
Abstract
Abstract
In the last three decades, with the advancement of laparoscopic and thoracoscopic surgery, minimally invasive approaches for benign and malignant diseases of the esophagus have been developed and more experience is starting to accumulate across the world. Minimally invasive esophagectomy (MIE) has demonstrated acceptable lymph node retrieval, good postoperative outcomes, and low mortality. In this article, we review our preferred technique of MIE for adenocarcinomas of the gastroesophageal junction and distal esophagus.
Introduction
M
Benefits of MIE
Cushieri described the first MIE in 1993, 6 and since then, these techniques have evolved from the initial hybrid approaches (when thoracoscopy was combined with laparotomy)7–10 to the current MIE, which is performed entirely in a minimally invasive manner.11–18 Table 1 shows common surgical approaches to esophagectomy, including pros and cons.
MIE is associated with a significant operator-dependent learning curve. A recent study recognized that 35–40 MIEs are needed to gain competency. 19 However, once gaining the experience, the results of MIE are excellent. In their review of more than 1000 MIEs, Luketich et al. 1 reported an overall mortality of 1.7% with overall morbidity, mortality, lymph node harvest, and cancer outcomes similar to, or better than, most published series of open esophagectomy. Similar results have been reported in studies that compared MIE with open and hybrid esophagectomies. Nagpal et al., in their meta-analysis comparing MIE with open and hybrid esophagectomies, included 672 MIE and hybrid esophagectomies and 612 open esophagectomies. They found that there was no significant difference in 30-day mortality, MIE had lower blood loss, shorter hospital stay, and reduced morbidity and respiratory complications. 2 Additional studies found no significant difference in esophagectomy-related morbidity (i.e., anastomotic leak, anastomotic stricture rate, gastric conduit ischemia, chyle leak, vocal cord palsy) and a reduced use of narcotics from less postoperative pain.3–5,7,20,21 Dantoc et al. studied the oncologic outcomes of patients who underwent MIE. He reviewed 1586 patients (in 17 case-controlled studies) in which MIE was compared with open esophagectomy: lymph node yield was significantly higher in the MIE (median of 16 nodes compared with 10 nodes harvested in open esophagectomies, P = .03) and 5-year survival was similar between the two groups (12.5%–67% in the MIE versus 16%–57% in the open esophagectomies, P = .33). 4
Staging and preoperative workup
All patients with esophageal cancer should undergo multidisciplinary evaluation that includes surgeons, medical, and radiation oncologists, radiologists, and gastroenterologists. Clinical staging should be performed to assess tumor resectability with a computed tomography (CT) scan of the chest and abdomen, positron emission tomography (PET/CT), esophagogastroduodenoscopy (EGD), and, in some cases, endoscopic ultrasound (EUS). All surgical candidates should be screened for physical fitness to withstand major surgical intervention. If the patient has high-grade esophageal obstruction, an alternative to oral nutrition may become necessary. A feeding jejunostomy is preferred to a gastrostomy in the interest of preserving the stomach for use as a conduit during MIE. Surgical candidates should undergo pulmonary function tests and an electrocardiogram. If cardiovascular comorbidity is present, an echocardiogram and/or stress test should be included in the preoperative workup.
Preoperative chemoradiation, followed by surgery, is the most common multimodality treatment for resectable esophageal cancer in patients who are fit to undergo surgery and have locally advanced, yet resectable, tumors (T1b and N > 0, T2–T4a with any N). Multiple randomized trials have demonstrated the survival benefit for concurrent neoadjuvant chemoradiation.11,12,22–26
While several acceptable surgical approaches are available today, the type of esophageal resection and reconstruction should be tailored to the patient and based on tumor location, availability and suitability of the conduit, history of prior operations, surgeon experience, and patient preference. Moreover, the approach can be influenced by the surgeon's anticipated management of anastomotic leaks or other complications. For selected cases, in which potential jejunal or colonic transposition might be used, colonoscopy, abdominal arteriography, or computed tomographic angiography (CTA) is recommended. Last, bowel preparation should be planned before surgery.
Preoperative EGD and bronchoscopy
Patients undergoing esophagectomy should undergo EGD, which allows the best gross assessment of the proximal and distal extent of tumor spread, to determine the treatment effect and to assess pyloric patency. Because of the vagotomy that is incurred during esophagectomy, some surgeons choose to endoscopically inject Botox at this point to facilitate later gastric emptying. Alternatively, Botox may be injected during laparoscopy. Bronchoscopy complements the evaluation by assessing for endoluminal invasion or compression and esophagotracheal/bronchial fistula from the esophageal tumor when tumors extend more proximally.
