
Abstract
Abstract
Introduction:
The aim of this study was to evaluate the efficacy of the retroperitoneoscopic one -trocar -assisted pyeloplasty (OTAP) in children of different ages.
Materials and Methods:
Clinical data of all children who underwent OTAP for ureteropelvic junction (UPJ) obstruction at our Institution, between 2006 and 2014, were reviewed by focusing on demographics, surgical management, and outcomes. Data were analyzed by dividing patients into three groups according to age at operation: patients younger than 2 years (group 1), between 2 and 6 years (group 2), and older than 6 years (group 3).
Results:
During the study period, 70 children (50 males) underwent OTAP (45 left and 25 right). A 10-mm ballooned trocar was inserted under the 11–12th rib and pneumoretroperitoneum was induced (12 mmHg pressure). Through an operative scope, the UPJ was carefully mobilized and exteriorized to the skin level to perform conventional Anderson–Hynes dismembered pyeloplasty. Mean age was 48 months (range, 1 month–14 years). Thirty-six patients (mean age 8.8 months) were in G1, 18 patients (mean age 4.2 years) in G2, and 16 patients (mean age 10.2 years) in G3. There were no intraoperative complications. Mean operative time was 137 minutes: 128 minutes (range, 85–213) in G1, 118 minutes (range, 90–215) in G2 (P > .05 versus G1), and 154 minutes (range, 95–215) in G3 (P < .05 versus G1; P < .05 versus G2). Conversion (an extension of the subcostal incision) rate was 27.1%: 16.6% in G1, 22.2% in G2 (P > .05 versus G1), and 56.25% in G3 (P < .05 versus G1; P < .05 versus G2). At a mean follow-up of 29 months (range, 12 months–5 years), recurrence was observed in 3 patients (2 G1, 1 G3).
Conclusions:
Our results show that OTAP is a good alternative in children younger than 6 years. OTAP is more challenging in older children because of the thickness of the abdominal wall and the higher incidence of aberrant crossing vessels.
Introduction
S
In 2001, Lee et al. 10 first described a laparoscopic-assisted pyeloplasty, and in 2004, Farhat et al. 11 reported a three-trocar retroperitoneoscopic-assisted technique. In 2005, Lima et al. described the retroperitoneoscopic one-trocar-assisted pyeloplasty (OTAP).12,13
The aim of this study was to evaluate the efficacy of the OTAP in children of different ages.
Materials and Methods
The clinical charts of all patients treated with OTAP at our institution between 2006 and 2014 were analyzed. Patients' demographics, surgical management, and outcomes were reviewed. Data were analyzed by dividing patients into three groups according to age at operation: patients younger than 2 years (group 1), patients between 2 and 6 years (group 2), and patients older than 6 years (group 3).
Student's t-test quantitative data comparison and chi-square test were adopted for statistical analysis. A P value of <.05 was considered significant.
Technique
With the patients under general anesthesia by orotracheal intubation, a catheter (Nelaton) is introduced to fill the bladder with methylene blue solution and then removed. The patient is placed in flank position. A 15 mm skin incision is made under the 12th rib. The Gerota's fascia is bluntly reached and opened. A 10-mm balloon trocar is inserted and CO2 is insufflated up to a pressure of 12 mmHg. A 10-mm 0° operative scope is inserted. Retroperitoneal dissection to develop the working space is performed under visual control through a peanut inserted into the 5-mm operative channel of the scope. The kidney is mobilized posteriorly. The proximal ureter, ureteropelvic junction (UPJ), and renal pelvis are identified (Fig. 1) and inspected for aberrant crossing vessels (Fig. 2). Needle aspiration of giant hydronephrosis is performed if needed. The UPJ is carefully mobilized, surrounded with a vessel loop inserted through an operative trocar, lifted up, and then exteriorized to the skin level as the telescope and trocar are removed. Conventional Anderson–Hynes dismembered pyeloplasty is then performed using a 6/0 absorbable suture (Fig. 3). A double-J ureteral stent is positioned in an antegrade manner before the completion of anastomosis: the methylene blue back flow proves the correct intravesical position. A final retroperitoneoscopic evaluation is performed to check for the absence of bleeding or twisting of the anastomosis. At the end of the procedure, a perianastomotic drain is left and the port wound is closed. The double-J stent position is further checked by cystoscopy and a bladder catheter (Nelaton) is reinserted. When the UPJ exteriorization is insufficient to perform pyeloplasty, conversion is performed with an adequate enlargement of the incision.
