
Abstract
Abstract
Surgical correction of achalasia using laparoscopic Heller myotomy with Dor fundoplication is argued to be the gold standard treatment for patients with achalasia. The goal of this technical report is to illustrate our preferred approach to patients with achalasia and to provide the reader with a detailed description of our operative technique, its rationale, and our pre and postoperative management.
Introduction
A
Ultimately, 5% of patients with achalasia will progress to end-stage achalasia requiring esophagectomy. Recent large population studies suggest an overall 2.2%–3.4% total risk of developing esophageal carcinoma with the majority (1.3%–2.7% of cases) as squamous cell carcinoma.11,12
The goal of this technical report is to illustrate our preferred approach to patients with achalasia and to provide the reader with a detailed description of our operative technique, its rationale, and our pre- and postoperative management.
Preoperative Care
Dysphagia, regurgitation, retrosternal pain, heartburn, respiratory symptoms, and weight loss are the most common symptoms. 13 While in the past many different parameters were used to evaluate the effect of treatment, today the Eckardt score is universally used. 14 It is based on four elements (weight loss, dysphagia, regurgitation, and retrosternal pain) and it varies from 0 to 12. A score of 3 or less is considered an excellent result, while a score of more than 3 is indicative of treatment failure.
The gold standard test in diagnosing achalasia is esophageal manometry. High-resolution manometry led to the development of the Chicago Classification in 2008 that separated patients into three different classes (type I, II, and III), each with different responses to surgical correction. 15 The esophageal manometry has also been shown to be extremely helpful for patients classified as having refractory gastroesophageal reflux disease (GERD). Some of these patients present with an abnormal pH monitoring score that is not due to real reflux but, instead, is a consequence of stasis and fermentation of foods, a phenomenon so-called pseudo reflux, hiding the actual diagnosis of achalasia and leading the surgeon to perform the wrong operation. 16
Esophagogastroduodenoscopy is utilized to rule out pseudoachalasia and candidal infections of the esophagus, which mandated medical treatment with antifungal agents.
The barium swallow helps confirm the diagnosis of achalasia with tertiary contractions of the esophagus, bird's beak appearance of the distal esophagus into the LES, and esophageal dilatation and tortuosity. In addition, the barium swallow may identify epiphrenic diverticula often associated with achalasia.
Description of the operative technique
Positioning and port placement
The patient is placed supine on the operating table over a beanbag. Usually, a rapid sequence intubation is performed by the anesthesiologist to minimize the risk of aspiration, especially in patients with a dilated esophagus. In the presence of a sigmoid esophagus and megaesophagus, a nasogastric tube is placed to facilitate emptying of esophageal contents. We have found that over the years although patients are instructed to have nothing to eat or drink the night before the operation, the esophagus may contain several liters of fluid. As a result, the patient is at a high risk for aspiration during induction of anesthesia. Therefore, we do recommend a clear liquid diet for 48 hours before surgery to decrease the solid food burden in the esophagus.
A Foley catheter is rarely inserted and the lower extremities are placed in a semi-lithotomy position on stirrups. The beanbag is inflated to form a saddle that will support the patient in a steep reverse Trendelenburg position. The surgeon stands between the patient's legs while the assistant stands on the patient's left side.
Port placement is illustrated in Figure 1. Four 11 mm ports are placed and a 5 mm incision is made immediately to the left of the xiphoid process for placement of a Nathanson retractor. This retracts the left lobe of the liver to expose the esophageal hiatus. The optical trocar is placed about 15 cm from the xiphoid process in the midline; the two operating trocars are placed below the right and left costal margins at the level of the mid-clavicular line. The trocar used to insert the energy device to transect the short gastric vessels and for stabilizing the gastroesophageal junction while performing the myotomy is placed at the level of the optical trocar at the left anterior axillary line. A 10 mm 30° laparoscope is always used.

Position of operative ports and liver retractor.
Once all ports are placed, the patient is positioned in steep reverse Trendelenburg to allow gravity to retract the abdominal organs inferiorly to provide optimal exposure of the distal esophagus and proximal stomach.
