
Abstract
Abstract
Purpose:
To understand the role of case complexity in the learning curve for robotic colorectal surgery.
Materials and Methods:
Sixty-two patients who underwent robot-assisted colorectal surgery were retrospectively reviewed. Each case was assigned a category of complexity ranging from I to IV. Overall, groups and categories of segmental colectomy, rectopexy, and proctectomy for cancer were analyzed according to case volume. Forty-eight patients who underwent similar laparoscopic cases during the same period were also reviewed for comparison.
Results:
Level I complexity cases were identified in 30% of the first 15 cases compared to 3% after the first 15 cases (P < .01). Level IV complexity cases were identified in 10% of the first 15 cases and 34% after 15 cases (P = .03). Mean operative time for the overall group was 426 minutes (range 178–766, standard deviation [SD] = 152) in the first 15 cases and 373 minutes (range 190–593, SD = 109) after more than 15 cases (P = NS). Mean operative time for rectal cancer procedures decreased from 518 minutes (range 425–752, SD = 88) to 410 minutes (range 220–593, SD = 98) after 15 cases (P = .02). Mean operative time for rectopexy decreased from 361 minutes (range 276–520, SD = 85) to 258 minutes (range 215–318, SD = 34) after 15 cases (P = .03). Overall complications were reduced after 15 cases (6.3%) compared with the first 15 cases (27%) (P = .04). When comparing laparoscopic and open cases, laparoscopic cases were associated with a significant shorter operative time (P = < .00001) as well as overall cost (P = < .00001).
Conclusion:
Complex robotic colorectal surgery can be performed early in the experience, with reduced operative time. Overall complications are reduced after 15 robotic cases. This study shows that improvement in robotic surgery operating time and surgical outcomes occur along with application of the technology to more difficult cases, not as a function of choosing less complex cases.
Introduction
M
The robot-assisted approach may offer advantages over laparoscopic colorectal surgery in patients with difficult anatomy such as those with obesity or a narrow pelvis, particularly during rectal dissection and total mesorectal excision (TME). 7 Oncologic outcomes for robotic rectal cancer surgery have been reported to be acceptable with low positive margin rates (5.7%) and a good 3-year survival rate (93%) in a retrospective case series of 370 Stage I–IV rectal cancer patients. 8 Robotic rectal cancer dissection may better preserve normal voiding and sexual function compared to laparoscopic TME. 9 Robotic surgery may also facilitate a lower conversion rate to open compared to laparoscopic procedures. 10
Most reports describe the robotic colorectal surgery learning curve to plateau after 15–25 cases.2,11 More complicated dissections such as TME may have a bimodal plateau after 33 cases, and again at 72–80 cases.12,13 Higher volume providers and hospitals perform robotic colorectal surgery with fewer complications and reduced cost. 14 An unaddressed point is how much of the improved operative times and outcomes reflects technical improvement compared to selection of less complex cases.
Miskovic et al. proposed recommendations for selecting cases early in the learning curve of laparoscopic colorectal surgery based on expert consensus and a systematic review of the learning curve literature. 15 Parameters of body mass index (BMI), colon versus rectal resection, and diagnosis are predictive of complications and conversions, and are used to classify cases into objective levels of complexity I–IV (Table 1). An experience of 150 laparoscopic colorectal cases has been recommended before performing the most challenging (Level IV) operations. 15
Described from Miskovic et al. 15
BMI, body mass index.
The aim of this study was to grade robotic colorectal surgeries with a complexity scoring system to demonstrate the evolution of case complexity in the robotic experience. We hypothesized that after 15 cases, the robotic surgeries would have decreased operative time with increased case complexity.
Materials and Methods
A retrospective chart review was performed from a robotic surgery database approved by the local Institutional Review Board. All patients were operated on by 2 surgeons performing robotic colorectal surgery during the study period of 2012–2014. These surgeons were experienced laparoscopic surgeons before beginning the robotic experience. Sixty-two patients were identified from the database. Subgroup analysis was performed for segmental colectomy, rectopexy, and rectal resection surgeries.