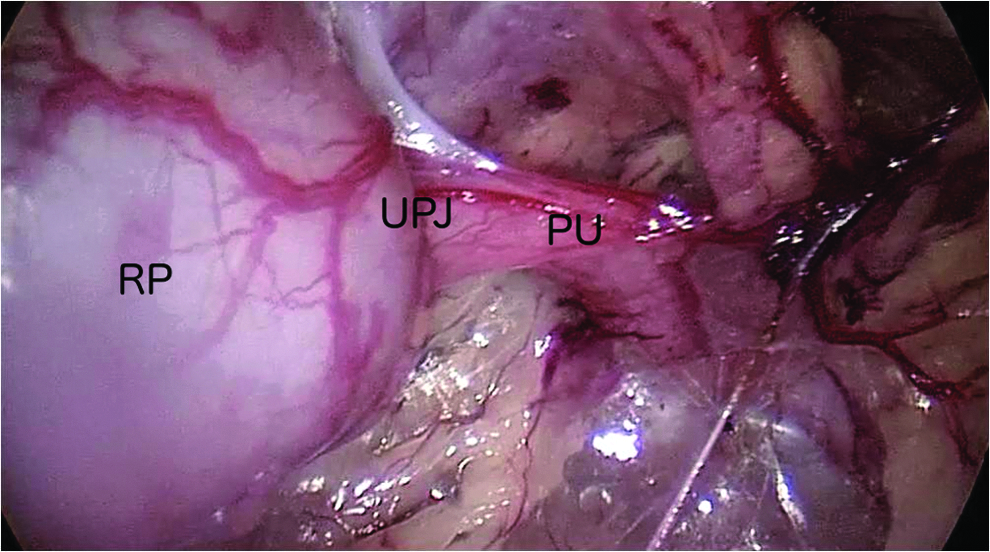
The PU, UPJ, and dilated RP are identified. PU, proximal ureter; RP, renal pelvis; UPJ, ureteropelvic junction.
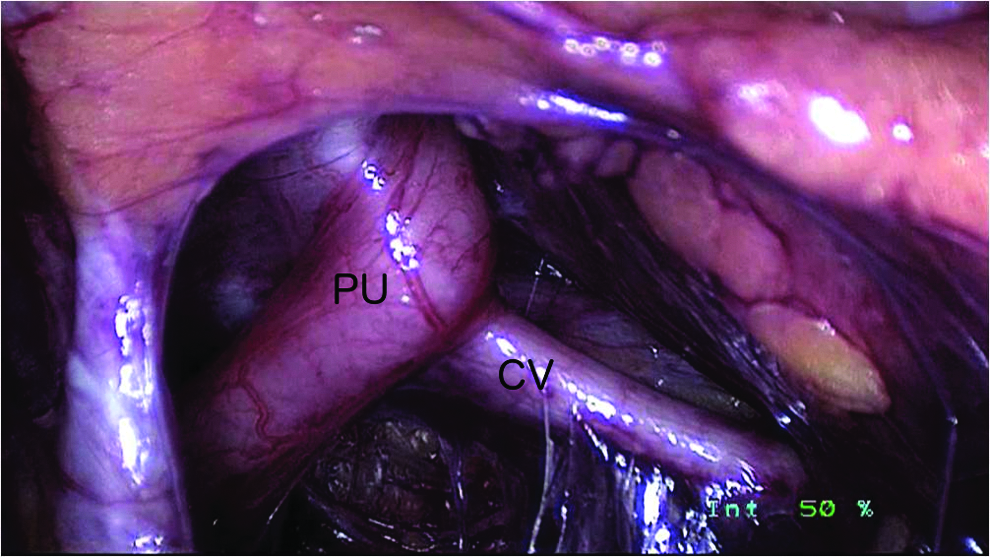
PU and aberrant CV are identified. CV, crossing vessels.

UPJ is lifted up at the skin level with a vessel loop and pyeloplasty is performed outside the abdominal cavity.
