
Abstract
Abstract
Purpose:
The robotic single-port access plus one conventional robotic port, a reduced-port robotic surgery (RPRS) for left-sided colon cancer, can enable lymphovascular dissection using the wristed instrumentation and safe rectal transection through an additional port maintaining the cosmetic advantage of the single-port surgery. The aim of this study is to compare the clinicopathological outcomes between reduced-port and conventional multi-port robotic colectomy for left-sided colon cancer.
Methods:
The study group included 23 patients who underwent an RPRS and 16 patients who underwent a multi-PRS (MPRS) for left-sided colon cancer between August 2013 and January 2016.
Results:
The operative time was significantly shorter in the RPRS group than in the MPRS group (mean time 258 ± 67 vs. 319 ± 66 minutes, P = .009). There were no apparent differences in tolerance of diet, postoperative pain score, length of hospital stay, the rate of postoperative complications, and the mean number of harvested lymph node, but the RPRS group had a significantly smaller total incision length (38 ± 12 mm vs. 83 ± 6 mm, P = .013).
Conclusions:
This study shows the feasibility and safety of the RPRS, with clinicopathological outcomes that is comparable with that of the MPRS for left-sided colon cancer.
Introduction
T
Robotic surgical systems were developed in part to overcome several of the inherent limitations of laparoscopic surgery and were introduced to colorectal surgery to overcome the challenges of laparoscopic dissection in the narrow, deep pelvis.10–14 However, the role of robotics in colonic surgery is still largely undefined. It is unclear whether robotic surgery has significant clinical benefits over laparoscopic surgery for treating colonic disease, because robotic colectomy has comparable clinicopathological outcomes, but higher costs and longer operative times than conventional laparoscopic surgery.15–18
Recently, robotic single-port access plus one conventional robotic port, a reduced-port robotic surgery (RPRS) was introduced for left-sided colon cancer, and this approach could enable precise lymph node dissection around the inferior mesenteric artery using the wristed instrumentation and safe rectal transection through an additional port maintaining the cosmetic advantage of the single-port surgery.19,20 Herein, we present our early experience with reduced-port robotic colectomy and compare the short-term oncologic outcomes with the results of the conventional robotic colectomy for left-sided colon cancer.
Materials and Methods
Between August 2013 and January 2016, a total of 168 patients underwent colonic resection for left-sided colon cancer at Dongsan Medical Center, Keimyung University, Daegu, Korea. After the exclusion criteria were applied, the study group included 23 patients who underwent an RPRS and 16 patients who underwent a multi-PRS (MPRS). Exclusion criteria were: open or laparoscopic surgery, patients with stage IV tumor, patients with synchronous or previous malignancies, patients presenting with acute obstruction or perforation, and patients who required en-bloc resection of adjacent organs due to locally advanced lesions.
Information regarding patient demographics was obtained from a prospectively collected DSMC Colorectal Cancer Database and included data regarding age, sex, American Society of Anesthesiologists grade, history of previous abdominal surgeries, preoperative carcinoembryonic antigen (CEA), and location of the tumor. Perioperative details included total operative time, conversion, the length of the total incision, time to first flatus, time to diet initiation, length of hospital stay, postoperative complications, and histopathological findings. The location of the tumor was categorized according to the location of the distal border of the tumor, as rectosigmoid colon (between 15 cm from the anal verge and rectosigmoid junction), sigmoid (between the rectosigmoid junction and brim of the pelvis), and descending colon (between brim of the pelvis and splenic flexure). Conversion to open surgery was defined as an interruption of the robotic approach, followed by laparotomy at any time, to complete the surgical procedure. Conversion to laparoscopic surgery was defined as an undocking of the robotic system, followed by laparoscopic surgery, before completion of the dissection procedure. Postoperative wound pain was measured using the numeric pain rating scale with endpoints labeled as “no pain” (scale of 0) and “worst possible pain” (scale of 10) on postoperative day 1 and 2. Surgical site infection was defined as the presence of clinical signs and symptoms of infection, which were based on definitions such as those described by the Centers for Disease Control and Prevention. 21 Tumor stages were classified in accordance with the American Joint Committee on Cancer (AJCC) 6th Edition staging system. This study protocol was approved by the Institutional Review Board of the Dongsan Medical Center, and informed consent was obtained from all patients.
