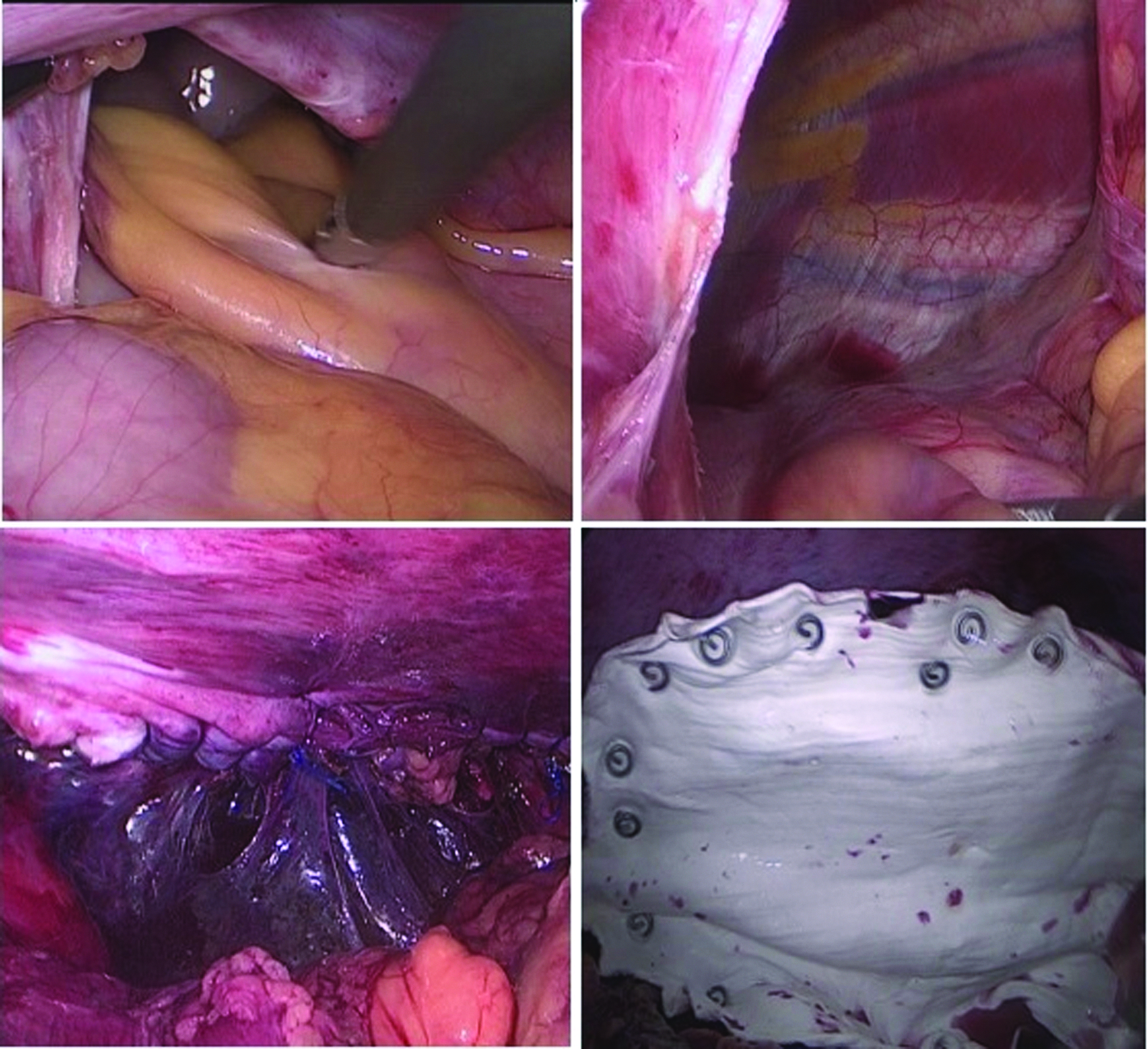
Top left: Bochdalek hernia; top right: hernia orifice; bottom left: closure; bottom right: mesh placement.