We reviewed age, gender, BMI, estimated blood loss (EBL), LOS, readmission, complications, conversion to open surgery, lymph node harvest, margins, pathology, and total operative time for the patients. Operative time was from start time of incision to closure of the skin. Similar data were obtained for patients having undergone similar laparoscopic surgeries by the same surgeons during the study period.
Overall case complexity was graded by a previously defined system used in laparoscopic colorectal surgery based on factors such as type of disease process, BMI, and male or female pelvis (Table 1) 15 . This scoring system was established using multilevel regression models on original data sets to determine which factors increase conversion and complication rates. The disease processes that elevate operative complexity were determined from qualitative group consensus. Each case was assigned a complexity score ranging from least complex (Level I) to most complex (Level IV). Outcomes were compared between groups of patients undergoing robotic colorectal surgery within the initial 15 robotic cases of the surgeon and those operated upon after the first 15 cases in the experience (Table 2). The specific cases performed were recorded (Table 3).
≤15 includes all cases performed with <15 prior robot cases performed. M, male; F, female.
APR, abdominoperineal resection; BMI, body mass index; EBL, estimated blood loss; LAR, low anterior resection; LOS, length of stay.
APR, abdominoperineal resection; LAR, low anterior resection.
Cost analysis for the first 15 cases compared with the second 15 cases was performed. Cost of LOS and operating room (OR) were placed at $991/24 hour period and $5000/24 hour period, respectively. Cost of anesthesia was calculated as equaling $228 + (OR time/15) × 20.81. Additional cost for instrumentation was estimated at $2000/robot case. Values were extracted from cost assessment at a local hospital. Cost of robotic cases was also compared to laparoscopic cases, this formula included the costs above as well as the costs of readmission, and treatment of complications, including reoperation.
Statistical analysis
Clinical variables among the study groups were compared using t-tests for parametric data and χ2 tests for nonparametric data. Linear and logistic regressions were performed to identify variables of significance. Factors with both nominal and ranked variables were analyzed by the Kruskal–Wallis test. Moving averages for operative times were calculated and graphed for rectopexy and the rectal cancer groups. A P value <.05 was considered statistically significant. Statistical analysis was performed by Microsoft® Excel software and Epi Info™ 3.5.3 (Atlanta, GA).
Results
Overall robotic experience
Mean age of patients was 64.4 years in the first 15 cases and 62.8 years after 15 cases (P = NS). Fewer women (47%) were identified in the first 15 cases compared with 62% after more than 15 cases (P = .047). In the overall sample, Level I, II, III, and IV cases composed 16%, 44%, 18%, and 23%, respectively. There were 30% Level I cases performed in the first 15 and 3% Level I cases after 15 cases (P = .04). Level II and Level III cases were performed in 33% and 27% for the first 15 cases and 53% and 9% after 15 cases (P = NS). There were 10% Level IV cases performed in the first 15 cases and 34% Level IV cases performed after 15 cases (P = .01). Average operative time was 426.6 minutes (range 178–766, standard deviation [SD] = 151.9) for the first 15 cases and 373 minutes (range 190–593, SD = 109.2) after 15 cases (P = NS).
Overall complications were 27% for the first 15 cases and 6.3% after more than 15 cases (P = .03). Specific postoperative surgical complications were not different between the groups (Table 4). Conversion to open occurred in 13.3% of patients in the first 15 cases and 6.3% after 15 cases (P = NS). Readmission was 10% for the group operated upon within the first 15 cases and 6.3% after more than 15 cases (P = NS) (Table 2). There were no identified deaths or cancer recurrences in this cohort with average follow-up of 15.4 months. Among independent factors, including age, BMI, >15 cases, gender, and diagnosis, multivariate logistic regression showed that only >15 cases predicted complications (OR 0.9, P = .049).
