
Abstract
Abstract
Aim:
To compare the outcome of patients who had undergone single-incision laparoscopic appendectomy (SILA) with others who had undergone three-port laparoscopic appendectomy (3-PORT).
Materials and Methods:
Data from all adults with uncomplicated appendicitis treated by laparoscopic appendectomy between June 2012 and December 2015 were prospectively collected. Patients with chronic pain, appendix malignancy, at least two previous laparotomies, and those undergoing concomitant surgery for different condition were excluded from analysis. Postoperative pain was assessed by a visual analog scale (VAS). Patients were reviewed postoperatively at 7 days and 1 month in the outpatient clinic. Late complications were assessed with a telephonic interview.
Results:
A total of 91 patients were included (46 SILA; 45 3-PORT). There were 16 males and 30 females in the SILA group (mean age = 26.76 ± 10.58 years) and 18 males and 27 females in the 3-PORT group (mean age = 26.84 ± 10.79 years). The mean operative time for SILA was 48.54 ± 12.80 min, for the 3-PORT group the mean operative time was 46.33 ± 15.54 min (P = 0.46). No case required conversion. Mean postoperative hospital length of stay was 1.87 ± 0.69 days for SILA and 2.38 ± 1.11 days for 3-PORT (P = 0.01). VAS value of 3.91 ± 1.96 and mean ketorolac usage of 0.38 ± 0.65 in 3-PORT group and SILA patients reported 3.70 ± 1.58 and 0.39 ± 0.58, respectively (P = 0.91). Our mean follow-up in SILA group was 25.75 ± 10.82 months, for 3-PORT group the mean follow-up was 26.9 ± 11.8 months. Eleven patients missed long-term follow-up. No incisional hernia was found. There is a statistically significant difference in cosmetic evaluation in favor of SILA (P < 0.005).
Conclusions:
There was no difference in operative time, early complications, postoperative pain, analgesia requirement between SILA and 3-PORT laparoscopic appendectomy, but after SILA procedure discharge was quicker and long-term cosmetic satisfaction was superior.
Introduction
A
Since the first laparoscopic cholecystectomy was described by Muhe in 1985, and later published by Mouret, Perissat, and Dubois in 1987 and 1988,5–7 this kind of surgery has made huge progress, becoming the standard procedure for many intraabdominal surgeries.
One century after the first appendectomy codified by McBurney, 8 in 1977 the Dutch surgeon Hans de Kok 9 performed the first laparoscope-assisted appendectomy. News of this technique reached only a few because of its publication in an article that was only diffused locally, until Semm, 10 a German gynecologist, published the first laparoscopic appendectomy in 1983.
Appendectomies were being carried out with a single puncture as early as 1992, 11 the appendix was coaxed out of the umbilicus to complete the task after cecal mobilization. 12 In more recent years, there have been descriptions of this with transumbilical flexible endoscopy. 13
After that the use of multiple trocars gained popularity over the disadvantages of a single puncture. As even complex surgical procedures started to use conventional laparoscopy, four or more ports were generally used. The use of more ports meant reduced cosmesis, increased pain, and higher risk of complications, because of port site infections and hernias.14,15 One advantage of reducing the number of ports over cosmesis would be to reduce these complications.
The quest for scar reduction beyond standard laparoscopy led to experimentation with natural orifice surgery. The first description of the procedure to be known as natural orifice translumenal endoscopic surgery (NOTES) is attributed to Kalloo et al.16,17
In 2008, Rao et al. for the first time were able to perform a cholecystectomies case series 18 and they proposed the idea that access into the abdominal cavity could be concealed by the umbilicus, as this was an ubiquitous cicatrix from birth.
Ates et al. published in the same period, a case series of appendectomies with a single access device with two operative channels full intracorporeal performed. Since then, there has been a spread of interest in single-incision laparoscopic surgeries. 19
The safety and feasibility of this technique have already been described in the literature by many series of cases and more recently also by randomized controlled trials.20–22
The advantages set forth, such as the reduction of postoperative pain, earlier discharge, and a better aesthetic result, are still being debated, as were also emphasized in the recent reviews. 22
This study aims to help clarify these key issues as well as report the long-term results on the incidence rate of incisional hernia of the trocar site as these data are lacking in the literature.
Materials and Methods
This study analyzed a dedicated database that had been prospectively collected. From June 2012 to December 2015, 91 adults with clinical or sonographic signs of uncomplicated appendicitis were included.