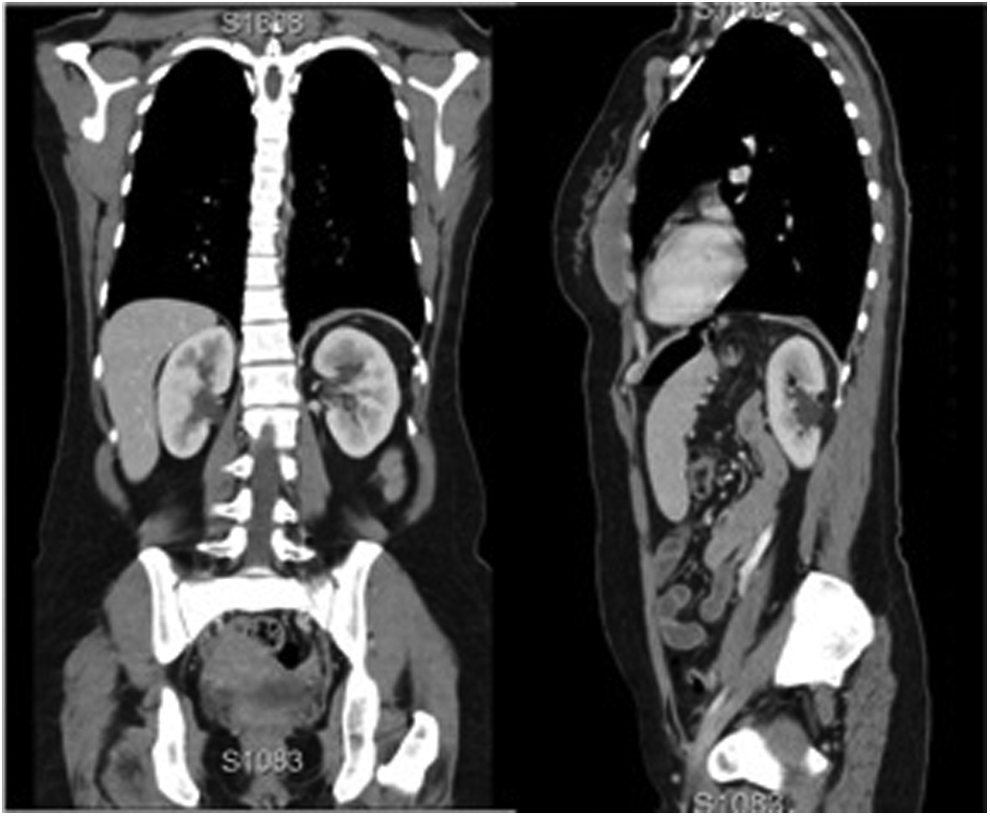
Postoperative CT scan.
Case 2
Clinical presentation
This was a 39- year-old man who presented to our clinic complaining of episodic headaches. His medical history was significant for cranioencephalic trauma 11 years before consultation. He referred that his wife heard some air–fluid sounds on his left chest. A chest X-ray showed the presence of herniated colon into the chest. CT scan clearly demonstrated a left posterior diaphragmatic hernia (Fig. 4). Laparoscopic repair was decided.
