
Abstract
Abstract
Background:
Caudate lobe is located in the deep dorsal area of the liver between the portal triad and the inferior vena cava (IVC). Torrential bleeding can occur from the IVC and short hepatic veins during dissection. Isolated total caudate lobe resection is still rare and technically demanding. We herein present a video on the technical aspect of laparoscopic total caudate lobectomy.
Method:
A 61-year-old woman was admitted for recurrent hepatocellular carcinoma detected on imaging. She had history of multifocal hepatocellular carcinoma in July 2015 and underwent open cholecystectomy, segment 6 and segment 8 tumorectomy. Ten months later, the computed tomography scan and magnetic resonance imaging showed a 1 cm arterial enhancing lesion in segment I (S1) with no other foci of recurrence. Laparoscopic total caudate lobectomy was contemplated.
Results:
The operative time was 270 minutes. The intraoperative blood loss was 200 mL and blood transfusion was not necessary. The patient was discharged on the fourth postoperative day without any complications.
Conclusion:
This report showed the safety and feasibility of laparoscopic total caudate lobectomy. Nonetheless, it is a technically demanding procedure. It should be performed in carefully selected patients and by experienced hepatobiliary surgeons proficient in laparoscopic liver resection.
Introduction
L
Caudate lobe is located in the deep dorsal area of the liver between the portal triad and the inferior vena cava (IVC), 9 which is difficult to approach even in open surgery. In the literature, there are only a few case reports and small case series on laparoscopic caudate lobectomy,10–17 most of which are on limited resection or combined resection with other lobes.18–20 Isolated total caudate lobe resection is still rare and technically demanding.13,17,20 Herein, we present a case (with video) on the technical aspect of laparoscopic total caudate lobectomy.
Methods
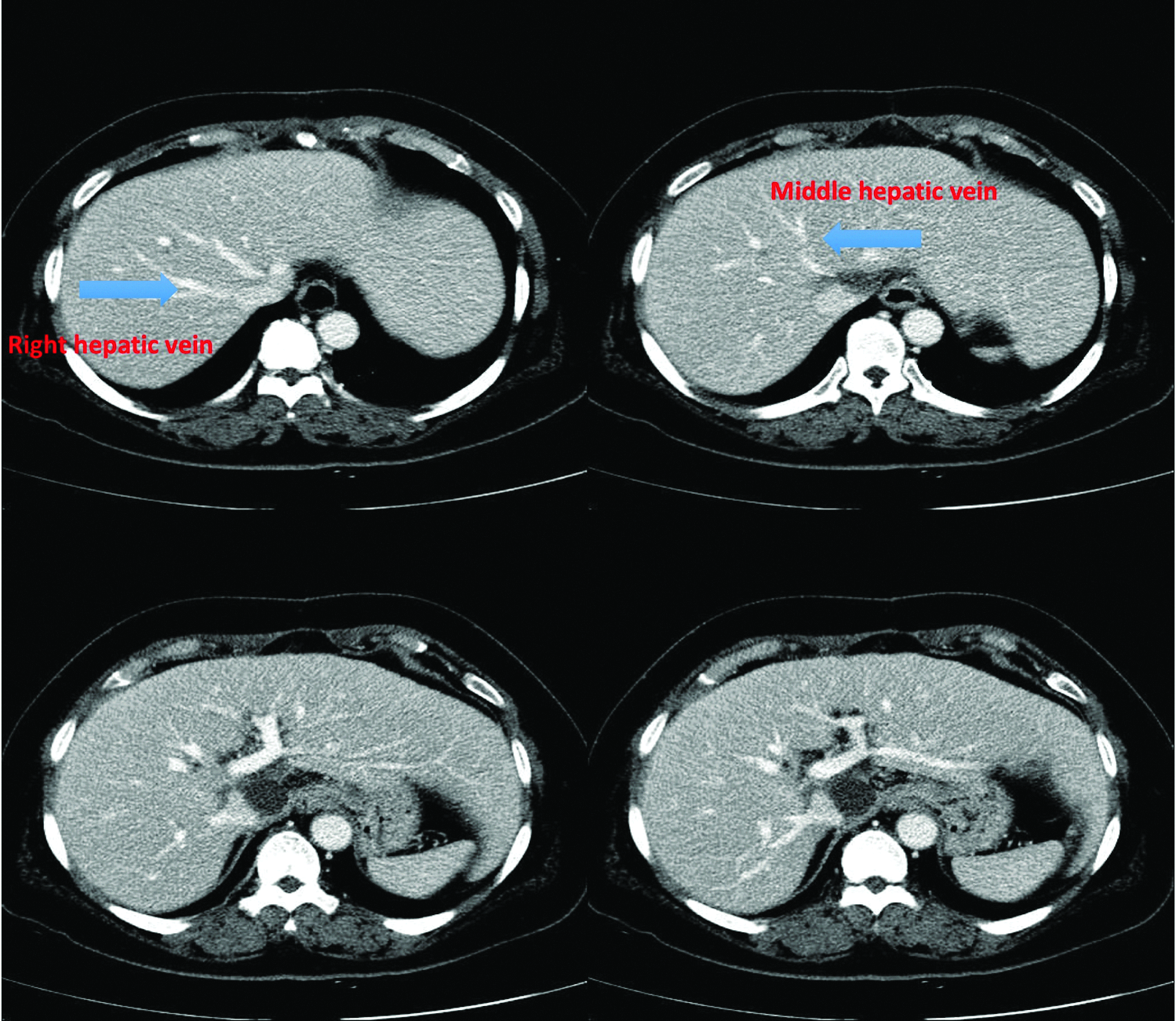
A 61-year-old woman was admitted for recurrent hepatocellular carcinoma detected on imaging study. She was diagnosed to have multifocal hepatocellular carcinoma and underwent open cholecystectomy, segment 6 and segment 8 tumorectomy for these lesions in July 2015. She is a hepatitis B carrier and has a medical history of diabetes mellitus requiring insulin injection. Ten months after the first operation, the computed