Patients with complicated acute appendicitis, appendix rupture or perforation, peritonitis, or local abscess were excluded.
Patients whose appendectomy was performed as part of another laparoscopic procedure and patients who had undergone two or more laparotomies were excluded from the investigation.
All patients were operated by 2 surgeons. Both surgeons were experienced in laparoscopic appendectomies, and they had undergone basic single-incision laparoscopic surgery training.
The decision to perform a single-incision laparoscopic appendectomy (SILA) procedure or a multiport laparoscopic appendectomy was made according to the surgeon's assessment of the patient in question and the patient's choice. Patients were fully informed preoperatively about both treatment options and the possible advantages and limitations of both techniques. Our records included patients' personal information, operating time, appendectomy technique, complications, pain (visual analog scale [VAS]), pain medication request, hospital stay, histopathological result, and follow-up.
Operating time was defined as the time from the skin incision to skin closure. Each patient was asked to self-estimate the severity of abdominal pain using a VAS, with scores ranging from 0 (no pain) to 10 (the worst pain imaginable) on the day of operation and postoperative day 1 (Fig. 1).

VAS Scale.
All patients received prophylactic antibiotic treatment preoperatively and it was continued postoperatively according to the surgeon's instructions and the macroscopic characteristics of the appendix.
During the postoperative period, patients received intravenous (IV) therapy with fluid and 1 g of paracetamol three times a day, and IV ketorolac tromethamine 30 mg/mL as needed for pain control.
All patients were allowed a clear liquid from 12 hours after surgery, and the diet was advanced as tolerated. The length of hospital stay was calculated as the time from operation to discharge. Patients were discharged at the time of first flatus and they were reviewed in the outpatient clinic at 1 week and 1 month after surgery.
Patients were asked to assess late complications and cosmetic results during a telephone interview and to e-mail us a photo of their umbilicus, if they consented to this.
Operative Technique
Conventional laparoscopic appendectomy
The operation was performed under general anesthesia with the patient in a supine position. An orogastric tube and Foley catheter were inserted. The surgeon and scope operator were positioned to the left of the patient, the monitor was located in front of them, to the right of the patient.
A 10-mm laparoscopic trocar was inserted into the umbilicus, using the Hasson technique to access the peritoneum. The abdomen was insufflated with CO2 to a pressure of 12 mmHg, after establishment of the first port. Two additional trocars were inserted under vision, a 10 mm trocar in the suprapubic area and a 5 mm trocar in the mid lower abdomen.
The patient was then placed in the Trendelenburg position, with the left side down. We used a 30° 10-mm laparoscope and standard rigid 5-mm laparoscopic instruments. Diagnostic laparoscopy was always performed. The mesoappendix was divided using bipolar coagulation. The base of the appendix was ligated using three endoloops or linear endostaplers, according to the surgeon's preference and flogistic conditions. The appendix was removed using a laparoscopic endobag. Intraabdominal saline irrigation was performed. No drains were inserted. The umbilicus 10-mm port site was closed using one absorbable suture and skin incisions were closed with 3-0 nonabsorbable monofilament sutures.
SILA
Patients were prepared and put into the same position as for the three-port appendectomy. The umbilicus was everted by two clamps placed on either side of midline. A vertical skin incision of 2 cm was performed. The fascia was prepared and a 4 cm vertical incision was made.
The incision was pulled up with clamp and a single-port (multichannel) device was added. Three trocars (5 mm) were placed in the SILS device and the abdomen was insufflated to 12 mmHg with CO2 gas (Fig. 2).