Which body cavity to start with?
The decision regarding whether to start in the abdomen or the chest is crucial and is based on the tumor location, level of the planned anastomosis, and the extent of esophageal resection. Upper and mid-esophageal tumors are generally treated by total esophagectomy with esophago-gastrostomy at the neck. For this approach, the thoracic esophagus is mobilized before the abdominal and cervical portions of the operation. Cancers of the gastroesophageal junction and distal esophagus, of which adenocarcinomas are the most common in the Western world, can be approached in the same manner. However, esophagectomy with esophago-gastrostomy in the chest (Ivor Lewis esophagectomy) is often more favorable. In these patients, the abdominal portion should be performed first, followed by repositioning for the thoracic portion. Below, we describe our minimally invasive technique for such an approach to cancers of the gastroesophageal junction and distal esophagus.
Positioning
Abdominal positioning
Patient is placed supine and in semilithotomy position, both arms tucked at the sides.
Thoracic positioning
Standard left lateral decubitus positioning is used, either with thoracic bolsters or bean bag and an axillary roll. A 20° tilt toward the prone position is preferred.
Laparoscopic phase
(a) Port placement is shown in Figure 1. An open Hasson technique is usually employed through a supraumbilical incision for the placement of a 12-mm port. This provides a route for CO2 insufflation and becomes the main access for our preferred laparoscope, an Olympus Endoeye Flex camera. Note that if a rigid 30° laparoscope is used, it requires a more cephalad port placement due to the scope's shorter length and narrower viewing angle. The patient is placed in reverse Trendelenburg position. A 5-mm port is next placed in the right upper quadrant for a Lapro-Flex articulating liver retractor. A second 12-mm port is placed midway between the retractor port and camera port to accommodate an Endo GIA stapler, the scope, Endostitch device, or grasper. Last, two 5-mm ports are placed in the left upper quadrant for graspers and an energy source. We prefer the use of a Maryland tipped LigaSure device (Covidien®). Operative duties are shared between a surgeon who stands to the right of the patient and one who stands between the patient's legs. An optional assistant stands to the left.
(b) Exploration—to rule out metastatic disease. Common sites for metastases are the liver, including the falciform ligament, the greater omentum, and the peritoneal surfaces of the lesser sac and the pelvis. Adhesiolysis often needs to be performed in patients as well, especially in those with a prior history of abdominal surgery or infection. Occasionally, a prior jejunostomy must be taken down because it impedes dissection and mobilization.
(c) Greater omentum dissection—identification and preservation of the right gastroepiploic arcade is mandatory. Dissection usually starts at a level between the right and the left gastroepiploic arteries and carried cephalad toward the left crus. The omentum should be divided no closer than 2 cm from the gastroepiploic arcade. The stomach should be retracted medially and to the right, thus exposing the lesser sac and the retroperitoneal attachments. The left gastroepiploic vessels become attenuated at the fundus, so dissection can be carried out closer to the stomach. Extra care should be practiced with the division of the short gastric vessels as the spleen and splenic hilum are often closely attached to these vessels. After mobilizing this portion of the stomach, caudad dissection toward the pylorus should then be performed up to the base of the right gastroepiploic vessels.
(d) Esophagogastric dissection—here, adhesions and fibrosed tissue planes can often be present in the postneoadjuvant setting. The pars flaccida is opened and the right crus is identified, then the esophagus is dissected off the right crus, and access is gained into the posterior mediastinum. The phrenoesophageal membrane is opened and the esophagus is freed from its attachments to the posterior mediastinum. The gastroesophageal junction is lifted up and the dissection is carried posteriorly to identify the left crus.
(e) Celiac axis dissection—the celiac artery can be visualized in two ways: by elevating the stomach from the lesser sac, thus viewing it from below, or by retracting the stomach caudally and to the left, thus exposing it along the right crural axis. The dissection of fat and lymph nodes can then proceed at the left gastric pedicle, which is ultimately divided by an Endo GIA stapler. However, vigilance for a replaced or accessory left hepatic artery should be employed as they can be present in up to 20% of patients. If this is the case, then temporary occlusion of the left gastric artery should first be performed to assess hepatic perfusion. If vascular embarrassment is significant, the left gastric artery will need to be preserved, unless division can be safely accomplished at a separate branch from the replaced or accessory vessel.
