
Abstract
Abstract
Purpose:
To date there exists no published study examining the safety and efficacy of the EndoWrist 45 (Intuitive Surgical, Inc.) robotic stapler. We compared outcomes between the robotic and comparable laparoscopic stapler in robotic-assisted colorectal procedures.
Materials and Methods:
We conducted a retrospective review of 93 patients who underwent robotic-assisted colorectal surgery at our institution from 2012 to 2014. Surgeries included left, sigmoid, subtotal and total colectomies, and low anterior rectal resections. Indications were malignancy and diverticular and inflammatory bowel disease. Preoperative demographics, intraoperative data, and postoperative outcomes were examined. Student's t-test and Fischer's exact used were appropriate.
Results:
Forty-five millimeters laparoscopic staplers were used in 58 cases, while the 45 mm robotic stapler was used in 35 cases. There was no difference in age (P = .651), gender (P = .832), or body mass index (P = .204) between groups. There was no difference in estimated blood loss (P = .524), operative time (P = .769), length of stay (P = .895), or complication rate (P = .778). The robotic stapler group had one anastomotic leak, while the laparoscopic stapler group had six (P = .705). There were more laparoscopic stapler fires (2.69) per patient than robotic stapler fires (1.86) (P = .001). The cost per patient for the laparoscopic group was $631.45 versus $473.28 for the robotic group (P = .001).
Conclusion:
This is the first study to evaluate the robotic stapler. Advantages of the robotic stapler include large range of motion and 90° of articulation, which may provide a benefit when using the stapler in difficult areas like the pelvis. The robotic stapler has a comparable level of safety as a 45 mm laparoscopic stapler and is more cost effective.
Introduction
C
Robotic surgery has been widely used for over a decade. While it has been garnering popularity for gynecologic, thoracic, and colorectal procedures, the disadvantages have been frequently cited. These include increased cost and increased operating time.5–7 However, several studies have shown that in institutions with high volume providers, outcomes between robotic and laparoscopic colectomies are comparable. At these high volume centers, logistical concerns can be mitigated by standardizing docking procedures, appropriating robotics to large rooms, and providing continuity of a robotic-trained staff.7,8
Alternatively, robotic techniques have demonstrated distinct advantages, including increased degree of instrument articulation, three-dimensional visualization, and the ability to control as many as three instruments at once.4,9,10 These technological improvements may be responsible for recent data, which indicate that outcomes such as distal margin length, lymph node procurement, and estimated blood loss are at least equivalent and may be superior in robotic rectal cancer resection versus other modalities. 6
For the confined space of the bony pelvis, robotic-based instruments such as the robotic stapler may provide distinct advantages for maneuverability compared to standard laparoscopic stapling devices. This may lead to decreased stapler firings and improved costs.11,12
To date, there have neither been studies comparing the relative efficacy of robotic staplers with its laparoscopic counterparts nor has there been any data addressing the implications of cost with usage of either device. Moreover, the recall and subsequent reinstatement of the EndoWrist 45 stapler (Intuitive Surgical, Inc.) raise concerns of its safety. In this study, we retrospectively compared outcomes between the robotic versus laparoscopic staplers in patients who underwent robotic-assisted colon and rectal procedures for benign and malignant pathologies. In doing so, we were able to not only provide evidence-based data regarding the robotic staplers' cost effectiveness but also survey our own data to establish its safety.
Materials and Methods
Study design
We conducted a single-center retrospective review of all patients who underwent a robotic-assisted colon and rectal surgery from 2012 to 2014. All operations were performed by a single surgeon. To ensure that our study was adequately powered, any patient who had a left colectomy, sigmoid colectomy, subtotal colectomy, total colectomy or low anterior resection for malignancy, diverticular disease, or inflammatory bowel disease was included for analysis. Patients on whom either a laparoscopic or robotic stapler was not used and patients who underwent robotic-assisted surgery for transverse or right colon pathology were excluded. In total, 93 patients met our inclusion criteria. Data on preoperative patient demographics, intraoperative variables, and postoperative outcomes were collected. Financial data were obtained from the business and financial department for surgical services at our institution and representative of purchasing costs, but not necessarily reflective of costs seen or incurred by patients.
Statistical analyses
Variable distributions were examined for skewness and outliers and log-transformed if necessary. Univariate comparisons between procedures were done with the chi-square or Fisher's exact test for categorical or ordinal variables and with the unpaired two-tailed t-test for continuous variables. Multivariate models were examined for the outcome variables: cost, number of staples, leak, and overall complications. The predictors included procedure (laparoscopic versus robot), as well as age, gender, prior abdominal surgery, body mass index (BMI), diabetes mellitus (DM), and hypertension (HTN). Logistic regression was used to predict leak and overall complications (binary outcomes). A general linear model was used to predict cost. A Poisson regression model was used to predict number of staples (a count outcome variable), with correction for overdispersion. As a sensitivity analysis, we also used a general linear model for the staples outcome variable, since this could also be considered a continuous variable. All analyses were done using SAS version 9.3 (Cary, NC), with P < .05 considered significant.