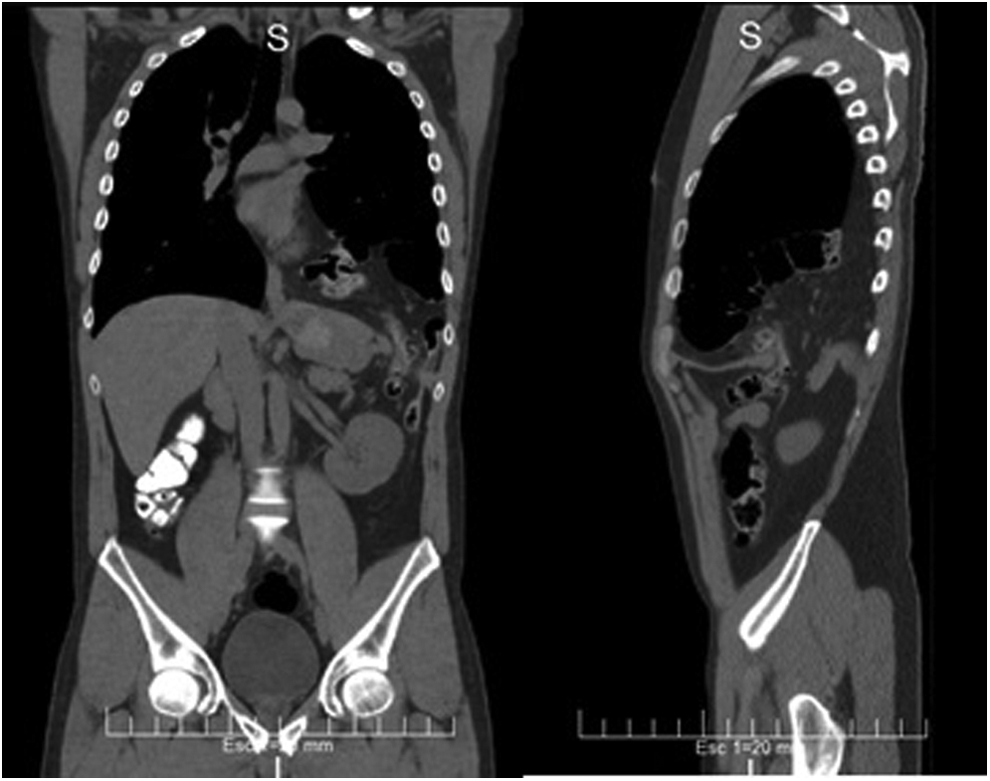
Second case preoperative CT scan.
Surgical technique
The patient was positioned as described in the first case. Once in the abdominal cavity, a big hernia orifice containing almost the entire colon was observed. The content was reduced into the abdomen using atraumatic graspers and harmonic scalpel. No hernia sac was found. The defect measured about 9 × 4 cm. The orifice was liberated for correct approximation of the edges. The defect was closed using 2.0 Prolene running suture. A chest tube was placed before the closure was completed. The lung was expanded under direct laparoscopic vision. A ePTFE material (GORE DUALMESH) was placed to reinforce the closure (Fig. 5). The patient was transferred to the regular floor and was started on liquids on post-op day 1. The chest tube was removed on post-op day 2, and he was discharged home on post-op day 3.
Top left: Bochdalek hernia; top right: hernia orifice; bottom left: closure; bottom right: mesh placement.
Discussion
Bochdalek hernia is a congenital diaphragmatic defect that results from improper fusion of the septum transversum and the pleuroperitoneal folds during the eighth week of gestation. They are usually found on the left side. This phenomenon might be because of the earlier closure of the right diaphragmatic side and the protection that the liver provides on the right side. 7 However, Mullins et al. 8 studied the prevalence and characteristics of adult Bochdalek hernia by reviewing 13,000 CT scans. They found that the frequency was 0.17%, the majority occurred in women (77%), and most cases were on the right side (68%). This finding would refute the theory that the liver protects from herniation. Still, this can be explained by the fact that right-sided hernias tend to be asymptomatic, whereas left-sided hernias are symptomatic and prompt the patient to seek consultation. 9
In fact, another recent literature review 7 including 173 symptomatic patients indicated that left hernias were found in 78% of the cases, and that distribution among men and women was equitable (55% and 45% respectively). Our report included 2 cases, 1 woman and 1 man, both with hernias on the left side. Only the first patient presented with symptoms at the time of consultation. It is worthy of mention that hernia sac was not found in any of the cases. This has been described as a distinct characteristic that confirms diagnosis. 10
Diagnosing Bochdalek hernia might be challenging because of its plurisymptomatic presentation. This includes restrictive respiratory and abdominal disorders that might lead to complications such as obstruction of the herniated organs and its dramatic implications. 11 Imaging tests are key during the evaluation process. Chest X-ray is typically the first test ordered, and it might be helpful in some cases where large defects are present. However, false negative results may occur in small defects, where the hernia contents are reduced into the abdominal cavity at the time of X-ray. 12 Although barium swallow and barium enema are categorical when the bowel is herniated, a paraesophageal hernia can be misdiagnosed for a Bochdalek hernia. 2 An MRI can be helpful for patients allergic to IV contrast. 13 Still, the gold standard for diagnosing this pathology is the CT scan with oral and IV contrast. 14 Possible intestinal malrotation should always be considered, since this diagnosis would force an abdominal approach.15,16
The first successful surgical treatment of a posterior diaphragmatic hernia was performed in 1901, although the first laparoscopic case was done in 1998. 17 There are less than 20 cases reported in the literature, but in only 6 of them the classic absence of hernia sac was described. 7
The primary closure of the defect was performed using running suture of Prolene material. Big bites were used to prevent muscle tear. Bochdalek defects are typically closed along their transverse axis in a medial to lateral manner. 7 The surrounding tissue was dissected as much as possible to have a tensionless closure. Prolene is a nonabsorbable, resistant, and easy-to-handle type of suture. Considering the difficult location where the surgeon needs to perform the suturing, this is not a minor feature.
