
Abstract
Abstract
Background:
Liver resection or enucleation has been the basic treatment for liver hemangioma. However, there were few reports about laparoscopic surgery (LS) of hemangioma. The intention of this study is to explore the indication and efficacy of LS for laparoscopic hepatectomy (LH) and develop an opinion of these modern developments.
Patients and Methods:
Forty-four patients with LH underwent LS, with hemihepatic vascular occlusion (HVO group n = 24) or modified vascular occlusion (MVO group n = 20), and were retrospectively reviewed, including patients' demography, surgical technique, tumor size and location, blood loss, operation time, complications, modes of hepatic vascular occlusion and changes in postoperative liver function, and the difference in patients demography and operative outcome between HVO and MVO groups were compared as well.
Results:
There were no deaths. The mean operating time was 162 minutes, intraoperative blood loss was 335 mL, blood transfusion rate was 9.1%, postoperative complication rate was 18.2%, and length of hospital stay was 7.3 days. Although the tumor size in the HVO group was significantly larger than that in the MVO group, there were no differences concerning operating outcomes, length of stay, and postoperative serum alanine transaminase (ALT), aspertate aminotransferase (AST) level between the HVO and MVO groups.
Conclusions:
LS was feasible for LH with hepatic vascular occlusion with zero mortality and low complication rate.
Introduction
H
Patients and Methods
Patients
Between October 2004 and May 2012, 69 consecutive patients with LH underwent enucleation or liver resection at our institution. All procedures were performed by one doctor. Of these patients, 44 (63.8%) underwent laparoscopic surgery (LS). Because of the giant tumor size (diameter larger than 20 cm) and the special tumor location, the other 25 patients underwent open surgery. The primary indications for LS were abdominal pain (26 patients), Kasabach–Merritt syndrome (2 patients), tumor greater than 10 cm that grow rapidly (3 patients), uncertain diagnoses (2 patients), and a hemangioma become larger over a 6-month period. In addition, 9 patients with an asymptomatic LH underwent LS for concomitant abdominal diseases. Retrospective analysis of the patient data for these 44 cases involving LS, including patients' demography, surgical technique, tumor size and locations, blood loss, operation time, modes of hepatic vascular occlusion, changes in postoperative liver function, and complications, was performed. The patients were divided into two groups based on the occlusion method used: the hemihepatic vascular occlusion (HVO group n = 24) (Fig. 2a), in which all patients underwent liver resection for LH; and the modified vascular occlusion (MVO group n = 20) (Fig. 2b), in which all patients underwent enucleation at least (Table 2). The advantages and disadvantages of the various methods were determined.
Surgical Procedure
Body positioning and trocar placement
The patients were in a supine position with the head elevated higher than the feet and the legs apart and tilted 30° to the left or right according to the location of the lesion. The CO2 pneumoperitoneum pressure was less than 12–14 mmHg. For tumors in the right side of the liver, the trocars were placed in positions similar to those used for the four-hole laparoscopic cholecystectomy method, and appropriate adjustments were made based on the tumor location. If the lesions were located in the left liver, the primary incision ran from under the xiphoid process to under the left costal margin on the mid-clavicular line (Fig 1). A 30° laparoscope was used in all cases. The liver was examined visually and by intraoperative ultrasonography to confirm the number and size of the lesions and to define their relationships with the intrahepatic vascular structures.

Four-hole laparoscopic cholecystectomy method.
Hepatic inflow occlusion
The methods used in the study included HVO and MVO (Fig. 2a). HVO, which is similar to the half-Pringle maneuver and is widely used in hemi-hepatectomy, 11 clamps the tumor-side portal vein and hepatic artery branches (Fig. 2b). In contrast, MVO occludes the portal vein and tumor-side hepatic artery and is expected to reduce loss of bleeding for limited liver resection. In this process, the ipsilateral hepatic artery was first exposed, and then a tape was placed around the portal vein and the tumor-side hepatic artery. These vessels were occluded, and the contralateral (nontumor-side) hepatic artery was left open (Fig. 2b). To investigate the feasibility and safety of MVO, the efficacies, including operative outcomes, of the two modalities were compared.