Results
Patient data are included in Table 1. In total, 93 patients who underwent robotic-assisted surgery were included in the study. Of these cases, 58 utilized the 45 mm laparoscopic stapler, while 35 used the 45 mm robotic stapler. Between groups, there was no statistically significant difference in age (P = .651), gender (P = .768), prevalence of comorbidities, BMI (0.204), preoperative steroid use (P = 1.000), preoperative chemoradiation (P = 1.000), or incidence of prior abdominal surgery (P = .201). There was no significant difference in estimated blood loss (P = .524), operative time (P = .769), length of hospital stay (P = .895), or overall complication rate (P = .778). While the laparoscopic stapler group had six anastomotic leaks and the robotic stapler group had one, this difference was also not significant (P = .705). There were, however, significantly more laparoscopic stapler fires (2.69) required per patient than robotic stapler fires (1.86) (P = .001). The stapler cost per patient for the laparoscopic stapler group was $631.45 versus $473.28 for the robotic stapler group (P = .001).
COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; DVT/PE, deep venous thrombus/pulmonary embolus; HTN, hypertension.
On multivariate analysis, there were no statistical differences in the amount of anastomotic leaks or overall complications between groups; however, the laparoscopic stapler remained more expensive and required overall more staple fires compared to the robotic stapler (P = .0003 and .045, respectively)
Discussion
This study is the first of its kind to compare the cost effectiveness and efficacy of the robotic stapler with comparable laparoscopic devices. While the laparoscopic stapler can be articulated, its maneuverability is limited by both the diminished degrees of freedom within the joint of the stapler and the fulcrum effect of the shaft of the stapler through the trocar in the abdominal wall. The robotic stapler provides 90° of articulation, which may lead to more accurate and precise firings along the same trajectory of the initial staple line and diminishes the distance traversed across the bowel. With the recall of the EndoWrist 45 (Intuitive Surgical, Inc.) and its subsequent reinstatement, our study also addresses the concern for its safety in patient populations undergoing colon and rectal resection. As the use of robotic-assisted surgery becomes more widespread, these evaluations are critical.
It has been well documented that the risk for anastomotic leak increases with the number of stapler fires needed for resection11,13 and that the sequelae of these leaks can lead to significant morbidity. 12 Fewer stapler fires were required to transect bowel in the robotic group than the laparoscopic group (Table 1). One of our concerns was that the learning curve associated with new technologies or techniques may have skewed our data. We do not believe this is the case as staple fires over time for both groups (Fig. 1) did not diminish. In addition, bias between surgeons of varying experience level was not a factor as this was a single surgeon study.
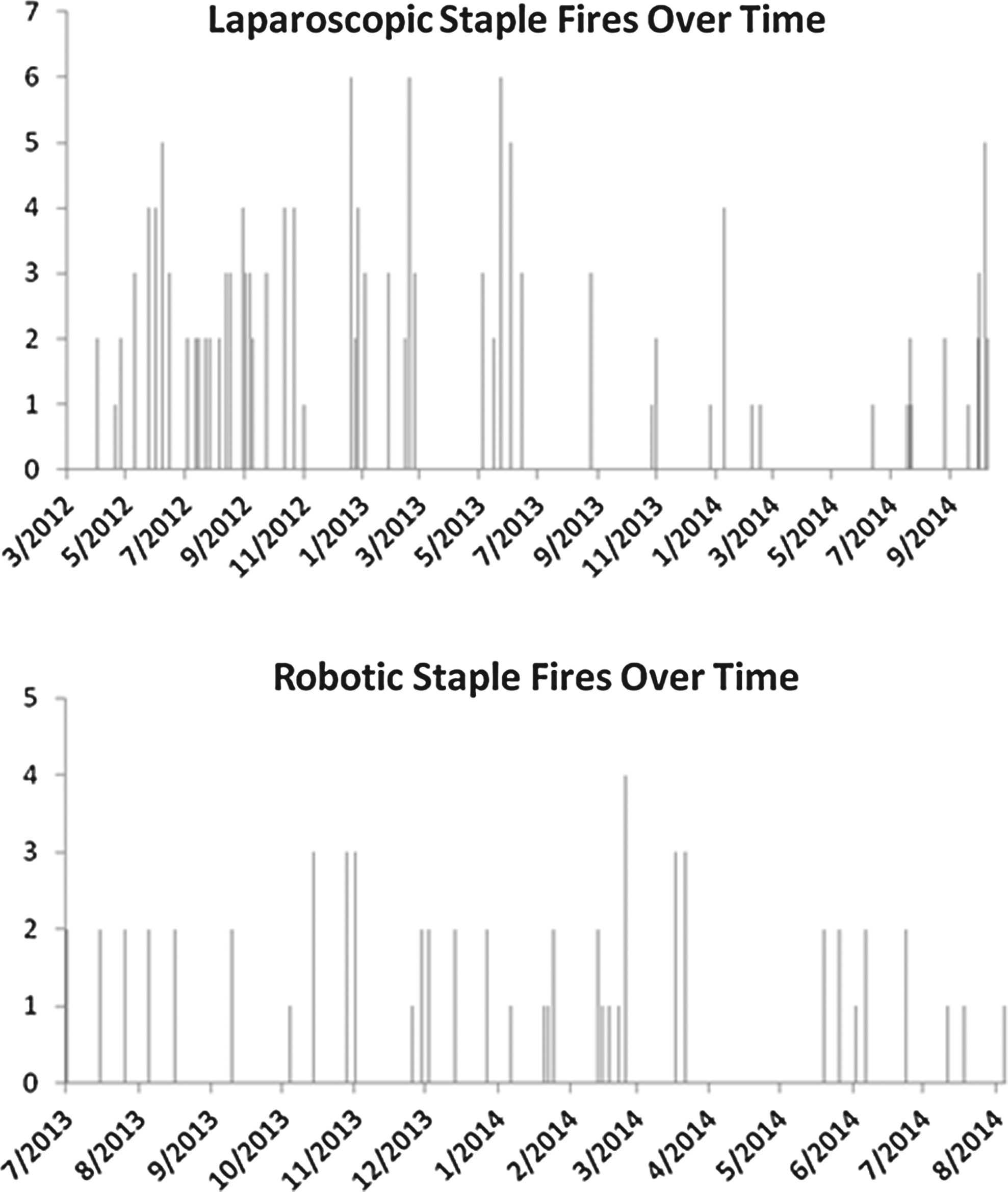
Stapler fires as a function of time between laparoscopic and robotic groups.
Although not statistically significant, our data show a trend toward decreased anastomotic leaks for the robotic stapler group compared to the laparoscopic stapler group (Table 1). In all operative cases, the EEA stapler was used in the formation of our anastomoses and there were no misfirings. The robotic group did have a high rate of reoperations within 30 days with three reoperations in the robotic group and none in the laparoscopic group (P = .05); however, none was related to anastomotic leaks. Two were for revision of an obstructed diverting loop ileostomy. One was for postoperative bleeding from a marginal artery.
