
Abstract
Abstract
Background:
Mirizzi syndrome (MS) is a rare complication of cholecystolithiasis that causes compacted gallstones and is often accompanied by severe inflammation of Calot's triangle. This study compared the use of laparoscopic surgery for MS without dissection of Calot's triangle with routine laparoscopic cholecystectomy (LC).
Methods:
A total of 411 consecutive patients underwent laparoscopic surgery for benign gallbladder (GB) disease between January 2013 and December 2014. Five patients underwent laparoscopic surgery for MS (MS group) while 406 underwent routine LC (LC group). The preoperative diagnosis was accurate in all patients in the MS group.
Results:
The LC and MS groups did not differ significantly in the operation time, blood loss, length of hospital stay, or incidence of GB carcinoma. In addition, conversion, bile duct injury, and bile leak rate were not different between the two groups.
Conclusions:
This study demonstrates the safety of laparoscopic partial cholecystectomy without dissection of Calot's triangle for MS. In addition, an accurate preoperative diagnosis is critical in surgical decision making to avoid injury to the bile duct.
Introduction
L
MS is a well-known but rare complication of cholecystolithiasis, and has been reported as a risk factor in LC. The incidence rate of MS is reported to be 0.18%–5.7% in cases of cholecystolithiasis.5,6 MS refers to a common hepatic duct (CHD) obstruction caused by an extrinsic compression from an impacted stone in the cystic duct or the infundibulum of the gallbladder (GB). Due to inflammation, the morbidity rate is reported to be 16%–31% and the conversion rate is 41%–67% in laparoscopic surgery for MS.5–9 These rates are extremely high compared to those in routine LC.
Partial or subtotal cholecystectomy has been reported as a procedure that avoids biliary injury in LC for difficult GB surgery.10,11 However, technical reports on the safety of laparoscopic partial cholecystectomy for MS are very limited. Here, we report the success of laparoscopic partial cholecystectomy for MS at our institute.
Materials and Methods
A total of 411 consecutive patients underwent laparoscopic surgery for benign GB disease between January 2013 and December 2014 at the Asahi General Hospital. Patients were divided into two groups: patients undergoing laparoscopic surgery for MS (MS group) and patients undergoing other LC surgeries (LC group). The MS diagnosis was based on clinical, radiological, and intraoperative findings, including inflammation due to gallstone impacted in the cystic duct or in the infundibulum of the GB and CHD disruption, stenosis, or compression caused by impacted stone. The type of MS was classified as type 1 or type 2 according to McSheery's classification. 12 The following parameters were examined: clinical data, preoperative radiography, surgical techniques, operative complications, pathological findings, and hospital stay. This was a retrospective study approved by the Ethical Review Board of the Asahi General Hospital (approval No. 2015051910).
Surgical procedures for MS with no dissection of Calot's triangle
We started the surgery for MS with four ports, which is similar to routine LC at our institution. First, dissection of the adhesion and exposure of the GB were performed. The surgeon checked the orientation around the GB including the duodenum, hepatorenal fossa, and the groove of Rouviere. The dissection of the inferior surface of the GB calls for careful attention as there is a high incidence of cholecysto-colonic or -duodenal fistula in MS. These fistulas can be repaired by laparoscopic suturing or stapling technique.
The resection of the GB was restricted to the bottom and body. The incision of the GB neck wall revealed the gallstone in the lumen of the GB and partial cholecystectomy was performed. The gallstone was confirmed in the lumen of the neck of the GB and was removed with laparoscopic forceps. Cutting the GB wall on the visceral side is helpful in avoiding biliary injury when removing the gallstone. The opening of the cystic duct was identified after removing the gallstone. Interrupted suture is a safe and easy technique for the closure of the opened cystic duct in the presence of inflammation. Practically, the suturing axis was out of order, because the epigastric port is perpendicular to the axis of the GB. An additional port parallel to the axis of the GB reduced the technical difficulty of the suture. Intraoperative cholangiography is indicated if the anatomy of the biliary tree is not clearly identified or there is suspicion of retained stones. Figure 1 shows the whole surgical procedure.