Right hemicolectomy subgroup
Eleven patients underwent robotic right hemicolectomy for colon cancer in 27% of cases and polyps in 73% of cases. The change in operative time after 15 cases was not significant (261.3 minutes versus 312 minutes, P = NS) in this group. Lymph node count was also unchanged in the first 15 cases (14) compared to the remainder (16.7) (P = .35). All right hemicolectomy margins were >2 cm in every dimension.
Complications were 14% within the first 15 cases and 0% after 15 cases (P = 1). Conversions were 29% in the first 15 cases and 0% after 15 cases (P = 1). LOS was 4.5 days for the first 15 cases and 7 days after 15 cases (P < .01). The case complexity for right hemicolectomies had a median of Level I in the first 15 and a median of Level IV after 15 cases (P = NS). Univariate linear regression for operative time in the right hemicolectomy subgroup shows BMI (b coefficient = 7.97, P = .01) and Level IV cases (b coefficient = 128.1, P = .035) to predict operative time.
Rectopexy subgroup
Fourteen patients underwent robotic rectopexy. Operative time for rectopexy was 361 minutes (range 276–520, SD = 85.3) in the first 15 cases, and 258 minutes (range 215–318, SD = 33.6) after 15 cases (P = .03) (Fig. 1). LOS was 6.3 days for the first 15 cases, and 3.9 days after 15 cases (P = NS). Univariate linear regression of operative time in rectopexy showed only >15 prior cases to be predictive of operative time (b coefficient = −107.1, P = .03). Multivariate analysis showed that only >15 prior cases predicted operative time (b coefficient = −133.1, P = .04). Average cost for rectopexies performed in the first 15 cases was $14049.20, and $12003.50 for those performed after 15 cases (P = NS).
