
Abstract
Abstract
Background:
Advent of minimally-invasive esophagectomy necessitated the incorporation of stapled anastomotic techniques especially for intrathoracic anastomosis. We present our approach to the Ivor Lewis esophagectomy highlighting a simple modification in the anastomotic technique and review our experience with anastomotic outcomes.
Methods:
With IRB approval, patients who underwent Ivor Lewis esophagectomy with circular-stapled end-to-end anastomosis (EEA) were identified, divided into three equal sequential cohorts (A, B, and C), and compared for perioperative outcome. Cohorts were divided in a chronological order to have equal number of patients in each group.
Results:
Seventy-five patients underwent Ivor Lewis esophagectomy with circular stapled (EEA-25/28) anastomosis. Group A had longer median postoperative hospital stay and median postoperative ICU stay compared to Groups B and C. Ten patients (13%) had anastomotic leak—one patient required redo-anastomosis and other patients were managed with endoscopic interventions. There was significant decrease in rate of anastomotic leak with experience (8 versus 1 versus 1, P = .004). There were two perioperative deaths, one each in Groups A and C, including one death due to anastomotic leak (Group A).
Conclusion:
Use of simple modifications to stapled EEA, as described here, has led to decrease in anastomotic leaks following Ivor Lewis esophagectomy.
Introduction
I
Surgery is the mainstay of treatment for locoregional esophageal cancer. However, it continues to be associated with high morbidity and mortality. Anastomotic leak is the Achilles heel of esophageal resection and is associated with significant morbidity and in-hospital mortality. Anastomotic leaks following neck anastomosis are reportedly more common than intrathoracic anastomosis, but are easier to manage.3,4 With lower esophageal tumors, Ivor Lewis esophagectomy with intrathoracic anastomosis additionally avoids the neck dissection and associated risk of laryngeal nerve injury. It has been suggested that esophagogastric anastomotic technique influences the outcomes and predicts the chances of anastomotic leak. 5 Stapled anastomosis following open or minimally invasive esophageal resection can be done by modified Collard side-to-side linear-stapled technique or EEA (end-to-end anastomosis) circular-stapled anastomotic technique. Lower leak rates have been reported with stapled anastomosis compared to hand-sewn anastomosis.5,6
With the introduction of minimally invasive esophagectomy, the perioperative and clinical outcomes of esophagectomy patients have improved. 7 A thoracoscopic hand-sewn anastomosis is technically challenging and time-consuming, making stapled intrathoracic anastomosis more desirable. A circular EEA-stapled anastomotic technique is commonly used, but was associated with a high leak rate in our early experience. Subsequently, we have made simple modifications to standardize the technique with a resultant decline in the anastomotic leak rate. This study reviews our experience and outcomes with standardization of technique.
Materials and Methods
After Institutional Review Board approval, we queried the prospectively maintained Esophageal Center Database to identify patients who underwent esophageal resection between September 2007 and August 2015. Patients with transhiatal approach, cervical anastomosis, or hand-sewn intrathoracic anastomosis were excluded. The patients who underwent Ivor Lewis esophagectomy with intrathoracic anastomosis using EEA circular stapler constituted the study cohort. Surgeries of all included patients were done by a single surgeon (S.K.M.). Included patients were divided into three equal sequential cohorts (Groups A, B, and C). Medical records of the patients were reviewed for age, gender, preoperative weight loss, body mass index (BMI) at the time of surgery, comorbidities, neoadjuvant therapy, perioperative outcomes, and endoscopic evaluation after surgery. Endpoints included anastomotic leak rates and operative morbidity and mortality. Anastomotic leak is defined as disruption of the anastomosis identified radiographically as an extralumination of contrast of any size from the site of intrathoracic anastomosis on routine esophagogram or chest computed tomography, clinically by altered chest tube drainage, endoscopically or during reoperation [Type II and above of ECCG (Esophagectomy Complications Consensus Group) classification 8 (Table 1)]. On the basis of the clinical presentation and radiographic findings, anastomotic complications with ECCG grade 2 or above are defined as anastomotic leaks. Perioperative and 30-day mortality was included. Perioperative morbidity was defined as postoperative complications of Clavien-Dindo grade 2 or higher. 9
GI, gastrointestinal.
Surgical Procedure
Ivor Lewis esophagectomy comprises of two steps: transabdominal mobilization of stomach and fashioning of conduit followed by transthoracic esophageal resection and intrathoracic esophagogastric anastomosis.