Surgical technique of the multi-port robotic colectomy
If the intervention was a left hemicolectomy, the colon was divided distally to the tumor at the level of the sacral promontory, without redocking (single docking) and anastomosis was carried out with a double stapling or hand-sewn technique. On the other hand, if the procedure was an anterior resection, rectal dissection with redocking was performed (dual docking), in accordance with tumor-specific mesorectal excision principles (Fig. 1). Operations with dual docking comprised two stages: colon stage and pelvic stage. Patients were put in the Trendelenburg position at 30°and tilted down toward the right side, at an angle of 10–15°. Six ports were used, including one 12 mm camera port and five 8 mm robotic working ports (Fig. 2A). During the colonic stage, the patient cart was positioned over the left flank, approaching the patient at an angle of ∼15. The surgical cart was then placed oblique to the surgical table, and docking of the robotic ports was completed. After completion of the colonic stage, the da Vinci arms were undocked and the operating table was rotated 60°counterclockwise, until a 45°angle was created between the patient cart and the operating table (Fig. 1). For transition from the colonic stage to the pelvic stage, the second robotic arm was moved from R2 to R4 and the third robotic arm was moved from R3 to R5 (Fig. 2A). After redocking, rectal dissection using tumor-specific mesorectal excision principles was performed. The rectum was divided using a laparoscopic or robotic stapler. The tumor specimen was extracted through the incision of the left lower trocar and end-to-end intracorporeal anastomosis was carried out, with a double stapling technique. A suction drain was placed in the pelvic cavity.

Dual docking technique in robotic colectomy for left-sided colon cancer.
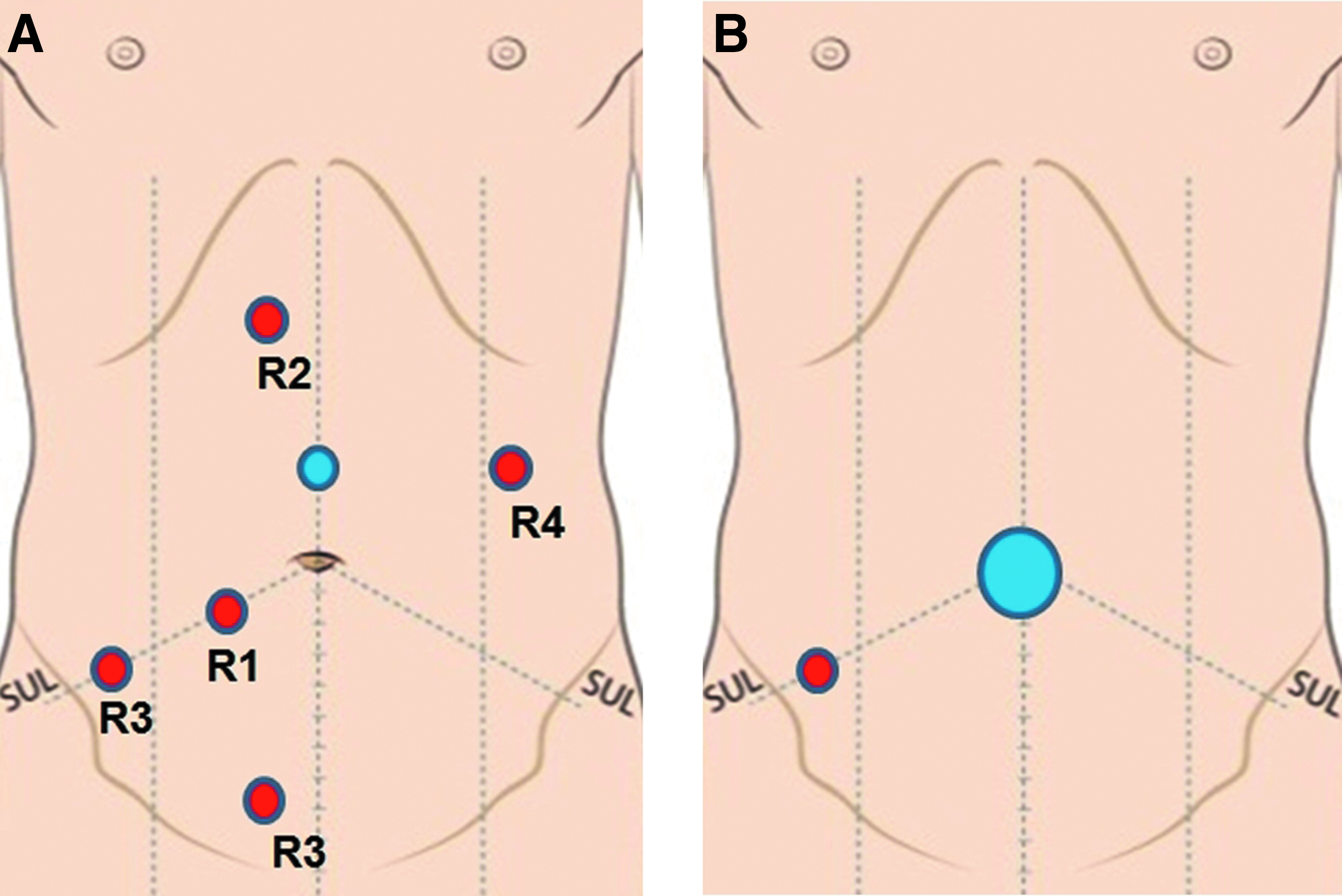
Port placement for totally robotic colonic surgery.