Pyloric mobilization and partial Kocher maneuver—the pylorus and, if needed, the first portion of the duodenum should be freed up to reach the esophageal hiatus. Care should be taken to avoid injury to the structures of the hepatoduodenal ligament. Botox may be injected into the pylorus at this stage if not already performed endoscopically; alternatively, a pyloromyotomy or pyloroplasty may be performed as a drainage procedure. However, no consensus exists as to the best method of draining the pylorus.27,28
(f) Creation of the conduit—A 4-cm-wide conduit is created from the greater curvature through the use of serial firing of an Endo GIA stapler. The stomach is stretched along the long axis of the greater curvature by retracting the pylorus toward the right leg and the cardia toward the left shoulder. The first stapler firing utilizes a vascular load to divide the fatty border and vascular arcade near the left gastric artery at the level of the incisura. Then, multiple firings of larger staple loads (e.g., Covidien, purple cartridges) should create a tubularized conduit along the gastric body toward the cardia and medial fundus. Shorter staple lengths with a greater number of loads are desired to produce a longer conduit. Ultimately, the distal esophagus, in continuity with the cardia and lesser curvature, is excised from the remaining stomach. This proximal gastric portion constitutes the distal margin of the specimen. It is sutured to the tip of the conduit with an Endostitch device for later retrieval in the chest. It is aligned to maintain proper orientation when doing so. Some surgeons prepare a separate omental flap and attach it to this suture to bring omentum to the chest as an anastomotic buttress. Alternatively, additional omental fat can be left along the gastroepiploic arcade during mobilization of the stomach. While either may be desirable, too much fat can impede the delivery of the conduit into the chest unless the hiatus is widened. This, itself can later lead to herniation of abdominal contents into the chest, unless steps are taken to cinch down the hiatus during the thoracic phase of the operation. After completion of the conduit, a feeding jejunostomy is usually created, which also allows enough time to evaluate the perfusion of the conduit.
(g) Laparoscopic feeding jejunostomy—the ligament of Treitz is identified, and the jejunum is marched 30 − 40 cm distally. Briefly placing the patient in Trendelenburg position facilitates this action. An Endostitch (Ethicon®) is used to tack the jejunum to the abdominal wall in the left upper quadrant, just medial to the lowest 5-mm port. It is often helpful to momentarily reduce the amount of CO2 insufflation to avoid tension on the jejunum by allowing the abdominal wall to be pushed downward while securing the bowel. This maneuver also allows for tactile feedback during stitching by pushing the sutures against the compressing hand.
(h) The conduit is now reevaluated for perfusion and bleeding from the staple line. Adequate mobilization of the conduit is confirmed by bringing the pylorus up to the hiatus. Finally, the alignment of the conduit is reassured before finishing the abdominal phase.

Laparoscopic phase port positions.
Thoracoscopic phase
A double-lumen endotracheal tube or bronchial blocker is used for single lung ventilation. The patient is placed in the left lateral decubitus position. Tilting the patient 20° to a prone position enables the right lung to shift anteromedially, which exposes the posterior mediastinum and esophagus with less need for retraction. This position also enables a deeper dissection along the spine. 14 Usually, four ports are used (Fig. 2). All ports are 2 cm long. The first port is placed at the eighth intercostal space in the posterior axillary line. The Endoeye Flex scope is inserted, and under direct vision, additional port incisions are made at the seventh intercostal space behind the tip of the scapula and the fourth or fifth intercostal space at the anterior axillary line. These latter two port sites are mainly used for graspers, lung retraction, and suction. A fourth port site is introduced one to two interspaces above the insertion of the diaphragm, posteriorly overlying the esophagus, as determined by direct visualization. The scope is switched to this last port, which allows for the original camera port incision to be used for energy, graspers, suction, and an Endostitch. The operative surgeon stands to the left of the patient, and the first assistant stands to the right. Some surgeons prefer the use of light CO2 insufflation during the thoracic phase. While this creates a desirable degree of pneumothorax that pushes the lung forward and provides a wider space for dissection, the use of laparoscopic port devices are mandatory to maintain insufflation. This limits the type of instruments that can be used and it does not allow for the passage of multiple instruments through each port, which is occasionally preferred.

Thoracoscopic phase port positions.