Mobilization of the distal esophagus
An Allis clamp is applied near the gastroesophageal junction to lift the gastrohepatic ligament. This ligament is then divided to expose the right pillar of the crus. The esophagus is then bluntly dissected away from the right crus while the Allis clamp provides gentle downward traction to the gastroesophageal junction, thus, allowing for the myotomy. In cases with a sigmoid esophagus, the dissection is carried into the posterior mediastinum to straighten the axis of the esophagus. The esophageal fat pad, which lies anteriorly to the esophagus in the abdomen, is excised to identify the angle of His that separates the esophagus from the stomach. This provides exposure to the anterior wall of the stomach that is subjected to the cardiomyotomy. Additionally, the exposure of angle of His provides the surgeon with a reference point to assess the distal extension of the cardiomyotomy itself.
Myotomy
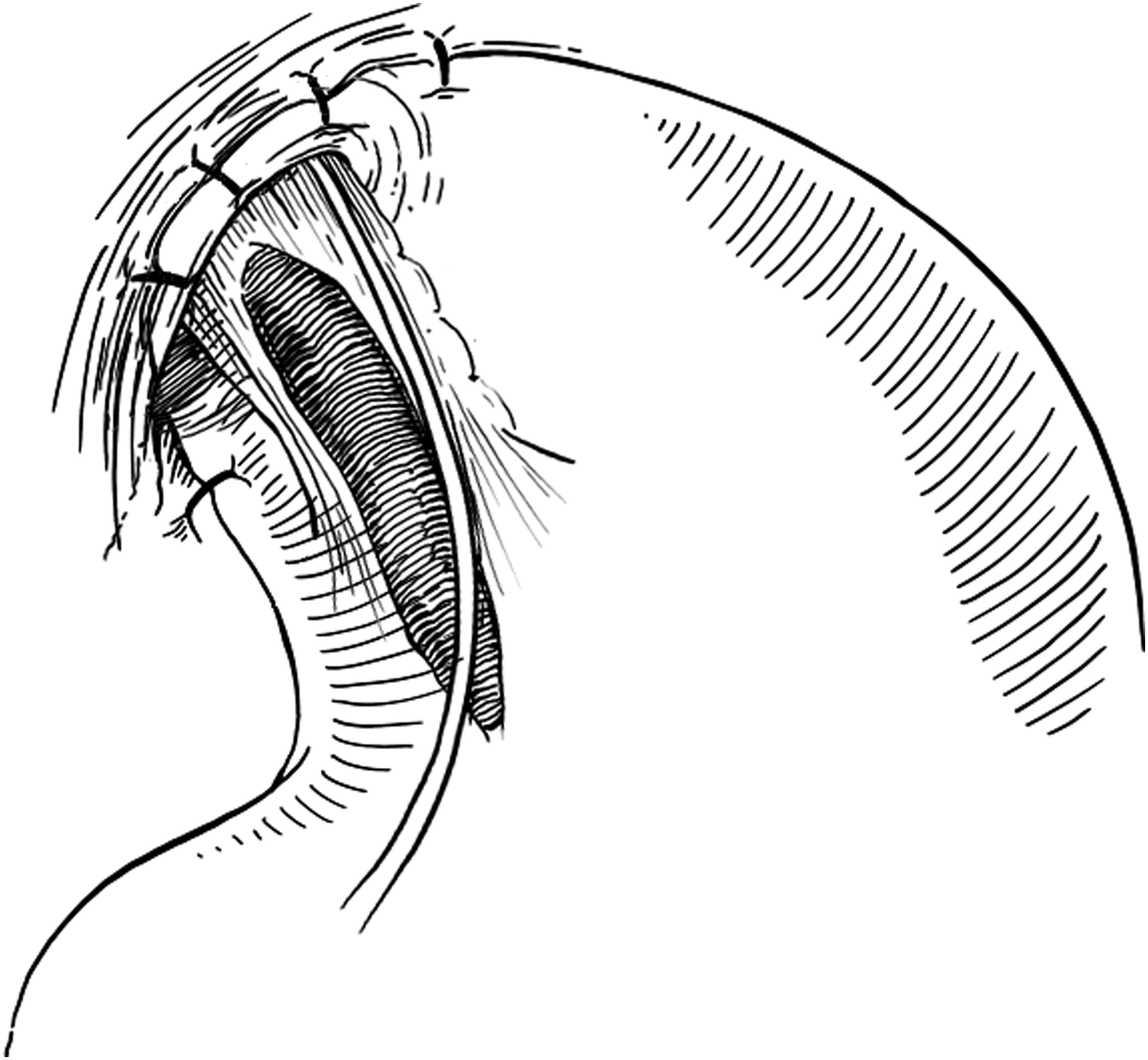
The cardiomyotomy is extended 7 cm cranially onto the esophagus and 3 cm caudally onto the anterior wall of the stomach until approximately the level of the first branch of the left gastric artery. The gastric extension of the myotomy is often the most difficult part of the operation, because it entails in dividing the clasp (or “U”) fibers described by Lieberman-Maffert et al. 17 This is the reason why the myotomy is usually started above the gastroesophageal junction, where the surgical planes between the longitudinal and circular muscle fibers are more consistent. During the myotomy the anterior vagus nerve is preserved (Fig. 2). The cardiomyotomy therefore is performed at the 10 o'clock position, onto the right anterolateral aspect of the esophagus, between the anterior and posterior vagal nerves. Two indicators of a well executed myotomy are the complete outpouching of the submucosa, which means that all small circular fibers have been transected, and a large transverse area of the exposed submucosa, which may reduce the incidence of recurrent dysphagia, an event probably related to fibrosis and bridging of the edges of the myotomy.