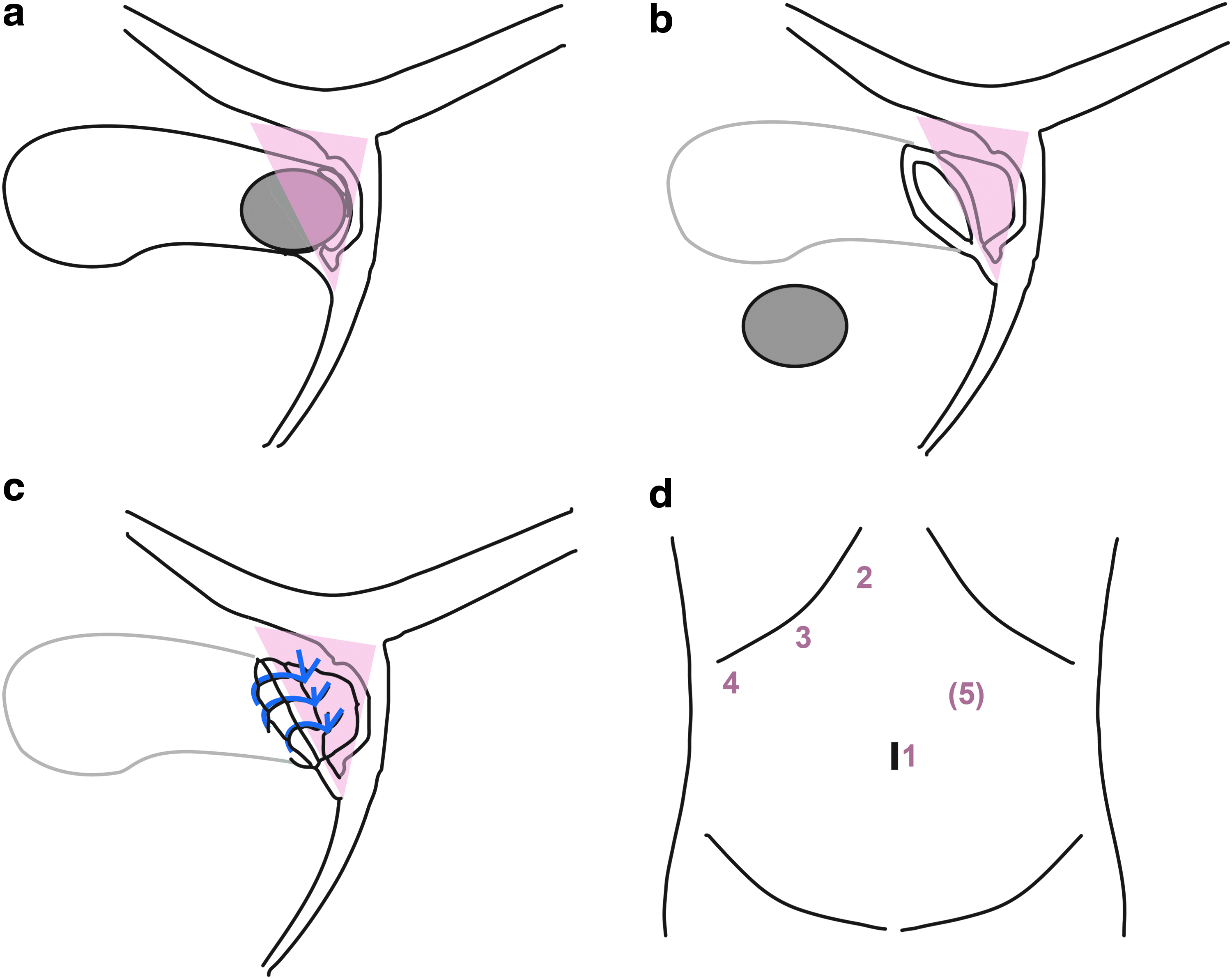
Schema of the surgical procedure.
Statistical analysis
Analyses were carried out using a t-test or Mann–Whitney U test for continuous variables and Fisher's exact test for categorical variables. A P < .05 was defined as significant. Statistical analyses were performed using JMP version 10 (SAS Institute, Cary, NC).
Results
Characteristics of patients
During the study period, 5 patients were diagnosed with MS type 1 and no patients were diagnosed with MS type 2. The preoperative diagnosis was performed correctly in all patients with MS. Thus, a total of 406 patients were in the LC group and 5 were in the MS group. The age and sex of the two groups were not statistically different (Table 1).
LC, laparoscopic cholecystectomy; MS, Mirizzi syndrome.
Surgical outcome
The LC and MS groups did not differ in the operation time, blood loss, or length of hospital stay (Table 1). In the LC group, 3 cases were converted to open surgery and no case was converted in the MS group. In the LC group, bile duct injury occurred in 1 case intraoperatively and a bile leak occurred in 2 cases. These events occurred in conversion patients. They were treated conservatively and all were successful. No patients experienced bile duct injury or bile leak in the MS group. An incidental carcinoma of the GB was observed in 5 patients in the LC group but in none of the patients in the MS group; this difference was not statistically significant (1.2% versus 0%).