Our data further indicate that fewer stapler firings translate to lower intraoperative costs and the possibility of fewer anastomotic leaks. For the patient, this equates to improved outcomes regarding quality of life and avoidance of significant and debilitating morbidities. 12
From an oncologic perspective, obtaining an adequate distal margin has always been a concern for rectal cancer resection and it has been well established that the robotic approach does not negatively affect staging. 14 In this study, there is no significant difference in the mean distal margin length between the robotic stapler (2.29 cm) and laparoscopic stapler (3.38 cm) groups (P = .175; 95% CI −3.911 to 0.74). Similarly, there was not a significant difference between the groups for lymph node procurement with 17.81 versus 17.44 for laparoscopic and robotic, respectively (P = .0918, 95% CI −7.529 to 6.790) (Table 2).
Patients without residual cancer after chemoradiation therapy had no distal margins to assess, hence discrepancy between total cancer patients and those with margins.
Total lymph nodes noted in final pathology reports were recorded here, regardless of indication for surgery or final pathology.
IBD, inflammatory bowel disease.
There was a trend toward greater distal margins with the laparoscopic staplers compared to the robotic stapler for all pathologies. Our concern was that this was due to the relative difference in type of operation performed between groups (Table 3). We therefore compared rectal cancer cases in both groups to assess both the distal margins and lymph nodes procured. There was no statistically significant difference between the robotic stapler (1.19 cm) and the laparoscopic stapler (2.86 cm) groups (P = .733, 95% CI −3.204 to 0.126). Again, there was no statistically significant difference in lymph node procurement between the robotic (19.4) and laparoscopic (24.1) stapler groups (P = .301, 95% CI −13.645 to 4.485).
This study is retrospective in its design and brings with it all of its inherent limitations. In addition, our data set represents the work of a single surgeon at a single institution; thus, our experience may not be generalizable to the inexperienced robotic surgeon. However, we believe our sample set represents the caseload of a typical colorectal surgeon that practices robotic-assisted surgery, and our data recapitulate the situations in which the robotic stapler would be used.
In conclusion, our study is the first of its kind to compare the robotic stapler with comparable laparoscopic stapling devices. Advantages of the robotic stapler include a large range of motion and 90° of articulation, which may provide a benefit when using the stapler in confined spaces such as the pelvis. Our data indicate that the robotic stapler has a comparable level of safety and efficacy as a 45 mm laparoscopic stapler, can obtain comparable resection margins and lymph node yield as the laparoscopic stapler, and is a viable cost-effective option.
Footnotes
Disclosure Statement
Dr. Vincent Obias is a consultant for Intuitive Surgical, Inc., but did not receive any monetary compensation for this study; this study was not funded or supported by Intuitive Surgical, Inc. Ms. Aziz and Drs. Holzmacher, Luka, Amdur, and Agarwal have no disclosures.