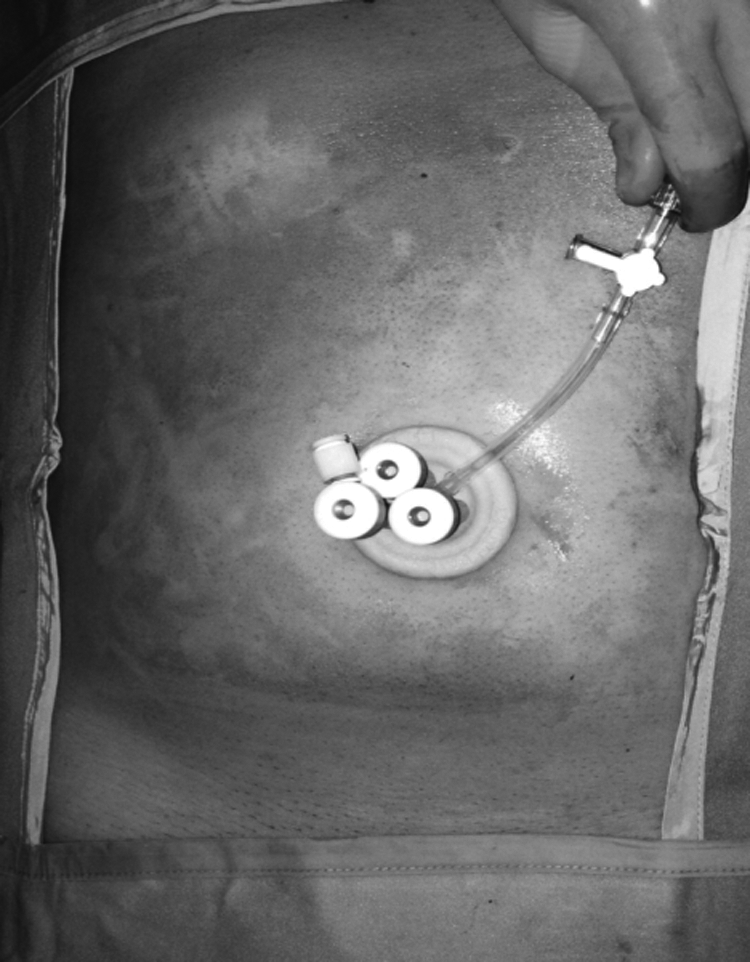
Single-port positioned.
Diagnostic laparoscopy and appendectomy were then performed using the same instruments as the standard technique, but for a 30° 5 mm laparoscope. The fascia was closed using one absorbable suture and the skin with a 3.0 nonabsorbable monofilament suture.
Small gauzes were inserted into the umbilicus and then the medication dressing was applied.
Results
Statistical analyses between the two groups were based on the independent t-test, χ2 test, and the Fisher exact test, and a multivariate analysis was also performed. A P < 0.05 was considered to be statistically significant.
We included 91 adult patients.
In the 3-PORT group, we had 18 males and 27 females with mean age of 26.84 ± 10.79 years, whereas in SILA group we had 16 males and 30 females with a mean age of 26.76 ± 10.58 years (P = 0.78) (Tables 1 and 2).
SILA, single-incision laparoscopic appendectomy.
SD, standard deviation; SE, standard error; SILA, single-incision laparoscopic appendectomy.
Table 3 shows patient distribution into two groups from 2012 to 2015 and there is no statistically significant difference, nevertheless there is a more frequent use of single-incision laparoscopic technique with the passage of time.
SILA, single-incision laparoscopic appendectomy.
We analyzed the demographical patient characteristics, and the population in the two groups had similar age, weight, body mass index, gender, and surgical history (P = 0.84).
To detect inflammation or other pathologies, all specimens were subjected to histological investigation. Three groups were identified according to the histological report: nonspecific inflammation (infiltrated with histiocytes and monocytes without neutrophils), exudative-productive inflammation (infiltrated with neutrophils, lymphocytes, histiocytes, and plasma cells), and purulent inflammation (with the presence of granulocyte). In this case, no statistically significant differences were observed between the groups (P = 0.46) (Table 4).
SILA, single-incision laparoscopic appendectomy.
All the operations were completed safely and without vascular, visceral injury. No patient had to be converted to the multiport or open procedure.
The appendix base was ligated with an endostapler in 32 cases for the 3-PORT group and 35 cases for the SILA group, whereas endoloops were used 13 times in three-port appendectomies and 11 times for the SILAs (P = 0.86).
The operative time was similar between the two groups (3-PORT 46.33 ± 15.54; SILA 48.54 ± 12.80). The SILA technique was 2.2 minutes longer than the three-port appendectomy technique without any statistically significant difference (P = 0.46).
The operating time for each histological subgroup for the two surgical techniques increased with the progression of inflammation (P = 0.15) (Table 5).
SD, standard deviation; SE, standard error; SILA, single-incision laparoscopic appendectomy.
The operative time was not influenced by which surgeon performed the appendectomy (Table 6) (P = 0.87).
SD, standard deviation; SE, standard error; SILA, single-incision laparoscopic appendectomy.