MS group
The incidence rate of MS was 1.2% (5/411). The mean age of patients in the MS group was 70 years (range, 63–77 years), and 3 were male and 2 were female. The preoperative clinical symptoms included cholangitis in 4 patients and cholecystitis in 3 patients (Table 2). In addition, 2 patients were comorbid for cholangitis and cholecystitis. Obstructive jaundice was observed in 2 patients. Patients with cholangitis were managed with antibiotics and endoscopic nasobiliary drainage or retrograde biliary drainage. Patients with cholecystitis were managed with antibiotics and percutaneous transhepatic GB drainage preoperatively. Choledocholithiasis was detected in 3 patients and the gallstones were removed by endoscopic retrograde cholangiopancreatography (ERCP) preoperatively. All patients underwent the selective surgery.
CBD, common bile duct; DIC-CT, drip infusion cholangiographic-computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; MRCP, magnetic resonance cholangiopancreatography; PTGBD, percutaneous transhepatic gallbladder drainage.
The radiological findings were defined as 4 CHD grades: disruption, stenosis, compression, and no finding (Fig. 2). Magnetic resonance cholangiopancreatography (MRCP) was performed in all patients. Disruption and stenosis were observed in 3 and 2 patients, respectively. ERCP was performed in 4 patients (3 with compression and 1 with no finding). Drip infusion cholangiographic computed tomography (DIC-CT) was performed in 3 patients (2 with stenosis and 1 with no finding). All patients were diagnosed as MS type 1 preoperatively. In case 2, pneumobilia and cholecysto-colonic fistula were diagnosed with computed tomography.
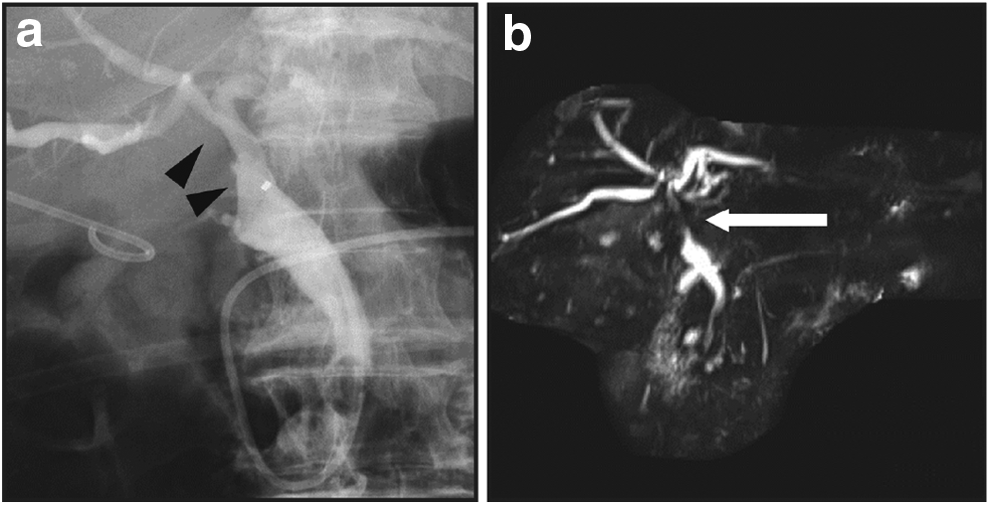
Preoperative radiological findings of case 3.
The operation for the MS group was performed according to the surgical procedures described above (Fig. 3). An additional port was used in 3 cases. The cholecysto-colonic fistula that was diagnosed due to preoperative and intraoperative findings in cases 2 and 3 was repaired by a laparoscopic suturing technique. Intraoperative cholangiography was performed in cases 3 and 5 to clarify the anatomy of the biliary tree. In case 5, antibiotics were continued for preoperative cholangitis until discharge on postoperative day 7 with no other complications. No postoperative morbidity or mortality occurred in the MS group. Postoperative radiological assessment was performed in all MS patients. The stenosis of CHD was improved and the biliary tree was repaired in all patients (Fig. 4). No late complication or recurrence of gallstone was observed during the follow-up period (mean, 24.4; range, 15–32 months).