Abdominal part
Procedure is done either by laparotomy or laparoscopic approach. Open procedures are done by midline laparotomy incision. For laparoscopic approach, standard five ports are used along with additional 5 and 12 mm trocars placed in the left lower quadrant and right lower quadrant, respectively, for the feeding jejunostomy tube placement (Fig. 1). Celiac axis lymphadenectomy is done and left gastric vessels divided. Greater curvature of stomach is mobilized preserving the gastroepiploic arcade, including the division of short gastric vessels upto the hiatus. A cuff of crus is included with the specimen. With the help of penrose drain retraction, dissection is done into the lower mediastinum.

Port placement for laparoscopic and thoracoscopic approach.
Lesser curvature mesentery is divided at the level of the incisura and serial loads of linear GIA stapler (Endo GIA™ Reinforced Reload with Tri-Staple™ Technology 45 mm, 3.5/4 mm staple size; Covidien, Mansfield, MA) are used first perpendicular to the lesser curvature and then parallel to the greater curvature (Fig. 2). We believe that a narrow tube, about 3–4 cm wide is better for a long-term function. A feeding jejunostomy is placed distal to ligament of Treitz. Drain is placed into left pleural space and brought out through the left upper quadrant. We do not routinely do a pyloric drainage procedure.

Figure showing staple resection line to make the gastric tube and for esophageal resection. Tumor present at gastroesophageal junction.
Thoracic part
The patient is repositioned in right side-up left lateral decubitus position with double lumen endotracheal tube. Through posterolateral thoracotomy or five-port thoracoscopic approach (Fig. 1), the mobilization of esophagus is done, including the mediastinal lymph nodes from hiatus to carina. Great care is taken for ligation of thoracic duct. The esophagus is divided with linear GIA stapler (Endo GIA Reinforced Reload with Tri-Staple Technology 45 mm, 3.5 mm staple size; Covidien) 1–2 cm above the azygos vein and at least 10 cm proximal to the tumor. Extra 1–2 cm of esophageal stump above the staple line is dissected and freed for anastomosis.
Anastomosis