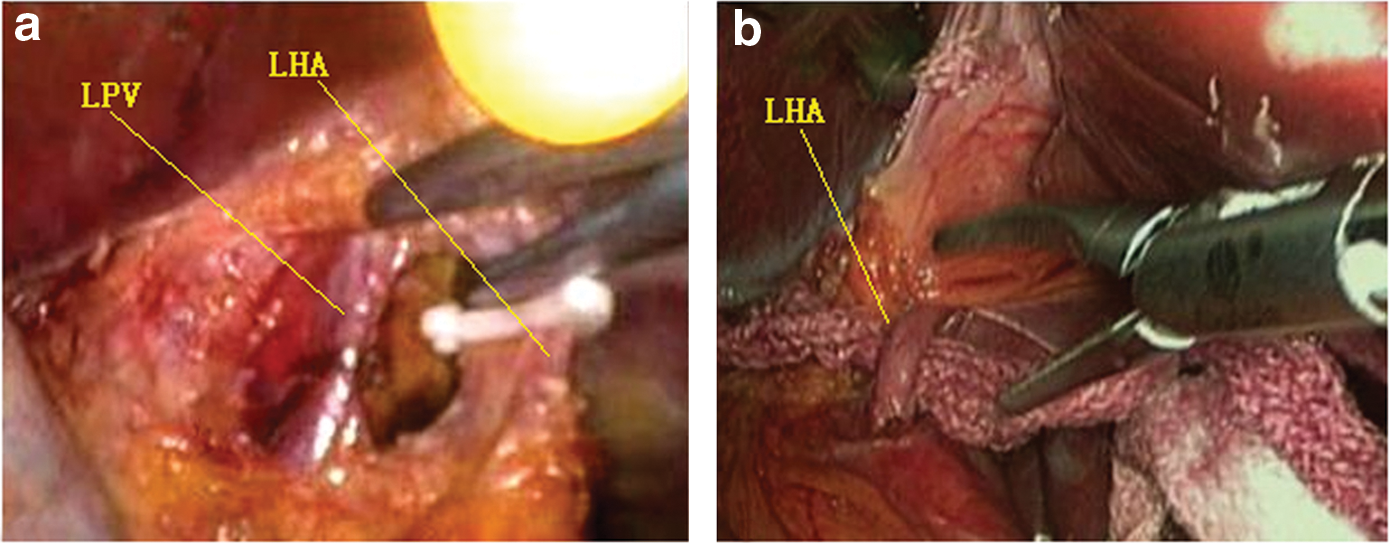
Photographs of hepatic inflow occlusion using
LS for hemangiomas
Enucleation was performed by dissecting the hemangiomas from the border of the normal liver parenchyma with a scalpel and suction. As bile ducts or blood vessels were encountered, they were secured and divided. Bleeding was controlled with clips, electrocautery at a power of 70–80 W, and sutures. Liver resection was performed via anatomic resections according to standard techniques. 12 The portal vein, hepatic artery, and bile duct were divided on the side on which the operation was performed. The hepatic veins were divided through liver parenchyma. Dissection was performed using an ultrasonic scalpel or electrocautery. Right hepatic lobectomy included the resection of segments V, VI, VII, and VIII (Fig. 3), and left hepatic lobectomy involved the resection of segments II, III, and IV (Fig. 4a,b). Nonanatomic resection refers to the resection of a hemangioma with the addition of some liver parenchyma. Histologic examination was used for certain diagnoses.