Pain on the first postoperative day was evaluated using the VAS and the amount of ketorolac requested. In the 3-PORT group, we had a mean VAS value of 3.91 ± 1.96 and a mean ketorolac usage of 0.38 ± 0.65 and those for the SILA patients were 3.70 ± 1.58 and 0.39 ± 0.58, respectively, without any statistically significant differences (Tables 7 and 8) (P = 0.91). There is a possible correlation between VAS and the patient's sex, in fact males reported a mean VAS value of 3.38 ± 1.50 whereas females reported 4.05 ± 1.88 with a border line P value, where P = 0.08. There is a correlation, without statistically significant difference between ketorolac request (vials) and gender: males showed a mean amount of ketorolac of 0.26 ± 0.57 and females reported a mean amount of ketorolac of 0.46 ± 0.63 (P = 0.15), but there is no statistically significant difference.
SD, standard deviation; SE, standard error; SILA, single-incision laparoscopic appendectomy; VAS, visual analog scale.
SD, standard deviation; SE, standard error; SILA, single-incision laparoscopic appendectomy.
As could be expected, the amount of ketorolac increased as the histological feature worsened, without any statistically significant differences however (P = 0.54).
Hospital stay reported for three-port patients was with a mean value of 2.38 ± 1.11 days and for that for SILA patients as 1.87 ± 0.69 days with a statistically significant difference (P = 0.01) in favor of single-incision appendectomy (Table 9). We also observed a prolongation of hospital stay with the worsening of histology but without any statistically significant differences (P = 0.11).
SD, standard deviation; SE, standard error; SILA, single-incision laparoscopic appendectomy.
Multivariate analysis confirmed the statistical difference between the two groups in terms of hospital stay, with shorter recovery for SILA patients.
We evaluated short-term complications such as bleeding, abscess, dehiscence, conversion to multiport laparoscopy or laparotomy, and scar infections, during the hospital stay, and we reviewed patients in the clinic at 7 days and 1 month postoperatively. All patients attended short-term follow-up. In the SILA group, we had a patient with a short-term complication; she complained of intense scar pain for 3 weeks. We evaluated the long-term results, such as the cosmetic appearance and incidence of incisional hernia with a telephone interview. We submitted a questionnaire over the telephone to assess the aesthetic results and incidence of incisional hernia (Table 10). Our mean follow-up in the SILA group was 25.75 ± 10.82 months with a median of 26 months. In the SILA group, 6 patients missed their long-term interview (13%). The evaluation was good, with quantitative score ≤9 in 6 (15%) cases and excellent with quantitative score > 9 in 34 cases (85%). No one complained of bulging, incisional hernia, or pain in the scar area (Fig. 3).