A cardiomyotomy and its relationship with the anterior vagus nerve are shown. A cardiomyotomy 10 cm long located at the 10 o'clock position extends onto the body of the esophagus and distally 3 cm onto the anterior wall of the stomach.
The myotomy is performed by stabilizing the anterior wall of the stomach near the gastroesophageal junction with an Allis clamp inserted from the assisting trocar positioned in the lower left upper quadrant. The myotomy is then accomplished by tearing down the longitudinal and circular fibers sharply with fine graspers or alternatively by using the laparoscopic hook cautery paying attention to avoid a perforation. However, it has been shown that patients are at an increased risk of perforation if they have undergone several previous botox injections, as botox may cause fibrosis and distortion of the normal anatomic planes. 3 If a perforation is encountered, it is repaired laparoscopically with interrupted fine (3–0 or 4–0) absorbable sutures tied intracorporeally and the repair is then covered by the Dor fundoplication (a drain is then positioned). During the myotomy, minor bleeding may ensue from small vessels in the esophageal submucosa. In these instances, bleeding is always controlled by applying pressure with gauze inserted in the operative field. Using a laparoscopic hook cautery to control the bleeding often results into a perforation of the submucosa.
We seldom perform an upper endoscopy intraoperatively, except in very difficult cases and during reoperations. Usually, an upper endoscopy is performed to rule out a perforation and to confirm the intragastric extension of the myotomy. However, as we routinely extend the myotomy onto the stomach and perform an anterior fundoplication to cover any potential perforation, we rarely feel the need to perform an upper endoscopy in all cases.
Dor fundoplication
The short gastric vessels are divided with an energy device inserted from the assisting trocar positioned in the lower left upper quadrant. Complete mobilization of the fundus is achieved also by taking down the posterior gastric artery that provides blood supply to the proximal uppermost portion of the posterior wall of the stomach. The gastric fundus is then sutured laterally to the apex of the left crus and the left edge of the myotomy. The gastric fundus now free of any tension posteriorly is folded completely over the myotomy and sutured superiorly along the diaphragmatic hiatus and medially along the right edge of the myotomy with 2–0 silk interrupted sutures (Fig. 3). A 180° anterior fundoplication first described by Andre' Dor in 1962 is therefore completed. 18 It is important to note that when the body of the stomach is used for the fundoplication, or when the fundus is anchored to the right pillar of the crus instead of the right edge of the myotomy, one may cause a narrowing of the esophageal lumen with resultant persistent dysphagia.
Completed partial anterior fundoplication.
Postoperative Care and Follow-Up
Upon completion of the operation, the nasogastric tube is removed before extubation. The patient is then admitted overnight. On postoperative day 1, the patient receives a diet. A barium swallow is seldom ordered before resuming a diet, unless a perforation is suspected in difficult cases. The patients are instructed to keep a soft-mechanical diet (e.g., cream of wheat, scrambled eggs) until the first clinic appointment when they are instructed to start an unrestricted diet.