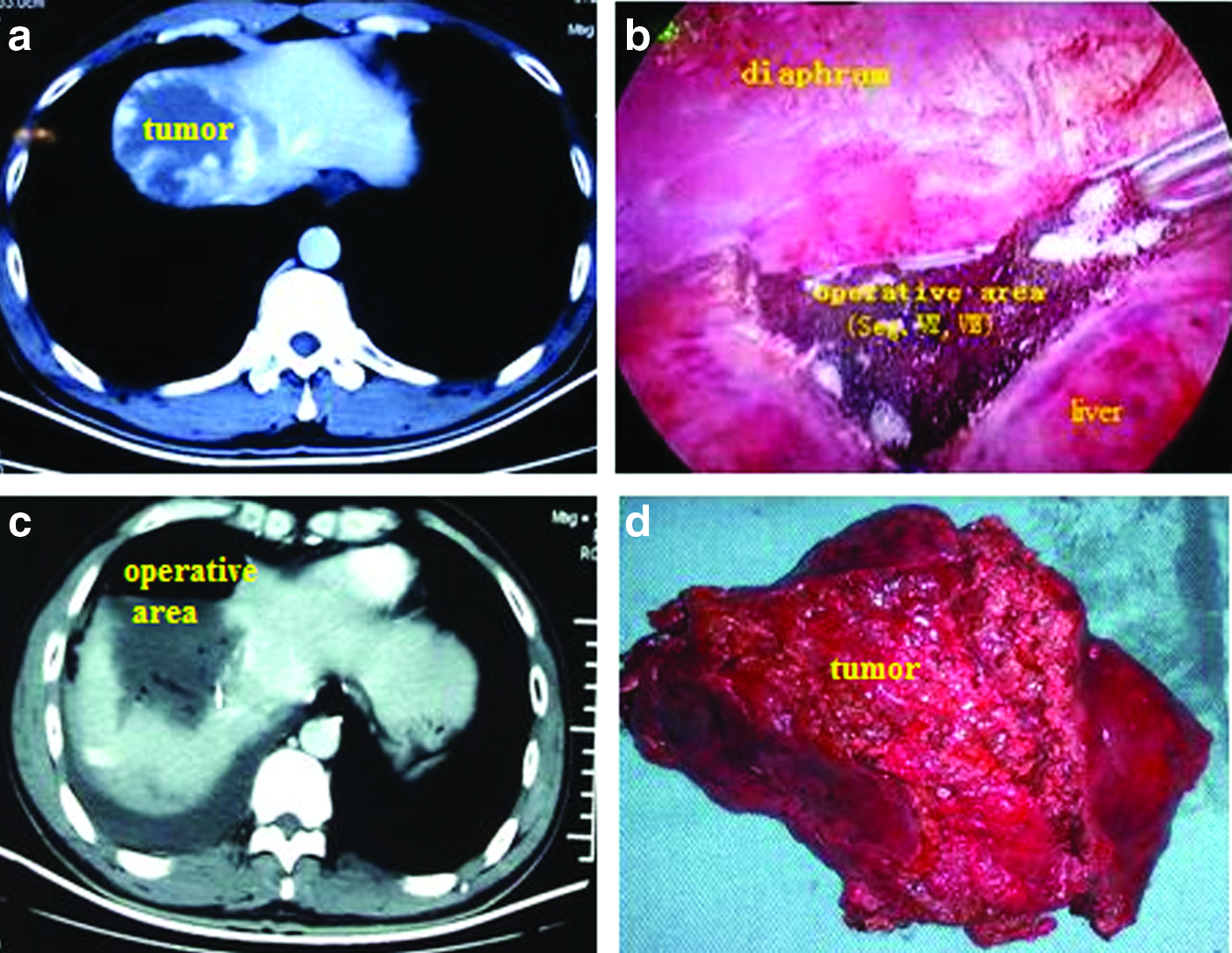
Hemangioma resection in segments VII and VIII.