Surgical technique of the reduced-port robotic colectomy
A single 2.5 cm vertical incision was made through the umbilical skin and the single-port was inserted into the intraabdominal cavity (Fig. 2B). We used the Single-Site® port (Intuitive Surgical, Sunnyvale, CA) or Glove port (Nelis, Bucheon, Korea), as access ports. An additional 8 mm conventional robotic port for the EndoWrist ® system was inserted into the right lower quadrant, under direct vision. The robotic cart was then placed oblique to the surgical table, at an angle of 45°. The camera arm was docked to the corresponding trocar and the endoscope was reinserted and attached to the camera arm. Lubricated 5 × 250 mm curved cannulas were inserted through the single port. For distal bowel resection, laparoscopic or robotic linear staplers were introduced through the additional port in the right lower quadrant area and this port site was used for the pelvic drain placement.
Statistical analysis
Clinical characteristics and variables were compared between the RPRS and the MPRS groups by using a Mann–Whitney test for continuous data or a chi-square test for categorical data. P-values of less than .05 were considered indicative of statistical significance. Statistical analyses were performed with IBM SPSS 20.0 software (SPSS, Inc., Chicago, IL) and data were expressed as mean with standard deviation.
Results
Patient characteristics
The demographic characteristics such as age, body mass index, and physical status according to the American Society of Anesthesiology status, preoperative CEA, location of tumor, and number of previous abdominal operations did not differ significantly between the RPRS and MPRS groups (Table 1).
RS, robotic surgery; SD, standard deviation; ASA, American Society of Anesthesiologists; CEA, carcinoembryonic antigen.
Perioperative clinical outcomes
All 39 procedures were technically successful, without the need for conversion to open surgery (Table 2). However, 1 patient (4.3%) with rectosigmiod colon cancer required conversion from RPRS to reduced-port laparoscopic surgery, because of air leak from the Single-Site port and external collisions. The operative time was significantly shorter in the RPRS group than in the MPRS group (mean time 267 ± 69 vs. 319 ± 66 minutes, P = .009). In the RPRS group, the operative time curve showed that the total operative time decreased as experience accumulated, with a mean operative time decrease of 304 minutes for the first 9 patients and 229 minutes for the rest of the patients (P = .020) (Fig. 3).