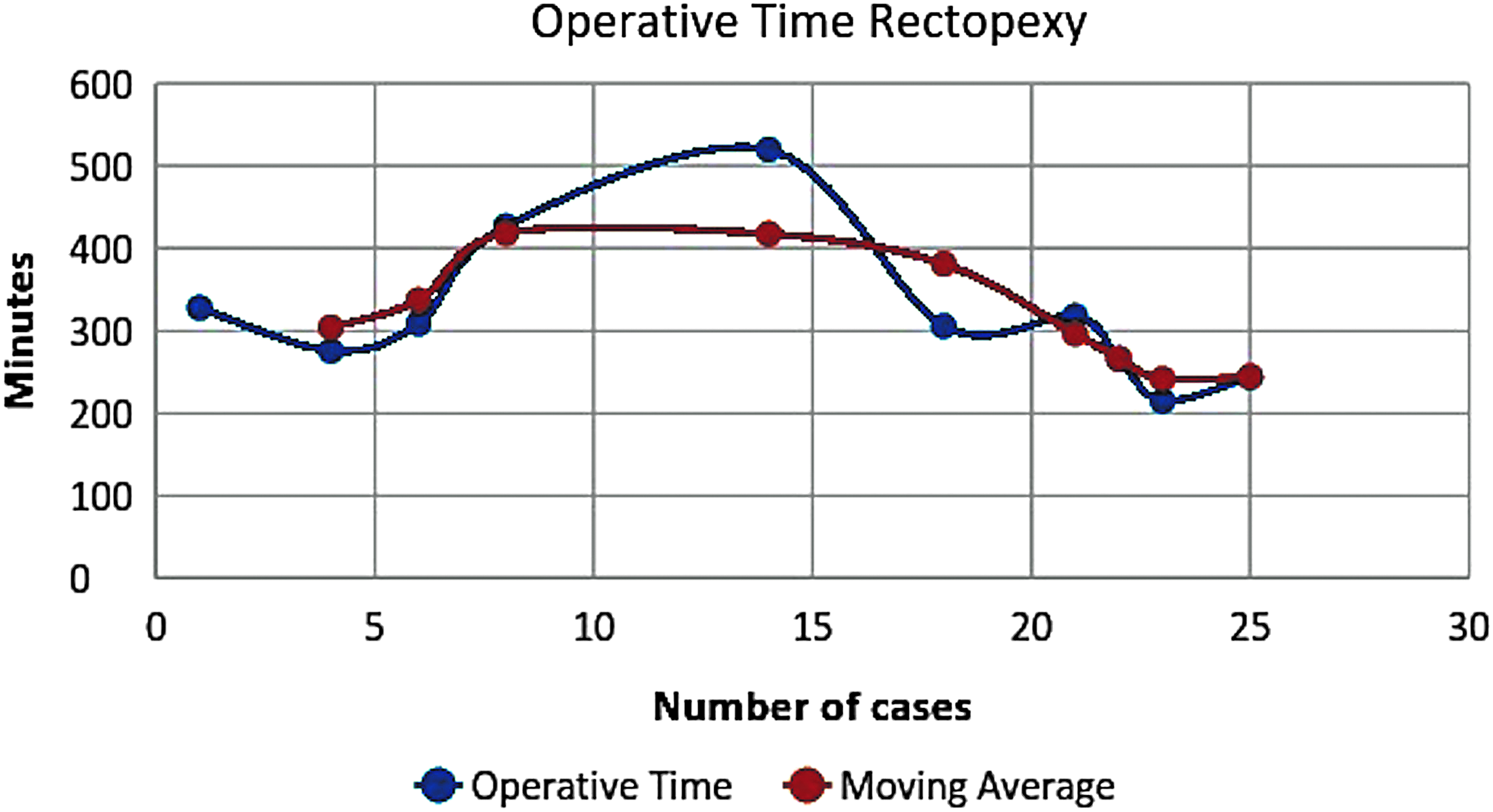
Relationship between number of robotic cases and operative time in minutes for robotic rectopexy with moving average trend line.
Rectal cancer subgroup
Twenty-four patients underwent robotic proctectomy for rectal cancer. Ninety-two percent of these underwent neoadjuvant chemoradiation for locally advanced disease before surgery. Four percent avoided neoadjuvant chemoradiation for T1 disease and 4% had a history of distant radiation. Operative time for rectal cancer dissections was 518 minutes (range 425–752, SD = 87.6) in the first 15 cases and 395 minutes (range 220–593, SD = 97.7) after 15 cases (P = .02) (Fig. 2). There was more frequent coloanal anastomosis after 15 cases (36%) compared with the first 15 cases (0%) (P = .046).
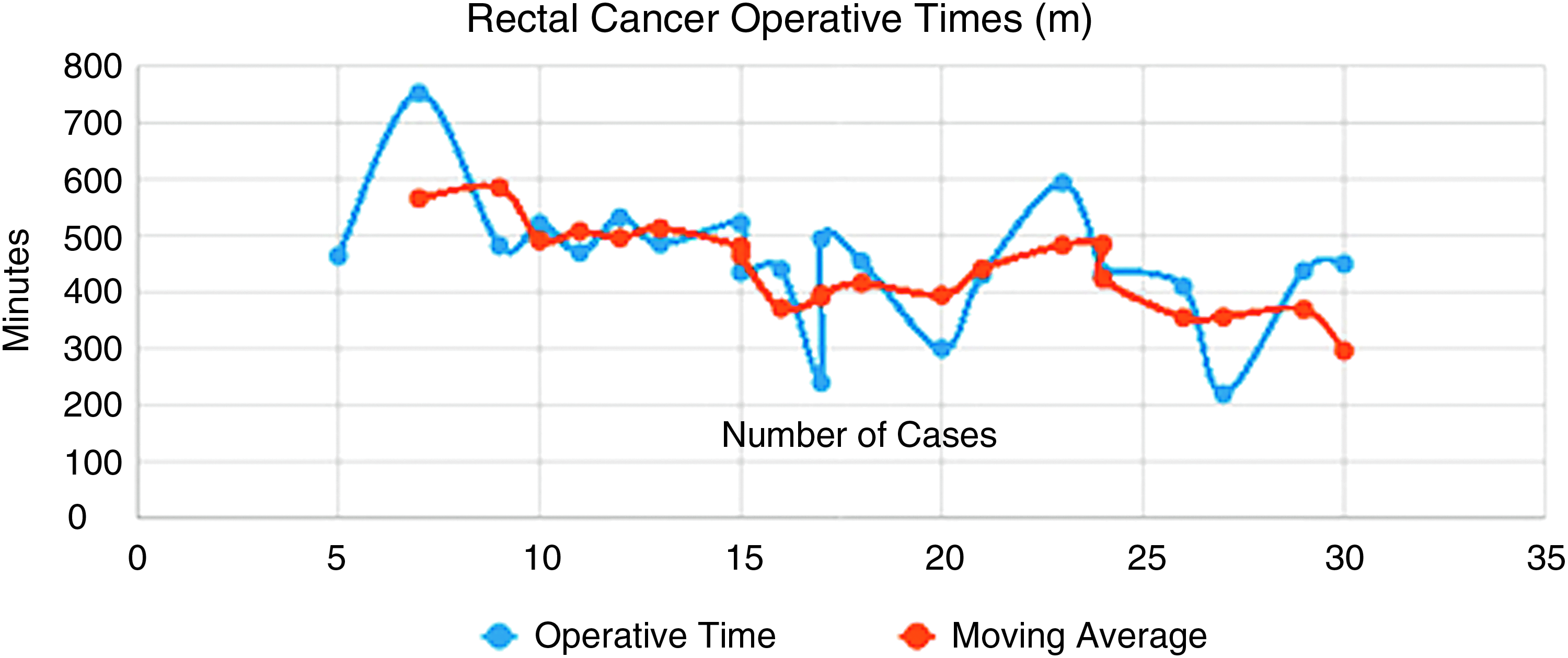
Relationship between number of robotic cases and operative time in minutes for robotic rectal cancer resection with moving average trend line.
LOS was 9.1 days in the first 15 cases and 7.9 days after 15 cases (P = NS). Lymph node harvest was 11.1 in the first 15 cases and 11.8 after 15 cases (P = NS). Margin positivity within 1 mm for rectal cancer cases was 9% (1 case of close radial margin) for the first 15 cases and 0% for after 15 cases (P = NS). Univariate linear regression for operative time in rectal cancer resection showed that BMI (b coefficient = 10.22, P = .02), number of prior robotic cases (b coefficient = −178.9, P = .03), male pelvis (b coefficient = 90.47, P = .03), and Level IV cases (b coefficient = 108.4, P = .008) predicted increased operative time.