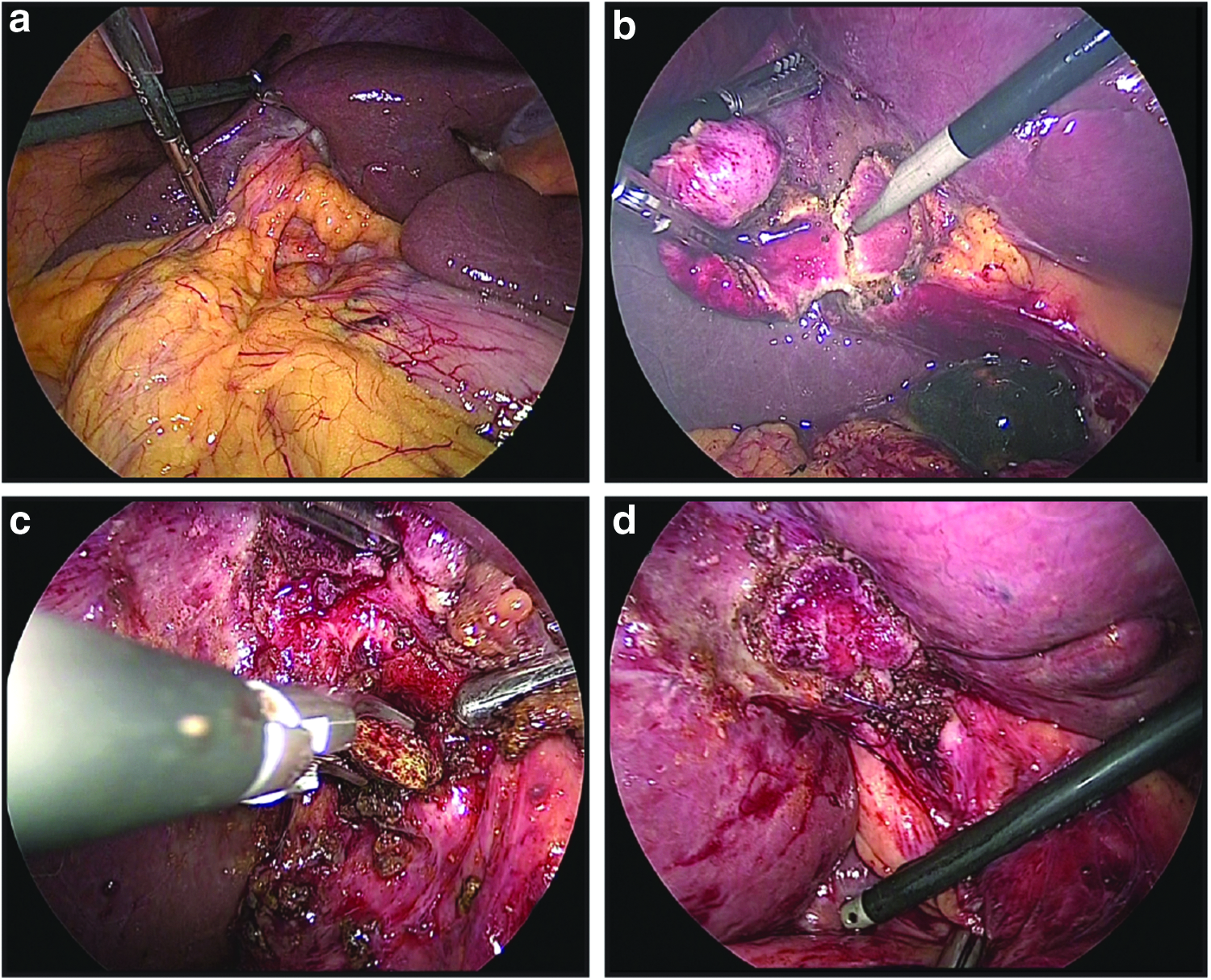
Intraoperative findings of laparoscopic surgery for type 1 Mirizzi syndrome (case 5).
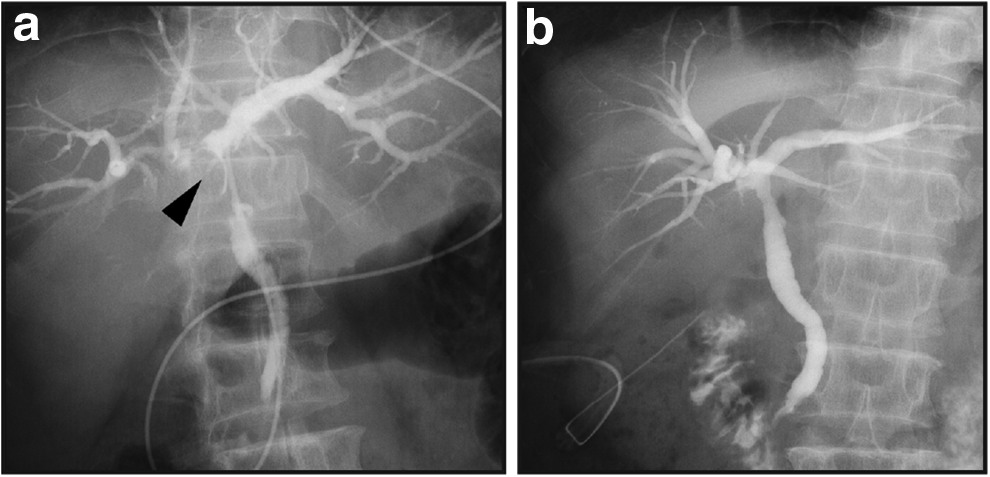
Radiological findings of case 5.