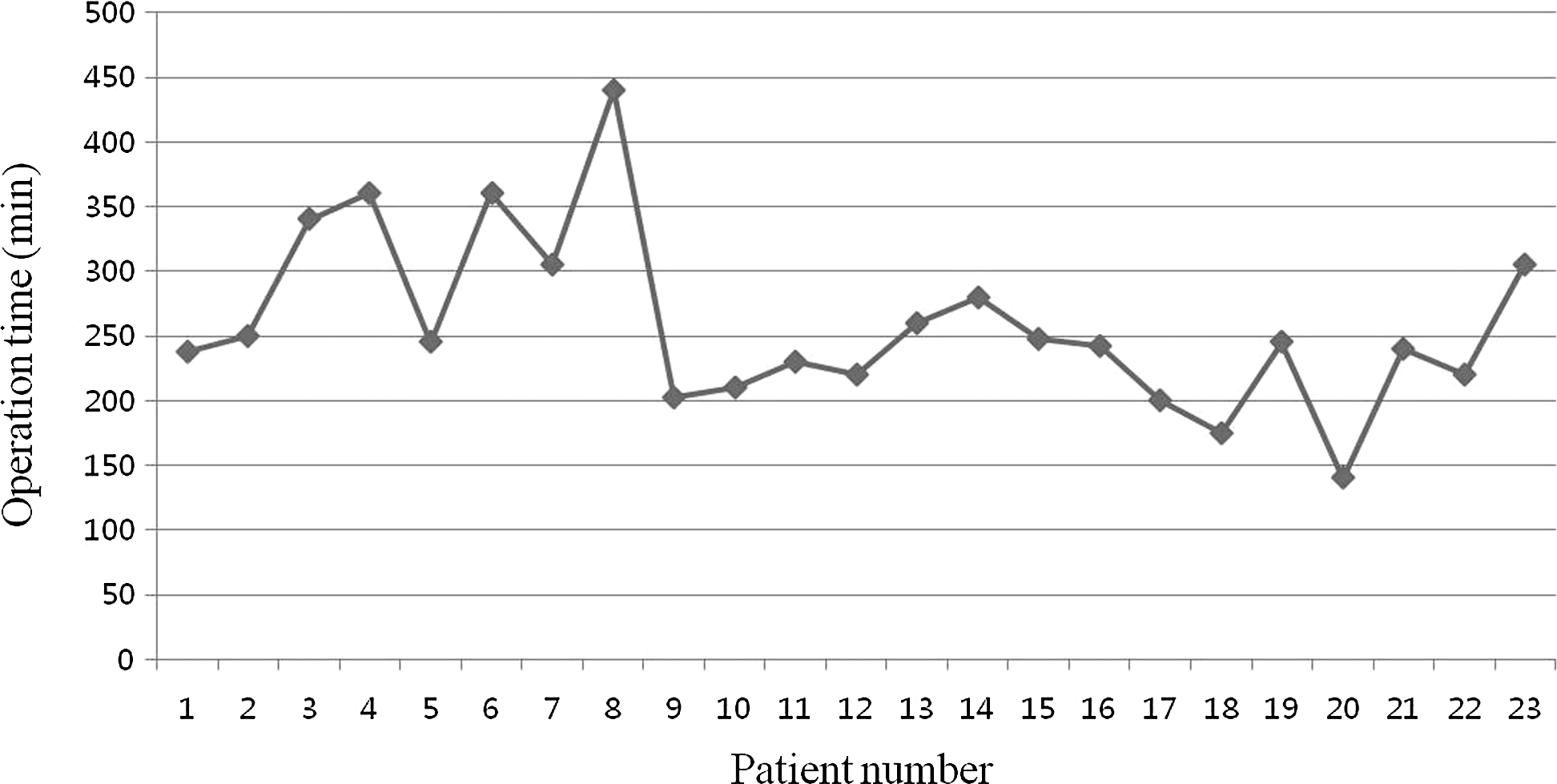
Operation time curve of reduced-port robotic colectomy for left-sided colon cancer.
All surgical site infections were superficial surgical site infection.
RS, robotic surgery; SD, standard deviation; NRS, numeric rating scale; POD, postoperative day.
There were no apparent differences in the time taken for return to a normal bowel function, tolerance of diet, length of hospital stay, or pain score (measured on the numeric rating scale, on postoperative day 1 and 2), but the RPRS group had a significantly smaller total incision length (RPRS: 38 ± 12 mm vs. MPRS: 83 ± 6 mm, P = .013). Morbidity within 30 days after surgery was comparable between the two groups (21.7% vs. 12.5%, P = .460). Among patients included in the RPRS group, 5 patients developed postoperative complications: 2 patients developed superficial surgical site infection, 1 patient developed voiding difficulty, 1 patient developed pseudomembranous colitis, and 1 patient developed ileus. Among patients included in the MPRS group, 2 patients developed postoperative complications: 1 patient developed ileus and 1 patient developed chyle leakage. There were no severe complications that required reoperation or intervention or mortality within 30 days of surgery in either group.
Postoperative pathologic outcomes
There were no differences in stage distribution, size of tumor, histological differentiation, and the proportion of patients with lymphovascular invasion (Table 3). The mean numbers of harvested lymph nodes (19.5 ± 8.4 vs. 20.8 ± 9.9, P = .680) and proximal resection margins (14.2 ± 17.7 vs. 16.7 ± 4.2, P = .760) were comparable between the two groups. The distal resection margin in the RPRS group was significantly longer than that in the MPRS group (4.7 ± 2.9 vs. 2.6 ± 1.6, P = .036).
RS, robotic surgery; TNM, tumor node metastasis; SD, standard deviation; LNs, lymph nodes; PRM, proximal resection margin; DRM, distal resection margin.
All T4 tumors were T4a.