In thoracoscopic cases, the working port in mid-axillary line is enlarged to 6 cm (Fig. 1) with Alexis™ small wound protector (Applied Medical Resources Corporation, Rancho Santa Margarita, CA). The specimen is retrieved, which also drags the gastric tube up into the chest. Care is taken to maintain the orientation of the gastric conduit. The division of the specimen is completed and is opened on the back table to make sure the margins are clear. If needed, a frozen section is obtained.
Figure 3 shows the identified proposed site of anastomosis. About 3 cm proximal to the proposed site, we place silk marking sutures. The marking stitches help maintain the orientation of the conduit and prevent any twisting at the time of firing of stapler. These stitches also mark the place where the remnant is stapled off.
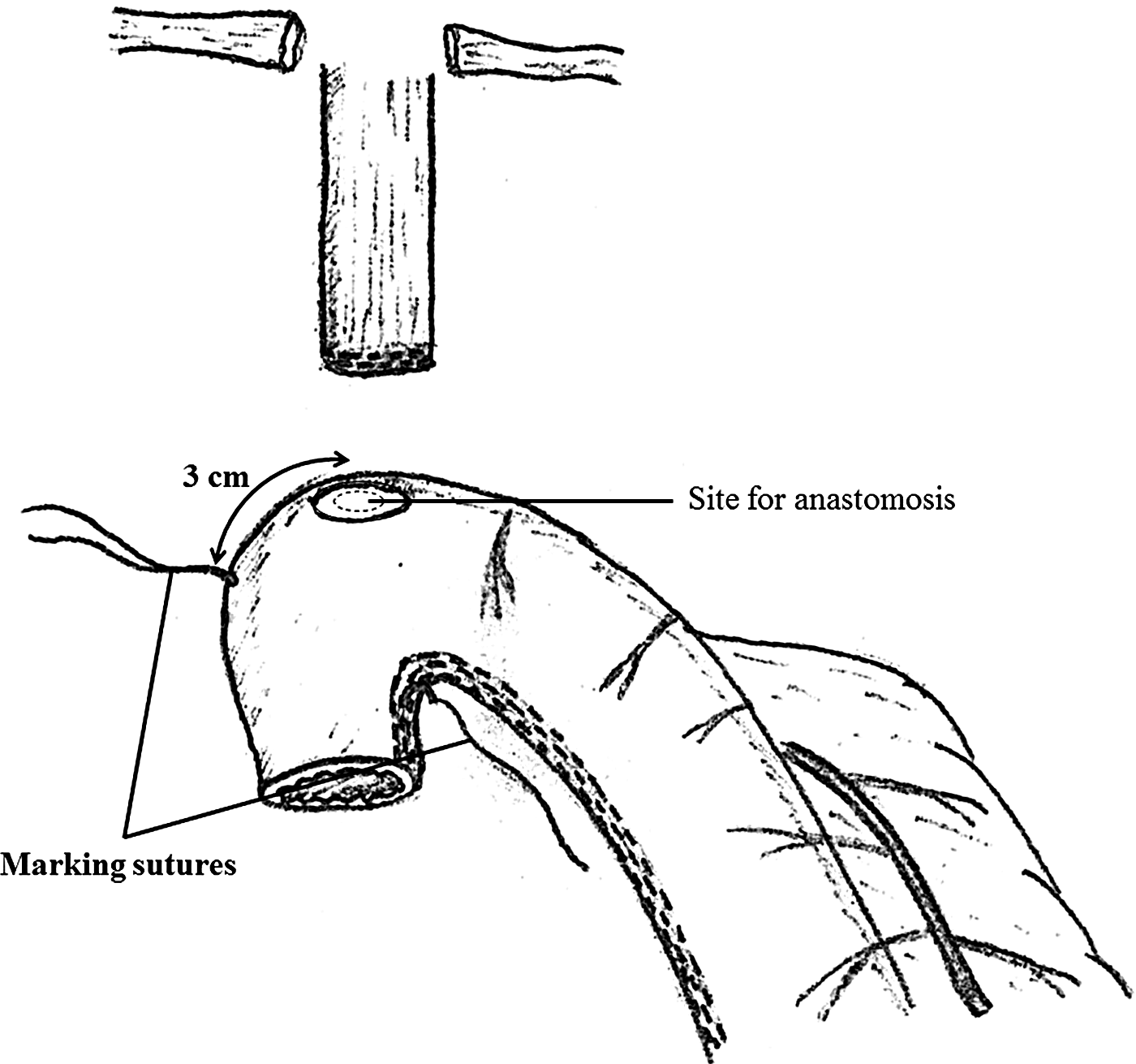
Placement of marking sutures relative to selected site of anastomosis helps in maintaining orientation and determining the position for stapling off the gastric tube.
OrVil™ (Covidien) is an Anvil assembly mounted on the 90 cm PVC delivery tube secured with suture. This helps in delivery of anvil of EEA circular stapler transorally. We use a 25F EEA stapler (DST Series™ EEA™ 25 mm Stapler, 4.8 mm staple size; Covidien) for the purpose of anastomosis. A small enterotomy is made at the tip of the esophageal stump to bring out anvil through it (Fig. 4). The EEA stapler is threaded in the retrograde manner and needle extended 3 cm proximal to the marking stitches at the proposed anastomotic site (Fig. 4). The stapler is engaged with the anvil (Fig. 5). The marking sutures are put under traction to maintain orientation. The stapler is appropriately tightened, fired, and then removed. The two “doughnuts” are examined after removal of the stapler. The proximal “doughnut” is sent as the final esophageal margin. Using previously placed marking stitches as the guide, the redundant gastric conduit is stapled off (Fig. 6).
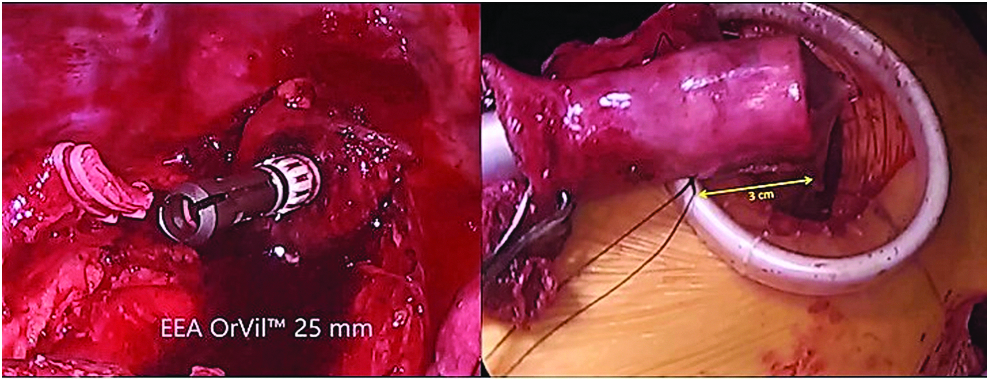
Orvil is brought out of the esophageal stump and EEA stapler threaded in retrograde manner. EEA, end-to-end anastomosis.

Figure showing the technique of anastomosis. Traction on marking sutures helps maintain orientation.

The proximal gastric stump is stapled off using a linear GIA stapler at marking sutures.