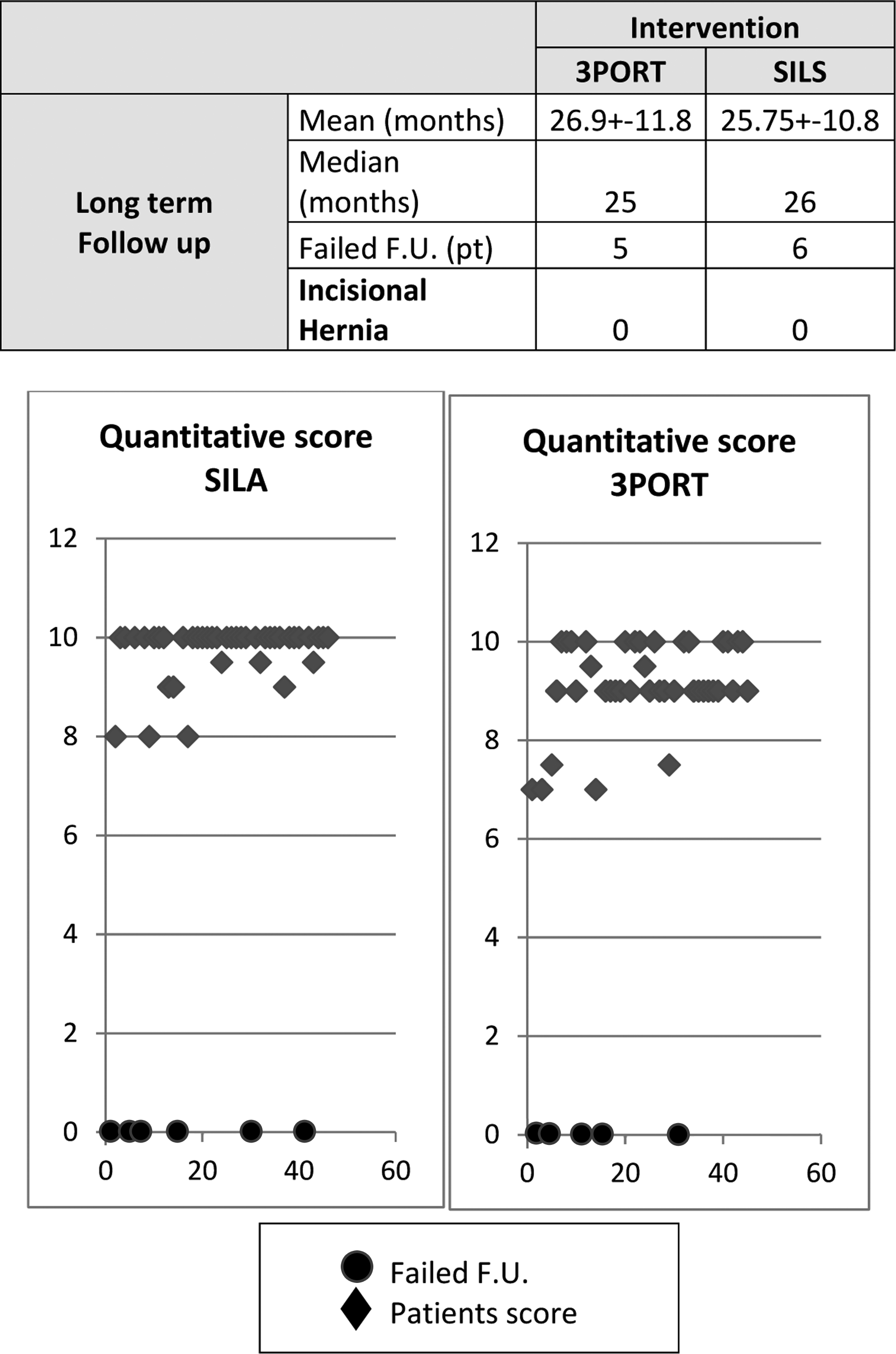
Long-term follow-up.
In the 3-PORT group, we had 2 cases of short-term complications: urinary tract bleeding and a reoperation for a suspected dehiscence of the appendicular stump, but a laparoscopic procedure excluded the presence of surgical complications. Mean long-term follow-up was 26.9 ± 11.8 months and a median of 25 months; 5 patients missed the interview (11%) and the evaluation was good with quantitative score ≤9 in 24 patients (60%) and excellent with score > 9 in 16 patients (40%). We did not find any incisional hernia in this group either. There is a statistically significant difference in cosmetic evaluation between the two groups in favor of single-incision appendectomies (P = 0.0038).
Discussion
Single-incision laparoscopic surgery is of interest in the laparoscopic field because of the promise of a “scarless” abdomen.
In the literature there are small case series, 23 and more recently some randomized controlled trial (RCT)24,25 about SILAs.
A recent review confirmed the feasibility and safety of this procedure without significant differences between single-port and three-port appendectomies. 22
For this reason, SILA is shown as a good choice for the treatment of appendicitis, but more studies are needed to define which kind of patients would have the best results and benefit from using SILA. 26
A long-term follow-up is frequently requested in the literature to evaluate incisional hernia incidence, which is one of the most important issues in this field. 27
The aim of our study was to compare two methods in a selected patient population to evaluate the potential benefits of SILA. We also aimed to fill the gap present in the literature regarding long-term follow-up of patients.
We included adult patients with suspected acute appendicitis on clinical and ultrasound grounds, and we excluded patients in line with the exclusion criteria as follows:
• Complicated appendicitis. • Two or more previous laparotomies. • Oncological pathology. • Appendectomy performed in a combined laparoscopic intervention. • Chronic pain requiring daily medications.
We analyzed data on 91 laparoscopic appendectomies, in a uniform population for all parameters.
The two methods are similar, without significant differences, regarding intervention and postoperative treatment, although the SILA operative time is 2.2 minutes longer, without statistically significant differences.
We explain this difference with our learning curve for the SILA procedure.