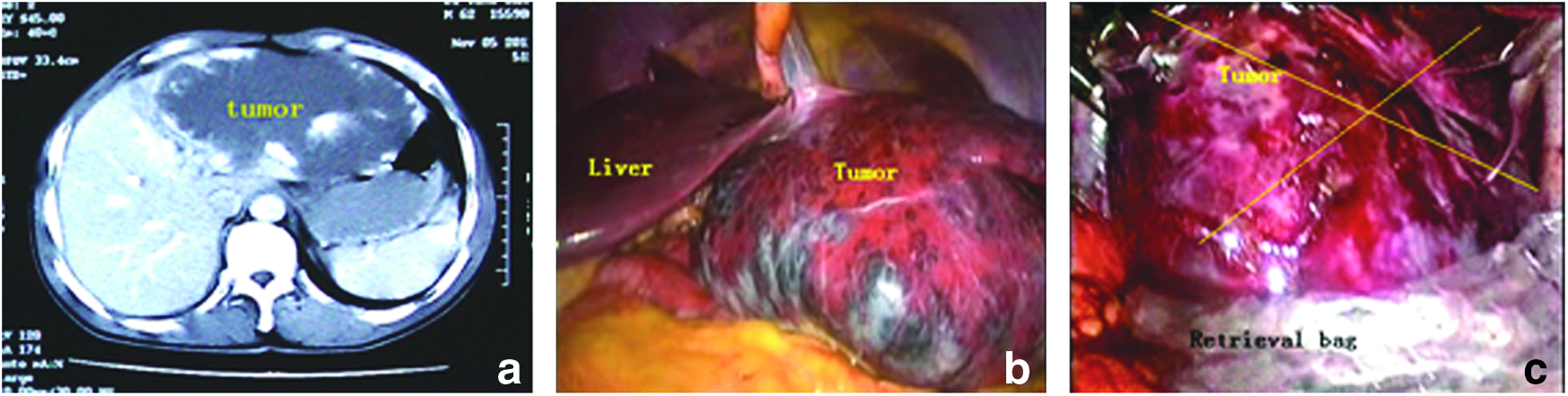
Left hemangioma resection in the liver.
Removing the excised tissue
The 12 mm trocar was removed, and its site was enlarged. An Endobag was inserted and deployed in the intra-abdominal cavity, and the excised tissue was placed in the specimen retrieval bag. The specimen retrieval bag was closed and brought against the anterior abdominal wall (Fig. 4c).
Statistical analysis
The clinical characteristics analyzed included blood loss, operation time, changes in postoperative liver function, morbidity, and mortality. These data were compared by the Student's t-test or χ2 test, using a statistical analysis program package (SPSS 15.0; SPSS, Inc., Chicago, IL). The results are expressed as the mean ± standard deviation. A probability of 0.05 or less (P < .05) was considered statistically significant.
Results
Patient characteristics and operative outcomes
There were 44 patients in the study group, 29 women and 15men, with a mean age of 48.3 years (range 28–72). The surgery for one patient was converted to open surgery (Table 1). The mean operative time of HVO and MVO groups are 170 minutes (range 90–260 minutes) and 147 minutes (range 100–250 minutes). The mean operative time was 162 minutes (range 90–260 minutes) and the mean blood loss was 335 mL (range 50–1000 mL). All of the patients recovered gastrointestinal function within 24–48 hours and were able to eat and get out of bed. According to the Clavien-Dindo classification of surgical complications, all of the complications are grades I to IIIa. The postoperative bile leakage rate was 6.8%, which lead to abdominal collection, and these leaks were treated with drainage for 2 weeks. The pleural effusion rate was 11.3%, and this complication resolved after diuretic therapy in all cases. The other complications were cured with conservative therapy (Table 1).
ASA, American Society of Anesthesiologists; BMI, body mass index; HVO, hemihepatic vascular occlusion; MVO, modified vascular occlusion; WBC, white blood cell.