The patency of the anastomosis and presence of anastomotic leak are checked through intraoperative endoscopy. The conduit is inflated and submerged in water to ensure water tightness. Nasogastric tube is placed with endoscopic guidance. A piece of omentum from the greater curvature is secured around the anastomosis with 2-0 absorbable suture. A 19 mm Blake drain parallel to the conduit and a 32F chest tube over the diaphragmatic recess are placed.
Nasogastric tube is kept in place till the return of gastrointestinal function. We routinely check for the integrity of anastomosis on postoperative day 6–7 before initiating oral intake (or earlier if clinically indicated) by transnasal endoscopy or contrast esophagogram using water-soluble contrast.
Statistical analysis
Continuous variables were reported as means or medians with range. Independent sample t-test or Mann–Whitney U-test was used to compare group means in univariable analysis. Medians for skewed data were compared using Mann–Whitney U-test. Bootstrapping was used to achieve normal distribution. Categorical variables were reported as number and proportion (%) and Pearson's χ2 (chi-square) test was used to compare groups in univariable analysis. Fisher's exact test was used when the numerator was five or less. Univariable analyses were performed to determine associations of clinical variables with overall anastomotic leak as endpoint. A value of P ≤ .05 was considered significant. All tests have only been analyzed by referring to cases without missing values (complete case analysis). All analyses were performed using SPSS®, version 22.0 (IBM® corporation).
Results
A total of 75 patients had Ivor Lewis esophagectomy with intrathoracic anastomosis using EEA circular stapler and constitute the study cohort. They were divided into three sequential cohorts of 25 patients each as shown in Table 2. The groups did not differ with respect to age, sex distribution, or BMI (Age: 63.7 years versus 66.7 years versus 64.4 years; male: female = 22:3 for all three groups; BMI: 31.4 Kg/m2 versus 29.1 Kg/m2 versus 28.9 Kg/m2; P > .05 for all). Sixty-seven patients (89%) were operated for adenocarcinoma of distal esophagus/gastroesophageal junction (GEJ), five patients (7%) for benign esophageal diseases, while three patients (4%) were operated for squamous cell carcinoma of lower esophagus.
P > .05 for all parameters.
BMI, body mass index; F, female; M, male.
Out of the 75 cases, 58 cases were done laparoscopically and the rest 17 cases done by open approach included 8 conversions from laparoscopy to laparotomy [thoracoscopic 56 cases, thoracotomy 19, which included 11 conversions]. One patient was converted to open hand-sewn anastomosis in Group A due to intraoperative stapler malfunction. The rate of conversion decreased from Groups A to C (21% versus 19% versus 9%, respectively). There was no statistically significant difference found between the three groups with respect to intraoperative blood loss (515 mL versus 333 mL versus 558 mL, respectively, P = .58) and operative time (383 minutes versus 375 minutes versus 356 minutes, P = .36). Median hospital stay decreased significantly over time [16 days (range 9–92 days) versus 15 days (range 8–39 days) versus 11 days (range 7–62 days), respectively; P = .001 for A versus C, P = .026 for B versus C, P > .05 for A versus B]. There was also a trend of decrease in median ICU stay over time [4 days (range 2–54 days) versus 3 days (2–27 days) versus 2 days (1–62 days) respectively; P = .005 for A versus C, P = .011 for B versus C, P > .05 for A versus B] (Table 3).
P-value not significant for all other parameters.
One patient was converted to open hand-sewn anastomosis due to intraoperative stapler malfunction.
P < .05 for hospital stay between Group A versus C and B versus C.
VATS, video-assisted thoracoscopic surgery.
Perioperative morbidity of Clavien-Dindo Grade 2 or higher was seen in 60% patients each in Groups A and B. Morbidity was lower at 40% in the last cohort (P = .03). There were two perioperative mortalities (2.67%), one each in Groups A and C.
According to ECCG classification (type 2 or above), 10 patients had anastomotic leak in the postoperative period requiring intervention (Table 4). Majority of anastomotic leaks occurred in the first cohort [Group A = 8 (32%), Group B = 1 (4%), Group C = 1 (4%); P = .004]. One patient underwent re-exploration and revision of anastomosis (Group C). Three patients were managed by repeated endoscopic washes, four patients required endoscopic stenting along with endoscopic washes, while two patients required transnasal wound VAC therapy. The mean hospital stay and ICU stay for the patients with anastomotic leak in Group A were 38 and 16 days, respectively. The hospital stay for the patient with anastomotic leak Groups B and C were 32 and 22 days and ICU stay were 4 and 2 days, respectively. There were two in-hospital/30-day mortalities (2.7%), including one mortality due to anastomotic leak, which was in the first cohort.
P = .004 for AL between Groups A and B and Groups A and C.