The usage of mesh is still a matter of debate. Some authors 6 reported good results after hernia repair without mesh; however, if primary closure is being considered, the size of the defect and the tension should be evaluated before making a decision. Currently, dual layer meshes have been developed. These meshes are considered safe since they can be placed in contact with the viscera, with no related complications. Mesh anchorage on the diaphragm is a delicate issue because of the risk of inadvertent cardiac injury resulting in a fatal tamponade, a very rare but catastrophic complication. In a survey of hiatal hernia repair among Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) members, sutures were the most common choice used by more than half of the respondents (56.4%), followed by tacks (23.9%). There were no cardiac injuries reported in this study. 18 Despite this, Frantzides reported a review of 15 cases of cardiac tamponade during hiatal and ventral hernia repair where 11 cases were caused by helicoidal tackers, 2 by suture, 1 by the straight stapler, and 1 not stated. In every one of these 11 cases, tacks were used for fixation of the mesh to the central tendon of the diaphragm. 19 Bochdalek hernia has an anatomical advantage regarding this particular point, as it is originated in the posterior mediastinum because of an improper fusion of the septum transversum and the pleuroperitoneal folds; this means that usually these types of defects are located apart from the middle mediastinum and the central tendon of the diaphragm where cardiac injury might take place as it could happen in hiatal and ventral hernias (Fig. 6). Moreover, the size of the defect in both cases allowed us to have a direct view of the location of the pericardium (Fig. 7), letting us use tackers safely. The lung was chronically collapsed because of the size of the hernia