Tumor location and operation mode
Size and location are considered important factors determining the feasibility of LS for LH. In the case of anterior and superficial lesions and lesions deep within the right hepatic parenchyma, enucleation is the indicated treatment, whereas large lesions located in a liver lobe that occupy most of the left or right lobe are treated with regular liver resection. Therefore, left lateral sectorectomy and left or right hemi-hepatectomy were usually adopted for the treatment of hemangiomata that occupied almost the entire lobe, whereas the tumors that occupied a small part of one or several lobes were removed by enucleation (Table 2). There were 5 cases of left lateral sectorectomy and 11 cases of left or right hemi-hepatectomy. The other cases involved tumor enucleation or concomitant regular liver resection.
HVO, hemihepatic vascular occlusion; MVO, modified vascular occlusion.
Concomitant surgery for abdominal disease
In the present series, some patients with LH underwent liver resection or enucleation during LS to treat other abdominal diseases. In these cases, the hemangiomas were not removed due to clinical symptoms or discomfort but to prevent the growth of the hemangiomas or its potential complications (Table 3).
Changes in the serum ALT and AST levels after surgery
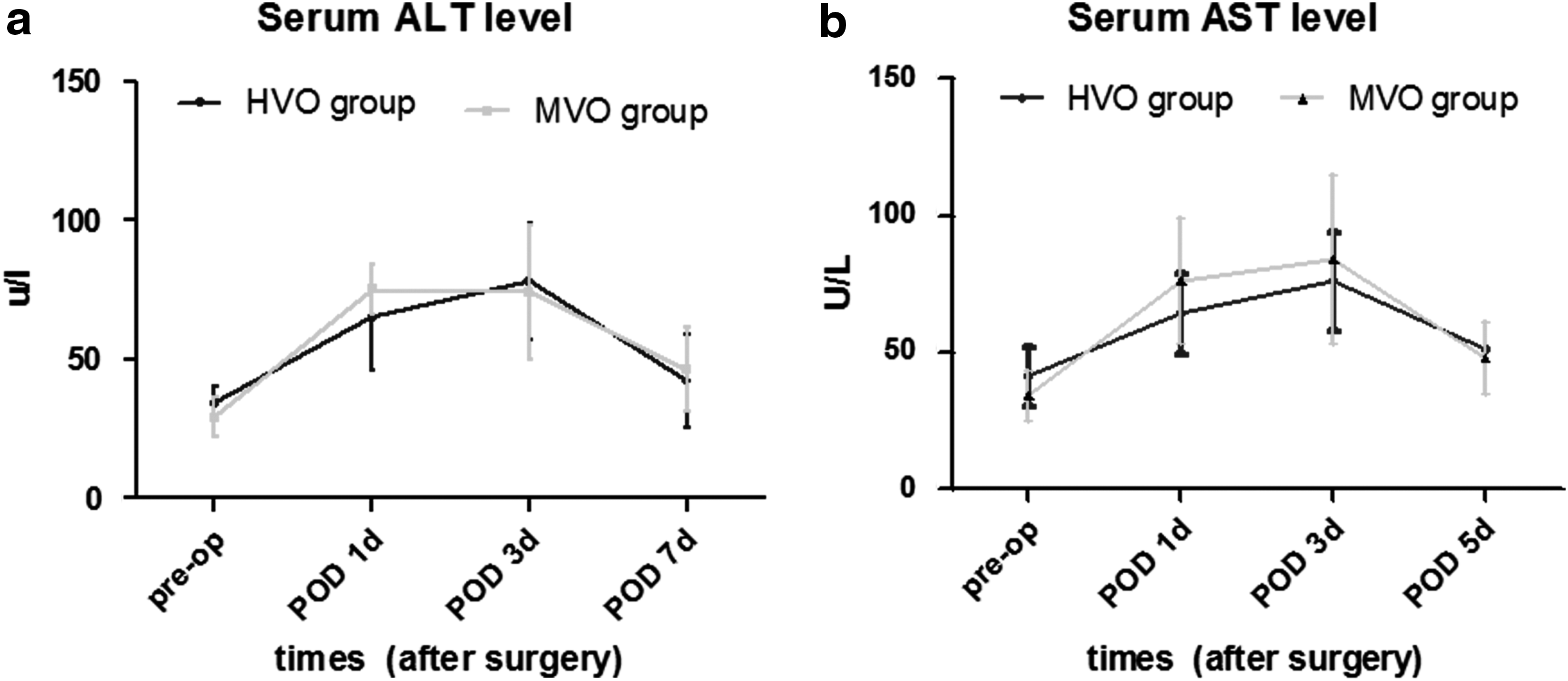
To reduce the intraoperative blood loss, HVO, which was demonstrated to result in less intraoperative blood loss and ischemic injury, has been regarded as the optimal option for hemi-hepatectomy; however, when performing limited liver resection or enucleation for the treatment of hemangioma, HVO is time consuming and thus may not be the best option. Therefore, we used a modified hepatic vascular occlusion method, referred to as MVO. This occlusion method was first used in hemangiomas surgeries. MVO is easier to perform, could greatly reduce blood loss (Table 1), and prevent the remaining liver from ischemic injury, as HVO could do. Figure 5a and b show that the changes in the serum alanine transaminase (ALT) and aspertate aminotransferase (AST) levels in the HVO and MVO groups were similar, also indicating no significant difference between the liver resection and enucleation for LH (P > .05).
Discussion