Results
During the study period, 70 children (50 males) with UPJO (45 left and 25 right) underwent OTAP. The mean age was 48 months (range, 1 month–14 years). Thirty-six patients (mean age 8.8 months) were in group 1 (G1), 18 patients (mean age 4.2 years) in group 2 (G2), and 16 patients (mean age 10.2 years) in group 3 (G3) (Table 1). The diagnosis and surgical indication were established based on history, physical examination, renal ultrasonography (US), and mercaptoacetyltriglycine renal scintigraphy (MAG3) in all cases. In 12 patients, magnetic resonance urography was performed because of suspicion of aberrant polar vessels or evidence of renal developmental anomalies at US. OTAP was performed in children with UPJO, without exclusion criteria.
There were no intraoperative complications. Mean operative time, including the final cystoscopy, was 137 minutes (range, 85–215): 128 minutes (range, 85–213) in G1, 118 minutes (range, 90–195) in G 2 (P > .05 versus G1), and 154 minutes (range, 95–215) in G3 (P < .05 versus G1; P < .05 versus G2). The overall conversion rate was 27.1% (19 patients): 16.6% (6 patients) in G1, 22.2% (4 patients) in G2 (P > .05 versus G1), and 56.25% (9 patients) in G3 (P < .05 versus G1; P < .05 versus G2).
In most cases, conversion was just as a small extension of incision (up to 3 cm in younger children) with a minimal muscles splitting. In G1, 5 patients (14.2%) had aberrant crossing vessels and 2 (5.5%) had horseshoe kidney. In G2, 4 patients (22.2%) had aberrant crossing vessel and 1 patient (5.5%) had kidney stones. In G3, 8 patients (47%) had aberrant crossing vessels, 1 (6.5%) had ectopic iliac kidney, and 1 (6.5%) had horseshoe kidney (Table 2). Mean hospital stay was 3 (range, 2–4) days in all groups. All patients performed renal scintigraphy MAG3 between 6 and 12 months after operation. At a mean follow-up of 29 months (range, 12 months–5 years), 3 (4.3%) recurrences were observed: 2 (5.4%) in G1 (1 giant hydronephrosis, Fig. 4) and 1 (5.9%) in G3.
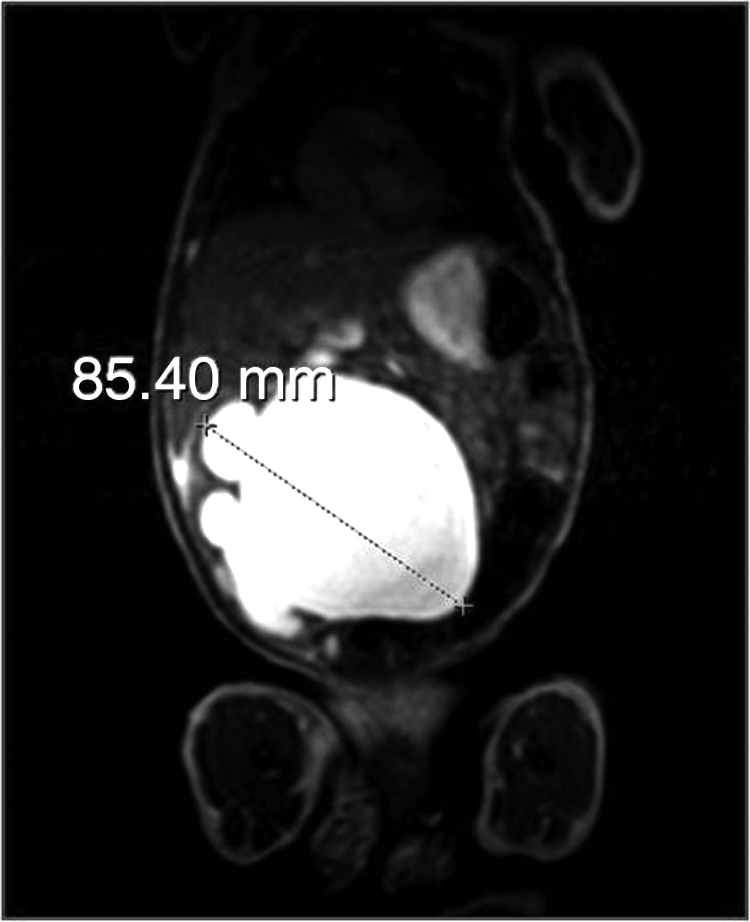
Magnetic resonance image showing a giant right hydronephrosis in an 8-month-old boy who had recurrence.