AL, anastomotic leak; ES, endoscopic stenting; EW, endoscopic washes; VAC, transnasal wound VAC therapy.
Discussion
Ivor Lewis esophagectomy, named after the surgeon who first described it in 1946 at Royal college of Surgeons, 10 proved superior to the other procedures because of its better oncologic outcome and remains the mainstay for treatment for esophageal cancers. It gives an excellent visualization of the surgical field and helps in adequate exposure for two-field lymphadenectomy. It was classically a 2-day procedure, >1 week apart, which was combined into two procedures done at the same time. Subsequently, in view of the morbidity associated with thoracotomy and intrathoracic anastomotic leak, transhiatal and McKeown approaches gained popularity. These approaches are, however, associated with higher rates of anastomotic leak and recurrent laryngeal nerve injury. 4 With increasing incidence of distal esophageal carcinoma, Ivor Lewis esophagectomy has shown a resurgence in popularity.
A minimally invasive approach in the form of laparoscopic thoracoscopic esophagectomy is associated with significantly better perioperative outcomes. However, hand-sewn anastomosis done thoracoscopically is time-consuming and challenging. Hence, advent of minimally invasive esophagectomy necessitated the incorporation of stapled anastomotic techniques especially for intrathoracic anastomosis. Lower anastomotic leak rate and recurrent laryngeal nerve injury associated with this procedure have been reported. 11
The anastomotic leak is the Achilles heel of the esophageal resection with incidence as high as 53% reported in literature.12–14 Mediastinal contamination following anastomotic leak is a dreaded complication. There is a 14-fold increase in perioperative mortality in patients with anastomotic leak after esophagectomy, 15 although the incidence, morbidity, and mortality associated with anastomotic complications have decreased over time. Refinement of anastomotic techniques and surgeon's expertise, rather than the choice of conduit, approach, or route of reconstruction, have been proposed to be predictive of leak. 14
Harustiak et al. studied stapled versus hand-sewn anastomosis in 415 esophageal resections and concluded that the stapled technique gave lower overall anastomotic leak and stricture rate. 6 However, the overall morbidity, in-hospital mortality, and length of hospital stay were not affected by the anastomotic technique. Orringer et al. observed a significantly higher leak rate with hand-sewn anastomosis (15%) versus stapled anastomosis (2.7%). 16 Fok et al. compared the circular stapled anastomosis with single-layered continuous hand-sewn anastomosis in 580 patients and concluded that stapled anastomosis had slightly better leak rates. 17 Authors believe that stapled anastomosis, in hands of an expert surgeon, is more reliable than hand-sewn anastomosis. The triple-stapled technique is widely used for esophagogastric anastomosis; however, it is technically difficult and is also associated with significant anastomotic leak. 18
Although the technique is similar to the one described by Luketich and colleagues, 7 we believe that these further little modifications with the addition of the orienting stitches 3 cm distal to the proposed site of anastomosis allow a safer anastomosis with decreased leak rate because (1) they help orient the gastric conduit easily and (2) prevent firing the final stapler too close to the previous staple line, which otherwise increases the chances of anastomotic leak, at least in our earlier experience. We would anticipate that new surgeons using this technique will avoid either anastomotic leak by stapling too close or a redundant conduit beyond the anastomosis.
We noticed that, in our early experience, the leak rate was high with the stapled anastomosis. Over time, we have made modifications to our technique. This has significantly brought down our leak rate. There was higher conversion rate in Groups A and B compared to the third group, however, the leak rate decreased substantially between Group A and B, which reflects that the improvement in anastomotic leak rate is a function of anastomotic technique and surgeon's experience rather than of conversion per se. Through this article, we have described the simplified anastomotic technique in detail and hope that surgeons who either currently have problems with anastomosis and/or are starting new with anastomosis can avoid further high rates of morbidity by adopting this simple technique.
Limitations
This is a single-institution nonrandomized study. The data were collected retrospectively from a prospectively maintained database. However, all the operations were done by a single surgeon and postoperative care was consistent in all three cohorts.
Conclusion
With experience and standardization of technique, the anastomotic leak rate can be significantly reduced. We endorse this simplified anastomotic technique for better clinical outcome and lower anastomotic complications.
Acknowledgments
Supervision, Conception of surgical technique: S.K.M.; Design of research study: S.S., S.K.M.; Data acquisition: S.S., A.K., C.B.; Analysis and interpretation: S.S., A.K., S.A., T.M.; Drafting and revisions: S.S., A.K., S.A., T.M., C.B., S.K.M.; Final approval and accountability for all aspects of work: S.S., S.K.M.
Footnotes
Disclosure Statement
No competing financial interests exist.