and the double lumen endotracheal tube used for ventilation allowed us to keep it collapsed after hernia reduction to work on the closure without trouble. When anchoring the mesh to the diaphragm, it is necessary to consider the risk of injury to the heart with the consequent cardiac tamponade, especially if the helical tacker is used in the central region. Only with appropriate awareness and recognition can this catastrophic complication be avoided. 19 Other authors also recommend the use of a prosthetic graft when the defect is larger than 8 cm in diameter 20 or 25 cm2. 21 Particularly, in our experience with the 2 cases already presented, we did not hesitate in using mesh for the repair. Finally, the continuing stress on the diaphragm that results from respiratory movements and cardiac motions is another particular factor to be taken into account in these cases. 12 In our experience, laparoscopic repair with mesh demonstrated to be a safe technique. None of the cases described presented complications or recurrence. Lung expansion usually occurs slowly over time because of chronic collapse. For this reason, we decided to place a chest tube in an attempt to diminish the dead space after hernia reduction. Moreover, the thoracic and the abdominal cavity remained directly connected with the consequent risk of pneumothorax and pneumoperitoneum. 22
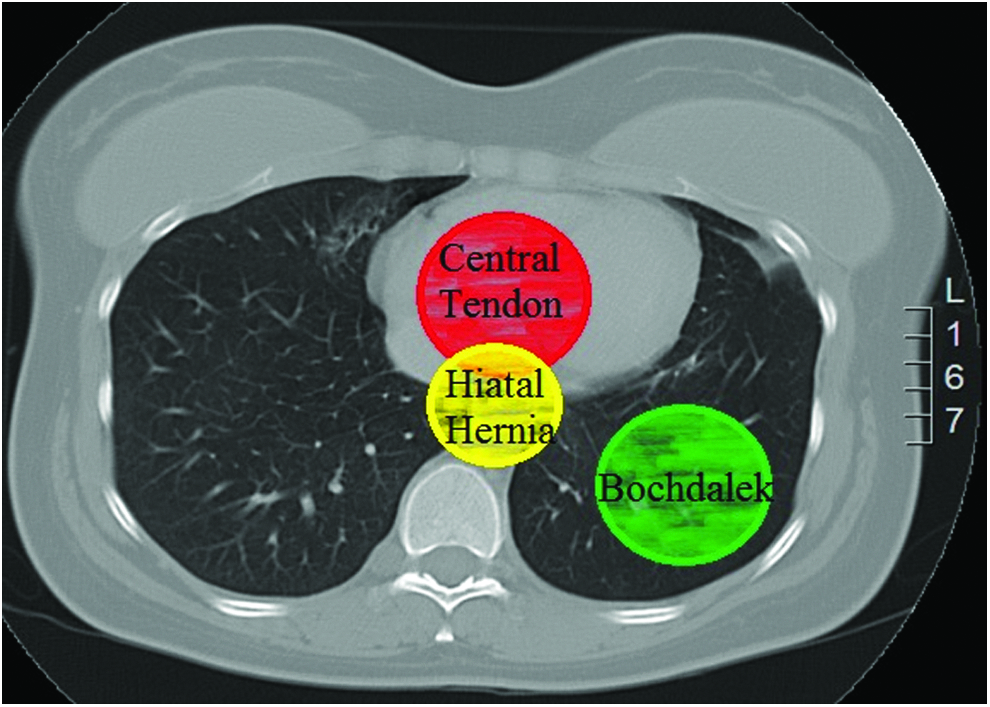
Bochdalek anatomical advantage.
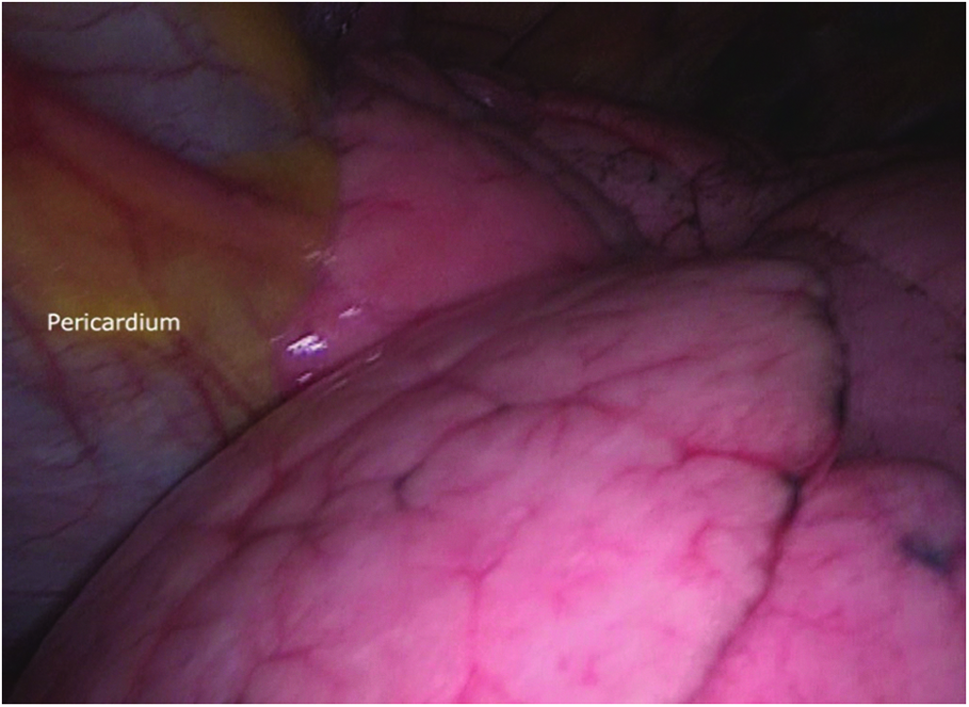
Direct view of lung and pericardium through hernia's orifice.
Conclusion
Bochdalek hernia in the adult is a rare entity that requires surgical treatment to avoid complications. CT scan of the abdomen and chest with oral and IV contrast is the gold standard for diagnosis. Laparoscopic approach has demonstrated to be safe and effective.
Footnotes
Disclosure Statement
No competing financial interests exist.