In outpatient clinics, patients with incidental hemangiomas are common, but most of these patients are asymptomatic, and the hemangiomas are small and require no treatment. Due to the benign and uncomplicated natural history of most hemangiomas, including giant hemangiomas, a policy of nonoperative treatment has been suggested for the majority of patients without clinical symptoms in many reports.3,5,6,10,11,13 However, some patients are at risk of potential complications and severe symptoms, and for patients who experience a surgical emergency due to hemorrhage, rupture, thrombosis, or infarction, surgery is the only treatment option.6–8,10 Farges et al. 14 followed up 163 patients for a mean duration of 92 months and found that the tumors in 9 patients increased in size, the observed complications included 2 cases of Kasabach–Merritt syndrome, 1 intrahepatic bleed, and 2 cases of Budd–Chiari syndrome. Sixteen patients underwent treatment, including eight resections, five arterial embolizations, two transjugular intrahepatic portosystemic shunts, one right hepatic artery ligation, and one liver transplantation. In a series of 115 patients, Yoon et al. 8 reported that there were 6 episodes of thrombosis and 3 cases of infarction or necrosis but no cases of rupture.
In recent years, a number of studies have revealed good long-term outcomes and a low complication rate with surgical treatment.7,8,15 Many authors have suggested that an LH combined with clinical symptoms, an LH of more than 10 cm, and an uncertain diagnosis are the “classical” indications of surgery,3,7,8,15 although the surgical indications for liver hemangiomas are controversial. However, since laparoscopic liver resection was first reported in 1992,16,17 this approach has been refined and has become common irrespective of the primary diagnosis. In the laparoscopic era, the treatment policy for LH, especially for patients with concomitant abdominal diseases that require surgery, should be based on the likelihood of operative injury or risk. In the present series, the patients who underwent LS did not experience severe complications, with minimal invasiveness. As long as the LH technically can be removed safely by LS, the removal of the LH during surgery for concomitant abdominal disease, which can reduce patients' concerns and prevent potential complications, may be justified and worth investigating further.