Discussion
UPJO is the most common cause of hydronephrosis in newborns, toddlers, and adolescents, and open dismembered pyeloplasty has been considered the gold standard since it was described by Anderson and Hynes in 1949 for the treatment of retrocaval ureter. 1 A success rate > 90% has been reported. 4 Laparoscopic dismembered pyeloplasty was first described by Tan in 1999. 8 Nowadays transperitoneal or retroperitoneal laparoscopic pyeloplasty is commonly performed in many pediatric urology centers with excellent results.2–8 However, the transperitoneal approach requires to separate the colon from the Gerota's fascia or to reach the right UPJ through the mesocolon and to perform a watertight suture to avoid intraperitoneal urine leakage. Retroperitoneoscopy is considered a more direct and appropriate approach but offers a minimal working space to make suture and knots, especially in younger children. For these reasons, the retroperitoneoscopic pyeloplasty requires a longer learning curve and is limited to well-trained surgeons. 5
The use of robot, in both transperitoneal and retroperitoneal approaches, may diminish such limitations, requiring lesser laparoscopic skill with a quicker learning curve. However, it has not gained adequate widespread use in children because it is still very expensive and there are also concerns about the use of larger trocars in infants.
Since its first description, 12 OTAP has been considered an adequate alternative because it combines the advantages of minimal invasive laparoscopic technique with those of traditional open surgery with the possibility to perform an handmade anastomosis outside the abdominal cavity after retroperitoneoscopic mobilization of UPJ. In fact it is possible to identify the UPJ easily, avoiding the difficulty to perform intracorporeal sutures related to the minimal working space of retroperitoneal cavity. Moreover in our experience, it warrants good cosmetic result also in case of conversion, which was just as a minimal extension of incision, especially in younger children, even in cases of aberrant crossing vessels or kidney anomalies. In older children, as the UPJ was already identified and mobilized by retroperitoneoscopy, conversion usually required an incision smaller than a standard lumbotomic approach, with a minimal muscles splitting. Moreover, Lima12,13 reported the feasibility of OTAP also in cases of UPJO secondary to aberrant crossing vessels.
Considering our previous experience with one-trocar surgery,14,15 after the description of OTAP we started this approach to the UPJO, reporting our preliminary experience in 2011. 15 We noticed how this technique was particularly useful in younger children and we considered the possibility of evaluating the results by dividing patients into different age groups.
Our study first compared OTAP results related to the age at operation.
Our results emphasize how the OTAP technique is especially useful in children under 6 years of age, without aberrant crossing vessels or kidney anomalies. In fact in our series, we observed a higher conversion rate in group 3 (patients older than 6 years) than younger patients enrolled in groups 1 and 2 with statistical significance. We observed that conversion was also related to kidney anomalies and aberrant crossing vessels that were more frequent in older children. Moreover, we observed only 3 recurrences at a mean follow-up of 48 months.
Furthermore, OTAP allows to perform the surgical procedure in a shorter time than other minimally invasive techniques, especially in younger patients. In fact, in our series, the mean operative time was 127 minutes in children under 2 years, and 107 minutes in children between 2 and 6 years, whereas it was significantly higher (154 minutes) in children older than 6 years. Sweeney et al. 16 reported a mean time of 254 minutes for the laparoscopic transperitoneal approach and Blanc et al. in 2013 17 reported a mean time of 185 minutes for the retroperitoneal three-trocar technique. For the transperitoneal robotic pyeloplasty, Franco et al. 18 reported a mean operative time of 223 minutes. Olsen et al. 19 performed the retroperitoneal robotics technique with a mean operative time of 144 minutes. More recently, Bansal et al. 20 reported a median operative time of 115 minutes for the transperitoneal robotics pyeloplasty in 9 infants. Our results are similar to those reported for other OTAP series.21–24
The technical difficulties that we observed, also in agreement with previous experiences, 21 were related to the thickness of abdominal wall in older children and to the occurrence of aberrant crossing vessels and renal developmental anomalies as horseshoe or ectopic kidney that made the UPJ mobilization difficult.
Conclusions
Our results show that OTAP is a good alternative in children younger than 6 years without renal developmental anomalies and aberrant crossing vessels. OTAP is more challenging in children older than 6 years because of the thickness of the abdominal wall and the higher incidence of aberrant crossing vessels. Future prospective randomized studies will be necessary to determine the gold standard of minimally invasive technique for the UPJO treatment in children.
Footnotes
Disclosure Statement
No competing financial interests exist.