The principles of the thoracic phase are as follows:
(1) Retraction of diaphragm and release of the inferior pulmonary ligament—the diaphragm is retracted cephalad directly over the esophagus. An Endostitch is used to place a figure-of-eight stitch through the diaphragm, and the suture is pulled through the lower anterior port and secured outside the chest so that the diaphragm is pulled away from the lower esophagus. Next, the inferior pulmonary ligament is taken down. This allows cranial and anterior traction of the lung for better exposure of the posterior mediastinum. Level 9 lymph nodes can be dissected and sent for pathology. (2) Posterior pleural dissection—the posterior pleura is opened in continuity with the release of the inferior ligament and dissected cranially up along the posterior hilum to the level of the azygos vein. Deeper dissection is performed to mobilize the esophagus. Particular attention should be paid to the carinal region where the left and right main stem bronchi can be easily injured. Postneoadjuvant radiation changes can make the dissection more challenging. Subcarinal lymphadenectomy is performed, and adequate hemostasis of the supplying bronchial vessels with energy must be balanced with the risk of airway injury. Oftentimes thermal injuries only declare themselves after gradual tissue breakdown in the later postoperative period. However, if an airway injury is readily apparent during surgery, immediate primary repair is recommended. Repairs to the left mainstem bronchus require vigilance to the bronchial cuff of a left-sided double-lumen endotracheal tube. A decision to perform the repair thoracoscopically versus open is based upon the judgment of the surgeon. The pleura is also opened posterior to the esophagus adjacent to the spine. The esophagus is dissected circumferentially. Care should be practiced in the posterior aspect of the esophagus so as not to injure the thoracic duct, which runs in the groove between the spine and aorta. If the thoracic duct is observed, proximal and distal suture ligation or clipping can be done to prevent chyle leak. (3) Azygos vein—the azygos vein is divided using an Endo GIA with a vascular load. Alternatively, some surgeons advocate leaving the vein intact to align the conduit and to prevent volvulus or conduit distention. (4) Proximal mobilization of the esophagus—for an Ivor Lewis transthoracic anastomosis, it is preferable that the anastomosis be located a few centimeters proximal to the azygos vein. Given the propensity for intramural spread of disease, and to encompass the presence of Barrett's, a higher level is often desired. The proximal esophagus should be freed further by 4 cm to prevent tension on the anastomosis. The distal esophagus is then pulled cephalad to retrieve the abdominal portion of the esophagus and gastric conduit. Care must be taken to maintain the same orientation of the conduit so as to avoid twisting. Bear in mind that the gastric staple line, once seen to the right in the abdomen, is now seen facing upward given the decubitus position of the patient.
Esophagogastric anastomosis
A properly performed anastomosis requires alignment, an adequate blood supply, limited tension, and patency. A thoracoscopic esophagogastrostomy can be performed with either a linear or circular stapled anastomosis.13,29 The circular stapled technique has been the most widely used given its relative technical ease and suitability for anastomoses that can reach the upper chest. The linear stapled, or side-to-side, method has the advantage of a lower stricture rate because of its potential for a wider anastomosis. However, its dependence on a larger portion of the esophagus and gastric conduit limits its use to the mid to lower chest.
The surgeon should inspect the length of the conduit and choose the highest portion of the proximal esophagus that will align with the conduit for a tension-free anastomosis. It is desirable to join the conduit below the tip created from the fundus, thereby excluding this relatively ischemic region. The nasogastric tube is pulled back and the esophagus is transected with cold laparoscopic shears at the planned level of anastomosis. The sutures adjoining the distal specimen to the conduit are cut, and the posterior camera port incision is widened to 3–4 cm. The scope is placed anteriorly, and the specimen is placed in a bag for retrieval through the widened incision. This is then sent to pathology for confirmation of free margins.