Multivariate linear regression for rectal cancer including age, BMI, case number, gender, pathology of T3 or greater, and chronic inflammation (level excluded given covariance with independent factors) showed that only BMI (b coefficient = 12.4, P < .01) and case number (b coefficient = −10.27, P < .01) predicted operative time. Average cost for rectal cancer dissections performed in the first 15 cases was $16550.27 and $15,337.21 for those performed after 15 cases (P = NS).
Robotic versus laparoscopic groups
Sixty-two robotic surgical cases were compared to 48 laparoscopic surgical cases. There were no significant differences in demographic variables of gender, age, or BMI. There were also no differences in LOS, complication rate, complication severity, blood loss, or cancer staging. Robotic surgery had a mean operative cost of $6920.58 (SD = 725.51) and a mean total cost of $17,293.32 (SD = 9787.39). Laparoscopic surgery had a mean operative cost of $3545.71 (SD = 1434.15) and a mean total cost of $11,581.88 (SD = 7975.25). Robotic surgery cost was significantly more than laparoscopic surgery, in terms of both operative cost and total cost (P = < .0001).
Discussion
Robotic colorectal surgery is an evolving frontier of treatment. This technology may be especially helpful for rectal dissections where there may be technical issues with the laparoscopic approach. 16 The addition of case complexity assessment to robotic learning curve studies may allow a more comprehensive analysis of the outcomes and surgeon progression. The present study expands on this complexity aspect of robotic colorectal proficiency.