Discussion
McSherry et al. 12 classified MS as type 1 (without cholecysto-choledoco fistula) or type 2 (with cholecysto-choledoco fistula). All of our MS cases were diagnosed preoperatively as MS type 1; no case was observed with cholecysto-choledoco fistula in the various radiological examinations. The incidence of MS was 1.18% during the study period, similar to previous studies.5,9 Nonprepared surgery for MS results in high rates of conversion and morbidity, and hazardous outcomes.5,7,8 Thus, improved diagnosis and surgical techniques are needed.
In previous studies, laparoscopic surgery for MS has been described for MS type 1 with proper preoperative diagnosis.5,7,9 However, no procedure has been described for the reduction of morbidity and conversion or for surgical procedures leading to success. This is the first report of a surgical principle and improved technique for MS.
Routine LC has a high risk of biliary injury compared to open cholecystectomy. 13 Traditionally, this risk can be overcome by using the “critical view of safety (CVS)” technique reported by Strasberg et al. 14 Yamashita et al. 15 reported a low rate of biliary injury under CVS. This procedure demands dissection to reveal the clear anatomy in Calot's triangle. However, CVS is difficult in surgery for MS because of the severe inflammation in Calot's triangle due to the impacted gallstone, and the surgeon can easily injure the biliary tree. Even careful dissection does not solve this problem because the dense adhesion and concrescence of the GB and CHD distorts the biliary anatomy. 16 Thus, the dilemma in the surgery for MS is that the CVS procedure for avoiding biliary injury causes biliary injury. This dilemma can be observed given that the most frequent reasons for conversion in MS are adhesions and uncertain anatomy. 9
The surgery for MS was not a simple cholecystectomy. The aim of the surgery was the repair of the biliary tree to remove the gallstone compaction to the CHD and perform a functional cholecystectomy. With our procedure, the surgeon must be aware of the dilemma associated with CVS in surgery for MS and recognize that CVS is not indicated in laparoscopic surgery for MS, preoperatively. Our preferable results are due to the principle of “no dissection of Calot's triangle” and show that laparoscopic partial cholecystectomy is a safe procedure for MS even though it is contrary to Strasberg's CVS technique. 14 In addition, partial cholecystectomy has been reported as a safe technique with a lower biliary injury rate to treat severe acute cholecystitis.10,16
However, partial cholecystectomy should be chosen carefully as MS has a higher reported incidence of malignancy. 17 In this study, we found 5 cases with GB carcinoma in the LC group and no cases in the MS group. A detailed and accurate preoperative diagnosis would be able to detect the GB carcinoma preoperatively. The recurrence of gallstones in the GB remnant is another concern of this procedure, with a reported rate of 2.2%. 10 Even though recurrence did not occur in any of our cases during the study period, the follow-up period was too short to rule out the recurrence of gallstones. Further study with long-term follow-up is needed to better understand the benefits and risks of partial cholecystectomy for MS.
Preoperative diagnosis for MS is critical in the decision for surgical strategy, particularly concerning the indication for CVS. However, several reports suggest that the preoperative diagnosis of MS is difficult and can only be made accurately in 0%–33% of patients.8,18,19 The sensitivity of ERCP and MRCP were reported to be 0%–100% and 50%, respectively.5,7,9,18 The accuracy of diagnosis varies depending on the case series. DIC-CT was also useful for diagnosis in this study. Thus, in the current study, accurate preoperative diagnosis ensured that the appropriate procedure was performed. The results also indicate that the image modality determines the findings of Calot's triangle; MRCP was the most sensitive in the detection of compression, stenosis, and disruption of the CHD. The combination of several image modalities and a high index of suspicion are important for an accurate diagnosis of MS and to avoid biliary injury.
Here, we demonstrate the safety of laparoscopic partial cholecystectomy without dissection of Calot's triangle for MS. This technique is a safe procedure for MS even though it is contrary to Strasberg's CVS technique. Thus, surgeons should reconsider the use of CVS in laparoscopic surgery for MS. In addition, an accurate preoperative diagnosis is critical in the decision of the surgical procedure to avoid bile duct injury.
Footnotes
Disclosure Statement
No competing financial interests exist.