For the creation of the anastomosis, we prefer the circular stapled method. A 28-mm EEA stapler is used for most of our adult male patients, although a 25-mm stapler is also frequently employed in smaller patients. Of note, no randomized trial to date has compared the sizes of the circular stapler with regard to stenosis or need for dilatation. First, an Endostitch with 0 Ethibond that is cut to 20 cm is used to place a purse-string suture in an over and over manner around the circumference of the transected esophagus. This is accomplished by grasping the very edge of the esophagus from the top posterior port and suturing through the lower anterior port. The camera is positioned in the lower posterior port. It is important to ensure that mucosa is incorporated into each bite and that sutures are not placed more than 1 cm apart. The grasped portion of the esophagus should also be incorporated into the sutured tissue so that it is eventually excluded by the stapler. One should also avoid narrowing the lumen by inadvertently tightening the purse string. The suture is not yet tied at this point, but the Endostitch is kept in place. Next, a 20 Fr Foley catheter is inserted to balloon dilate the esophagus. A second grasper is inserted from the top anterior port so that the esophagus is held open at the 9 o'clock and 3 o'clock positions. Next, the stapler anvil is inserted alongside the camera from the lower posterior port into the esophageal lumen past the suture line. Since this port incision was widened from the delivery of the specimen, both instruments should be readily accommodated. A laparoscopic anvil introducer may be used for the insertion, although standard thoracoscopic instrumentation will suffice. The purse-string suture is then cinched down onto the anvil's post and secured using a standard knot-tying technique with the Endostitch. A second purse-string suture is placed above the first suture line in a continuous horizontal manner along the inside of the anvil's disc. This is performed by grasping the post from the top posterior port and suturing from the lower anterior port, again using an Endostitch with 0 Ethibond that is cut to 20 cm. This suture is also tightened around the post and then tied. Note that commonly, the anvil is inserted into the transected esophagus before any suturing. We have found that placing the first row of sutures beforehand is less technically challenging and equally reliable.
Next, a gastrostomy is created in the upper part of the gastric conduit parallel to its staple line just above the intended level of anastomosis. This is accomplished by grasping the tip of the conduit from the top posterior port and placing hot laparoscopic shears through the bottom anterior port. The gastrostomy needs to be long enough to accommodate the head of the stapler; 3 cm will usually be required. Suctioning of the gastric contents can be performed from the top anterior port. The camera is then switched to the bottom anterior port. The conduit is grasped at the 9 o'clock and 3 o'clock positions around the gastrostomy from the top two ports. The stapler is introduced into the chest from the lower posterior port. The stapler is oriented so that it is pointing upward and placed gently through the gastrostomy, and then it is pushed forward against the back wall of the conduit while the tip is pulled back over the stapler with the two graspers (Fig. 3). Now, the spike should be advanced from the stapler so that it pierces the back wall of the conduit. It is extended outward until an orange line is seen at its base. The tissue of the conduit sometimes needs to be pushed down onto the head of the stapler to expose this line. Next, the spike is married to the post of the anvil, clicked into place, and drawn inward for firing. If, at this point, there has been confirmation of free margins per frozen section, the stapler is fired. The stapler is then withdrawn, and the anastomotic rings are removed so that they can be sent to pathology. Next, the nasogastric tube is readvanced slowly by the anesthesiologist under direct vision so that it can be positioned distally into the conduit. The gastrostomy is closed by excising it as a gastric wedge with additional fires of the Endo GIA stapler. The stapler is inserted through the lower posterior port, while the edges of the conduit are held together from the upper ports. This additional staple line should follow in continuity with the conduit's original staple line. In addition, it should not end too close to the esophagogastric anastomosis, and leaving a somewhat redundant portion of conduit is acceptable for this reason (Fig. 4). The wedge resection is sent to pathology as a final gastric margin. The anastomosis is then wrapped with omentum, which was brought up into the chest with the conduit earlier, or it can be buttressed with adjacent pleura or a pericardial fat pad. Last, an Endostitch can be used to tack down the conduit to the diaphragm to mitigate the herniation of abdominal contents in the late postoperative period. This is especially helpful if the hiatus was widened for the delivery of the conduit or if a significant hiatal hernia was present beforehand.
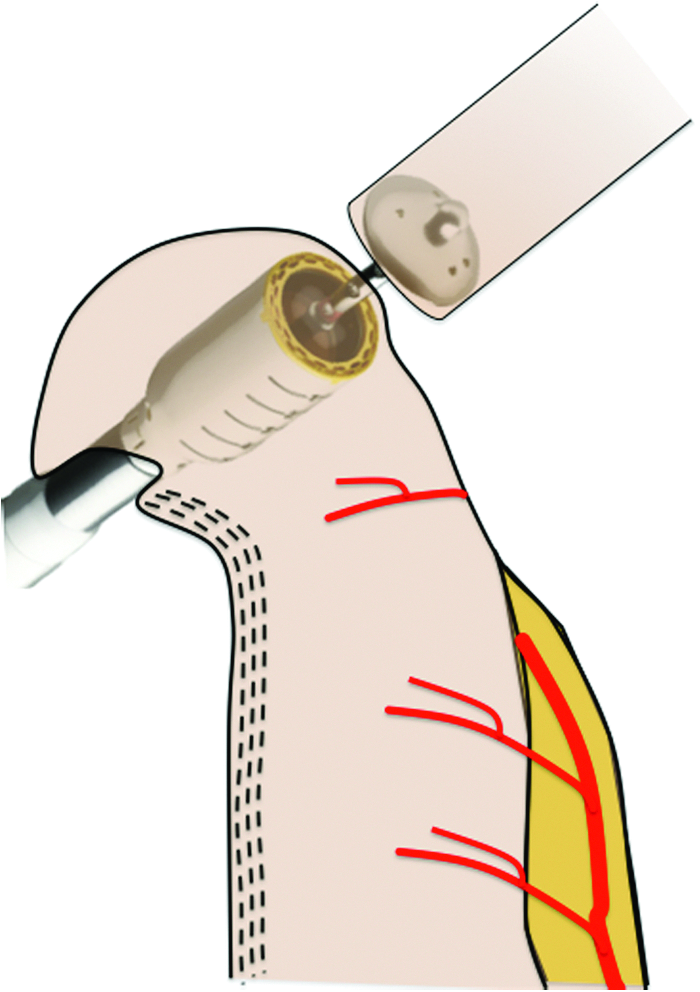
Esophagogastric anastomosis using the circular stapler technique.