The complexity of colorectal surgery is derived from surgeon and team factors, patient factors, and disease factors. A key study in assessing the complexity of laparoscopic surgery has accounted for these factors and provided the complexity scale used in this study. 15 Previous studies have suggested that short-term outcomes for robotic colorectal surgery may be shorter than laparoscopy and may improve after just 15 cases.14,17 However, case complexity was not reported in these studies, thereby introducing a possible element of bias based on favorable case selection.
This study shows that outcomes and complication rates improve after 15 cases, despite increased case complexity. Concern for the effect of case selection bias on learning curve was also alleviated by demonstrating a reduction in low complexity and an increase in the highest complexity operations performed after the first 15 cases. Operative time improved after 15 cases in the overall group, as well as for rectopexies and rectal cancer resection subgroups. Although LOS increased in the right hemicolectomy group after 15 cases, 66% of these patients had morbid obesity and were in the Level IV category.
Level IV cases also predicted increased operative time for the right hemicolectomy group. For rectopexy, only >15 previous cases predicted operative time. The level of case complexity did not impact operative time for rectopexy as case complexity was similar within this subgroup. Average cost for surgery did not decrease after 15 robotic cases, however, this may, in part, be explained by increasing complexity of surgery.
The spectrum of the cases shows a shift from segmental colectomies to more rectal surgery after the first 15 cases. There were more abdominoperineal resections in the first 15 cases. This may be explained by a greater ability to perform sphincter sparing surgery for low rectal cancers with greater experience. After 15 cases, coloanal anastomoses were performed more frequently in 36% of rectal cancer cases compared to 0% in the first 15. Robotic surgery may be a safe and effective alternative to open surgery for TME and coloanal anastomosis in low rectal cancer. 18
This study does have several limitations. One limitation of the data is the retrospective nature. Another limiting factor for the study was the inability to separate operative time spent on the console from other portions of the procedure. This facet of the learning curve has shown the greatest change with increased experience in other studies. 19 The console model and associated evolving tools such as more maneuverable robotic staplers may facilitate aspects of colorectal surgery such as TME and stapling at the level of the pelvic floor in patients with the most difficult anatomy, 20 and the advancement of the technology during the course of the study period was not evaluated. In addition, these results represent the experience of 2 surgeons with extensive prior laparoscopic colorectal experience.
Extrapolation of these results to surgeons with mostly open colorectal surgical experience and minimal laparoscopic skills may not be appropriate, although studies have shown good results with the transition to the robotic technology. 19 Similarly, future studies may be more helpful in comparing the difference in overall cost between laparoscopic and robotic surgery throughout the learning curve. An additional limitation is the small numbers in this retrospective series, as it is possible that another plateau in reduced operative time occurs at a higher volume. It should also be noted that the study had more women than men after 15 cases, however, male and female pelvis did not predict a difference in outcomes. This may be evidence for use of robotics in technically difficult rectal dissections with the laparoscopic approach such as the narrow male pelvis.
Ultimately, the role, if any, for robotics has yet to be determined. The goal should be for improved outcomes using robotic surgery with similar costs to laparoscopic surgery. This study shows an attenuated robotic learning curve compared to traditional data for early learning in laparoscopic colorectal surgery. However, further data are needed to determine if there is benefit at much higher volumes that could make the cost of robotic surgery worthwhile.
Conclusion
These results support using objective criteria to select easier cases for the first 15 cases in the robotic colorectal surgery learning curve. Complex robotic colorectal surgery can be performed safely by expert laparoscopic surgeons early in their experience, although overall complications are reduced after 15 cumulative robotic cases. This study shows that improvement in colorectal robotic operative time and surgical outcomes can occur while case complexity increases. Robotic surgery may accelerate the learning curve even in the face of more complex cases when compared to laparoscopic surgery. Future studies comparing laparoscopic and robotic methods should evaluate case complexity so that outcomes can be better evaluated.
Footnotes
Disclosure Statement
No competing financial interests exist.