In the early stage, the suggested criteria for LH include the following: tumor location in segments II to VI, relatively marginal and superficial tumor location, and tumor size of 5 to 6 cm. Tumors located in segments I, VII, and VIII are difficult to expose, and the location of the tumor in one or more of these segments is considered as a contraindication for LS. A tumor size greater than 8 cm is also regarded as a contraindication due to the lack of sufficient space.18,19 With the accumulation of LH experience and the advancement of the surgical technique, laparoscopic resection has become relatively easy, and LS has become the gold standard for left lateral lobectomies and left hemihepatic resections.17,20–22 Because there is no risk of tumoral dissemination during LS for LH and because the tumor can be retracted or compressed, in the present series, LS was also demonstrated to be feasible for the total resection of segments VII and VIII, major hepatectomy, and the resection of tumors greater than 8 cm in size.17,18,23 In the present series, there were 19 patients whose tumors were more than 8 cm in diameter (the largest was 20 cm), and all of these tumors were successful excised. The resectability of giant hemangiomas using LS is determined by the exposure of the portal hilum and by having access to the vessels feeding the tumor. Once the tumor-side hepatic and portal vein branches were isolated and obstructed, the tumor shrank, facilitating the surgical procedure. In our study, the mean tumor size measured using the surgical specimen was 9.2 mm, and we did not consider large lesions or lesions located near the major vascular structures or in the central and posterior segments to be contraindications for the laparoscopic approach.
Since Hermann Pfannenstiel first reported the resection of a hepatic hemangioma in 1898, surgery has remained the only effective treatment.15,24 Alper et al. described a new technique of enucleation of hemangiomas in 1988. 25 This surgery involves the dissection of a fibrous cleavage plane between the capsule of the hemangioma and the surrounding normal liver tissue. Enucleation can be performed for any size of hemangioma, and this procedure has the advantage of not removing any liver parenchyma.14,24,26 However, regardless of the type of liver resection or enucleation for the removal of LH, massive blood loss has remained “the Achilles heel.” Baer 27 et al. reported that the median blood loss for the enucleation of 11 lesions in 10 patients was 800 mL, which compared favorably with the findings reported by Schwartz 2 (1750 mL) and Yoon et al. 8 (1680 mL). Other authors used preoperative transarterial embolization of the feeding hepatic artery to reduce intraoperative bleeding.28,29 Bleeding during laparoscopic transection occurs during open surgery and may be more difficult to control. Therefore, a very careful technique must be used, and the surgeon must be able to control most bleeding episodes laparoscopically. In the present series, hemi-hepatic vascular occlusion and modified selective hepatic vascular occlusion was used to control blood inflow during liver parenchyma transection, and these methods achieved a mean volume of blood loss of 335 mL, also showed that it can make hemangiomata shrink rapidly, providing more space to mobilize and dissect the tumor. Moreover, in this setting, the remaining liver retains at least one hepatic artery, which is reported to supply 50% of the total oxygen 30 and can protect the liver remnant from ischemia injury. Thus, the postoperative serum AST and ALT levels only rise slightly and rapidly return to normal (Fig. 1 and 2).
In open surgery, there are two surgical procedures for the treatment of liver hemangioma: enucleation and resection. Some authors advocate regular or anatomic liver resection,14,28–30 but others advocate enucleation.15,25 Although anatomic or nonanatomic liver resections have been advised for a long time, the technique of enucleation was first described in 1988. 24 There have been two comparative studies evaluating enucleation and resection for the treatment of LH in the literature6,13 and showed the enucleation had advantage over the liver resection in reducing loss of bleeding and incidence of intra-abdominal complications. However, in our study, the operative time, blood loss, and blood transfusion requirement for anatomic liver resections (HVO group) were similar to those for enucleation (MVO group). In fact, the liver parenchyma transection technique and the enucleation technique were simultaneously adopted in same patient, in case the tumor was located deep within the liver parenchyma in several lobes, the superficial liver tissue covering the tumor had to be transected to find the demarcation and provide a large field of view to dissect a fibrous plane between the tumor and the surrounding liver tissue. Usually, the two techniques can not be independently adopted for liver hemangiomas.
In conclusion, the use of laparoscopy for both liver resection and enucleation with hepatic vascular occlusion for hemangiomas was feasible, with zero mortality and low complication rate, even for tumors in special locations. The simultaneous excision of asymptomatic hemangiomas during LS for another abdominal disease may be justifiable based on the balance between low complication rate and potential growth of tumor.
Footnotes
Disclosure Statement
No competing interests exist.