Discussions
Data from our study demonstrate the feasibility and safety of the RPRS, with clinicopathological outcomes that is comparable with that of the MPRS for left-sided colon cancer. The 30-day postoperative complication rates were 21.7% in the RPRS group and 12.5% in the MPRS group, without major complications and none of these procedures had to be converted to an open surgery. These findings are consistent with those of previous studies, which reported a morbidity rate of less than 20% and a very low conversion rate for robotic colorectal operations.10,22 The mean numbers of harvested lymph nodes and proximal resection margin between the two groups were comparable, although the distal resection margin in the RPRS group was significantly longer than that in the MPRS group; these are higher than the minimum length recommended for both groups.23,24
In the present study, the operative time was significantly shorter in the RPRS group than in the MPRS group (267 vs. 319 minutes). The results of our study could be associated with multiple dockings of the robotic cart, a greater number of port placements in the MPRS, and/or selection bias with regard to different time periods of each procedure. Since the time when we first used a robotic system to perform colorectal cancer surgery (August 2013), we have adopted a MPRS for general colon cancer surgeries as well as developed the RPRS for left-sided colon cancer surgeries (August 2014). 19 Kim et al. 25 reported that the learning curve for single-port laparoscopic anterior resection for sigmoid colon cancer was 61–65 cases according to multidimensional statistical analyses. The operative time curve showed that the total operative time decreased as experience accumulated in the RPRS group, associated with a mean operative time decrease of 304 minutes for the first 9 patients and 229 minutes for the rest of the patients (P = .020), despite an ongoing learning curve (Fig. 3). Although the adoption time of MPRS was earlier and time periods of each procedure varied, we believe that the RPRS approach can overcome the learning curve typically experienced with conventional single-access laparoscopic surgery.
Cosmetic benefits were naturally expected from the early descriptions of single-port laparoscopic procedures, given that a reduced incision length logically equals improved cosmesis. Gasior et al. 26 reported that patients or parents expressed better scar assessment with the single-port laparoscopic surgery, when compared with the multi-port surgery for appendicitis, at early follow-up. Ostlie et al. 27 demonstrated that patients perceived overall superior scar assessment at long-term follow-up after single-site laparoscopic versus four-port cholecystectomy. In the present study, the RPRS group had a significantly smaller total incision length (RPRS: 38 mm vs. MPRS: 83 mm). This result can be associated with cosmetic benefits, although prospective data regarding scar assessment are lacking.
Single-Site platform has limited availability of instruments and accessories. For the Single-Site system, there are only two lengths of curved cannulas, 250 and 300 mm. The distance between the tip of the instruments and the operative field is too close, because even 250 mm curved cannulas are too long for the dissection around the central vascular trunk. In this study, we lifted the remote centers of R1, R2 cannulas, and camera port upward, out of the abdominal wall, to shorten the distance between the tip of the instruments and the operative field and to secure the surgical space (Fig. 4). We are confident that this approach could be improved by the development of various lengths of cannulas that are not yet available in the future.

Adjustment of remote centers to secure the surgical space.
Regarding access port, in our experience, although the Single-Site port was designed for the Single-Site platform, lack of durability and occurrence of air leaks were observed when the remote centers of the robotic ports were placed at the level out of the abdominal wall. 20 In initial 12 cases, we used the Single-Site port as an access port, and this was changed to the Glove port in 6 patients. Because Glove port is transparent, we could easily adjust the level of remote centers out of the abdominal wall and problems related to air leaks resolved after changing access port.
The Single-Site platform has limited range of motion for robotic instrument, when compared with the conventional robotic platform. In some patients, we encountered a limitation in the range of motion for the lymph node dissection around the inferior mesenteric artery and during splenic flexure mobilization. We thought that this problem was related to the inherent limitations of the Single-Site platform and we changed the docking technique. In this study, the initial 12 patients underwent anterior resection or left hemicolectomy by using a single docking technique, whereas the latter 11 patients underwent procedures by using a dual docking technique, the same as that for the MPRS. With the dual docking technique, the robotic system was first positioned beside the patient's left shoulder and then moved down to the coxal area, for rectal dissection. Once we changed the docking technique, the problems related to the limitation in the range of motion resolved.
In conclusion, this study shows the feasibility and safety of the RPRS, with clinicopathological outcomes that is comparable with that of the MPRS for left-sided colon cancer. The reduced-port robotic technique is a viable option, until a more advanced robotic platform, specifically designed for single-port surgery, is developed and a pure single-port robotic colectomy can be safely performed. However, we note that our study has several limitations, including its retrospective nature, the small group sizes, and the selection bias regarding varying time periods for each procedure. A randomized prospective comparative study is needed to demonstrate the significant benefit of using this technique in patients with left-sided colon cancer.
Footnotes
Author Contributions
Study conception and design: Bae, Baek, Jeong; Acquisition of data: Bae; Analysis and interpretation of data: Bae, Baek; Drafting of article: Bae; Critical revision: Bae, Baek; Final approval of version to be published: Bae, Baek, Jeong.
Disclosure Statement
No competing financial interests exist.