While there is no consensus on patient surveillance, Zaninotto et al. recommend an endoscopy every 3–4 years. 19 This operation does not completely minimize the risk of esophageal squamous cell cancer. We also recommend an upper endoscopy every 3 to 4 years in asymptomatic patients, and immediately in patients with recurrent dysphagia.
Complications, Failures, and Management of Megaesophagus
The most common complication of a Heller myotomy is an esophageal perforation. When recognized intraoperatively, a small perforation can be dealt with laparoscopically as described above. When the perforation is too large for a primary repair, an esophagectomy is indicated. This event is more likely to occur during reoperations or when the patient has received several botox injections. 3 Therefore, in such instances the patient needs to be carefully counseled preoperatively about this potential risk. Conversely, when an esophageal perforation is not recognized intraoperatively, a leak will manifest in the postoperative period with chest pain, fever, and dyspnea. When a leak is suspected, a swallow evaluation using water-soluble contrast medium can properly identify the site (barium contrast can induce mediastinitis when a perforation is present). With this information the treatment algorithm is straightforward. Briefly, conservative management (nil per os, broad antibiotic coverage, and fluid resuscitation with possible endoscopic stenting) is reserved for early (<24–36 hours) perforations, whereas an esophagectomy is reserved for late (>36 hours) perforations. In these cases, an esophagectomy, rather than a primary repair, has the advantage of surgically removing the entire diseased esophagus.
Recent less invasive approaches to esophageal perforation include endoscopic luminal stenting with minimal invasive repair of the perforation. A study published by Ben-David et al. demonstrates that esophageal stentings with conservative therapy for early, delayed, and late perforations are an effective treatment. 20
Failure of a Heller myotomy manifests postoperatively with persistent or recurrent dysphagia. Persistent dysphagia portrays the immediate existence of technical problems with either the myotomy or the fundoplication. In fact, a short myotomy, usually associated with an inadequate extension onto the gastric wall, is associated with persistent dysphagia. Similarly, an inadequately configured partial fundoplication or the performance of a total fundoplication can trigger persistent dysphagia by extrinsic tightening of the distal esophagus. Usually, persistent dysphagia can be safely corrected with pneumatic dilatation.
Recurrent dysphagia can also occur after a period when the patient is free of symptoms. Although bridging of the edges of the myotomy has been reported as a potential cause, all efforts should be directed at identifying esophageal cancer as a cause of recurrent dysphagia. Once an upper endoscopy and histologic examination of the esophageal mucosa rule out this possibility, pneumatic dilatation can usually correct the dysphagia. In some cases, reoperation in which a second myotomy is performed contralateral to the original one has been shown to provide good outcomes. POEM has also been used for the treatment of recurrent dysphagia after Heller myotomy. Onimaru et al. described excellent results in 10 patients, suggesting that this procedure can obviate the need for a redo operation. 21
Esophagectomy is reserved for those who failed pneumatic dilatation, POEM, or previous surgical corrections in whom definitive treatment is sought.
Megaesophagus, or an esophagus >6 cm in diameter, is thought by some to require esophagectomy. However, others have shown that LHM with Dor fundoplication provides excellent or good results in 70%–100% of patients, even in those with a sigmoid-shaped esophagus.3,22,23 Despite advances in surgical technique, esophagectomy is performed on 5% of patients. Indications include massive dilation despite previous myotomy, persistence of dysphagia despite previous surgical correction, peptic strictures not amenable to dilation, and esophageal cancer. 24
Conclusions
While there is still much to learn in the pathophysiology of achalasia, current treatments can afford patients significant improvement in dysphagia. The overall technique of LHM has changed over the years to include not only muscle fibers of the esophagus, but also those on the stomach that contribute to LES tone. In addition, the type of wrap (partial anterior, partial posterior, and total) has been extensively studied with no general agreement on the best type of partial fundoplication in preventing reflux. 25 We therefore advocate an anterior Dor fundoplication as it not only helps relieve reflux symptoms, but also provides a patch over a potential esophageal perforation, especially in difficult cases. In addition, LHM with Dor fundoplication provides durable long-term results as compared to PD or medical treatments for achalasia. For patients who experience recurrent dysphagia after LHM, PD should be tried first. If a patient fails PD, either a redo myotomy or POEM should be considered in the management before resorting to an esophagectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.