Resection of gastrostomy that maintains a distance of at least 2 cm from the anastomosis.
Chest tubes are placed, the right lung is reinflated, and the port incisions are closed. Repeat bronchoscopy should be performed after placing the patient back in supine position, both for the clearance of secretions and to confirm that there has been no occult airway injury.
Lymphadenectomy
Lymph node involvement and lymphovascular invasion are considered poor prognostic factors in esophageal cancer. The extent of lymph node resection is a topic of controversy. Several studies favor extended lymphadenectomy,30–32
whereas others show there is no survival benefit from extended lymphadenectomy. Nevertheless, typical stations sampled are as follows:
• In the chest: periesophageal, subcarinal, and peritracheal nodes (levels 9, 8, 7, 4R, 2R). Several authors recommend en bloc resection of thoracic esophagus with the periesophageal nodes. The common practice is to send separate nodal stations and to label them for the pathologist. • In the abdomen: D1±D2.
33
Postoperative management
Patients are often extubated in the operating room and observed in the Intensive Care Unit for 24–48 hours. Liberal fluid resuscitation is practiced to assure adequate perfusion pressure to the conduit. A mean arterial pressure goal of 65 mmHg and above should be achieved without pressors to avoid conduit hypoperfusion. The patient's head should be at 30° at all times to avoid aspiration. At least one chest tube is kept until oral feeding is practiced (usually 1–2 days after a contrast study is performed). Trickle tube feeds are initiated on postoperative day 2 and subsequently advanced with the return of bowel function. The patient is encouraged to ambulate and aggressive chest physiotherapy is maintained to prevent respiratory complications. A contrast study is performed on day 7 with dilute barium to rule out leaks, anastomotic stricture, and to assure adequate emptying of the conduit down to the small bowel. Then, a clear liquid diet is initiated and advanced to full liquids. The patient is potentially discharged on postoperative day 9 with instructions on how to advance their diet while continuing supplemental tube feeds to maintain an adequate caloric intake.
Results
Over a period of 9 months, 7 patients underwent operations using the aforementioned technique. All patients were male veterans with adenocarcinoma of the distal esophagus at the VA Boston Healthcare System. Median age was 70, and 6 underwent neoadjuvant chemoradiation using the CROSS regimen. Operative mortality was 0%. One patient required conversion to laparotomy due to bleeding from the left gastric artery staple line. Mean estimated blood loss was 350 mL. Operative times are not reported due to variations in documentation. One patient developed a late postoperative leak from the gastric conduit staple line, 4 cm distal to the anastomosis. This was addressed successfully with drainage and stenting. None had vocal cord paralysis. One patient developed a symptomatic stricture requiring dilation 7 months after surgery.
Conclusions
MIE is a safe operation with similar oncologic outcomes when compared with traditional open esophagectomy. As technology has improved with the concurrent advancement of critical care and postoperative management, the complication risk of MIE has decreased significantly. Herein, we have described our technique for a minimally invasive Ivor Lewis approach that utilizes a semilithotomy position for the laparoscopic phase and a circular stapled esophagogastrostomy in the right chest. Our early experience in a VA setting has demonstrated acceptable results, although longer follow-up is needed to assess long-term complications such as stricture rate. Given the reported learning curve that exists for MIE, we expect measurable improvement in our outcomes that will parallel our increasing experience with this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.