Linear regression shows a gradual reduction in operating time without no plateau reached as yet, so we expect that our operating times may reduce even further (Fig. 4).

SILA operative time.
In our experience, hospital stay is shorter for SILA patients. We can explain this result by reduced trauma to the abdominal peritoneum by the surgical incision, despite the umbilical fascial incision being longer than that for the three-port patients. It is, however, located in just one site and this could explain the reduced trauma to the abdominal cavity and a shorter time before first flatus. This means a quicker return to normal activities.
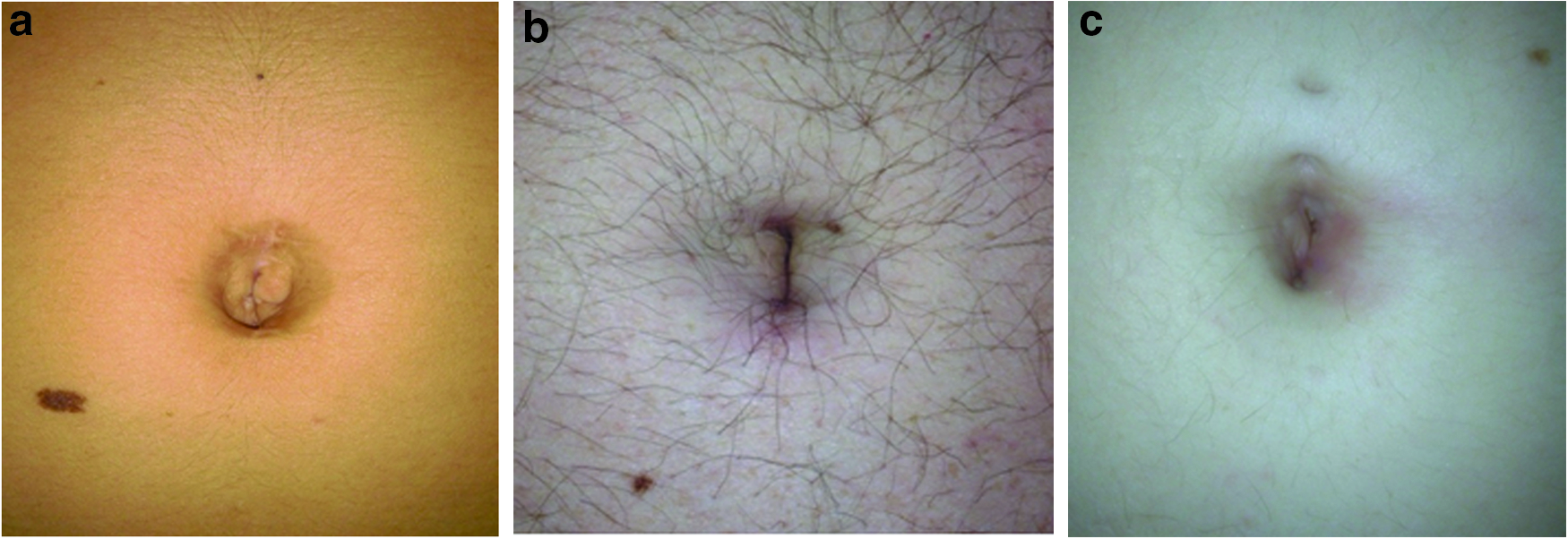
The long-term follow-up answered the issue of incisional hernia, and it revealed no difference between the two methods, whereas we found a statistically significant difference in cosmetic satisfaction in SILA patients. We explained this with the complete disappearance of the scar inside the umbilicus and the restoration of an apparently “scarless” abdomen 6 months after surgery. Patients in the three-port group were satisfied with the aesthetic result, but they explained that the scars, small and pleasant, remain mostly visible, whereas patients in the SILA group were happily surprised by the total absence of signs of surgery (Figs. 5–7).


The SILA entailed a shorter hospital stay and it improved long-term cosmetic results, in selected patients.
These results answer the question as to whether SILA can improve patient outcomes when compared with multiport laparoscopy.
We can recommend the use of single-port appendectomy for uncomplicated appendicitis, in young patients, in patients interested in their body image, without worries about the incidence of incisional hernia in the long term.
Footnotes
Disclosure Statement
No competing financial interests exist.
Acknowledgments
The authors thank Dott. L. Boni and Dott. M. Tarocchi for help in statistical analysis.