tomography and magnetic resonance imaging showed a 1 cm arterial enhancing lesion in segment I (S1) with no other foci of recurrence (Fig. 1). Her liver function tests were graded as Child-Pugh class A and the alpha-fetal protein level was normal. With a presumptive diagnosis of recurrent hepatocellular carcinoma, laparoscopic total caudate lobectomy was contemplated.

Preoperative CT scan showing 1 cm arterial enhancing lesion in S1. CT, computed tomography; S1, segment I.
Operative Technique
Under general anesthesia, the patient was placed in the lithotomy position. Pneumoperitoneum was created through the subumbilical port. Four additional 12 mm ports were placed as shown in Figure 2. Moderate adhesion was encountered due to previous hepatic resection and adhesiolysis was performed. The left lateral section was retracted with a fan liver retractor. The gastrohepatic ligament was divided and the Spigelian lobe was mobilized. The right posterior Glissonian pedicle was isolated and temporarily clamped with a bulldog clamp. The counter-demarcation of the caudate process and the right posterior section was marked with electrocautery. Superficial parenchymal transection was performed with Harmonic Scalpel® (Ethicon Endo-surgery, Inc., Cincinnati, OH), and the deeper portion was transected with laparoscopic CUSA® (Valleylab, Boulder, CO). The posterior surface of the caudate lobe was freed from the IVC and the short hepatic veins were controlled with clips and LigaSure® (Covidien). The portal branches to the caudate lobe were ligated and cut. The peripheral part of the right hepatic vein (RHV) was then identified and we continued the dissection of the paracaval portion along the RHV. The caudate process and the paracaval portion were retracted to the left side and the middle hepatic vein was exposed. Bleeding from the middle hepatic vein was encountered and it was readily controlled by sutures. With further parenchymal dissection and division of the portal branches to the Spigelian lobe, the whole caudate lobe was resected. The specimen was then extracted through the umbilical port inside a vinyl bag. After careful hemostasis, a fibrin glue sealant (Greenplast; Green Cross Corp., Seoul, Korea) was applied to the raw surface. A silastic drain was placed after irrigation of the surgical field and the wound was closed in layers (intraoperative photos shown in Fig. 3).

Position of trocar placement.
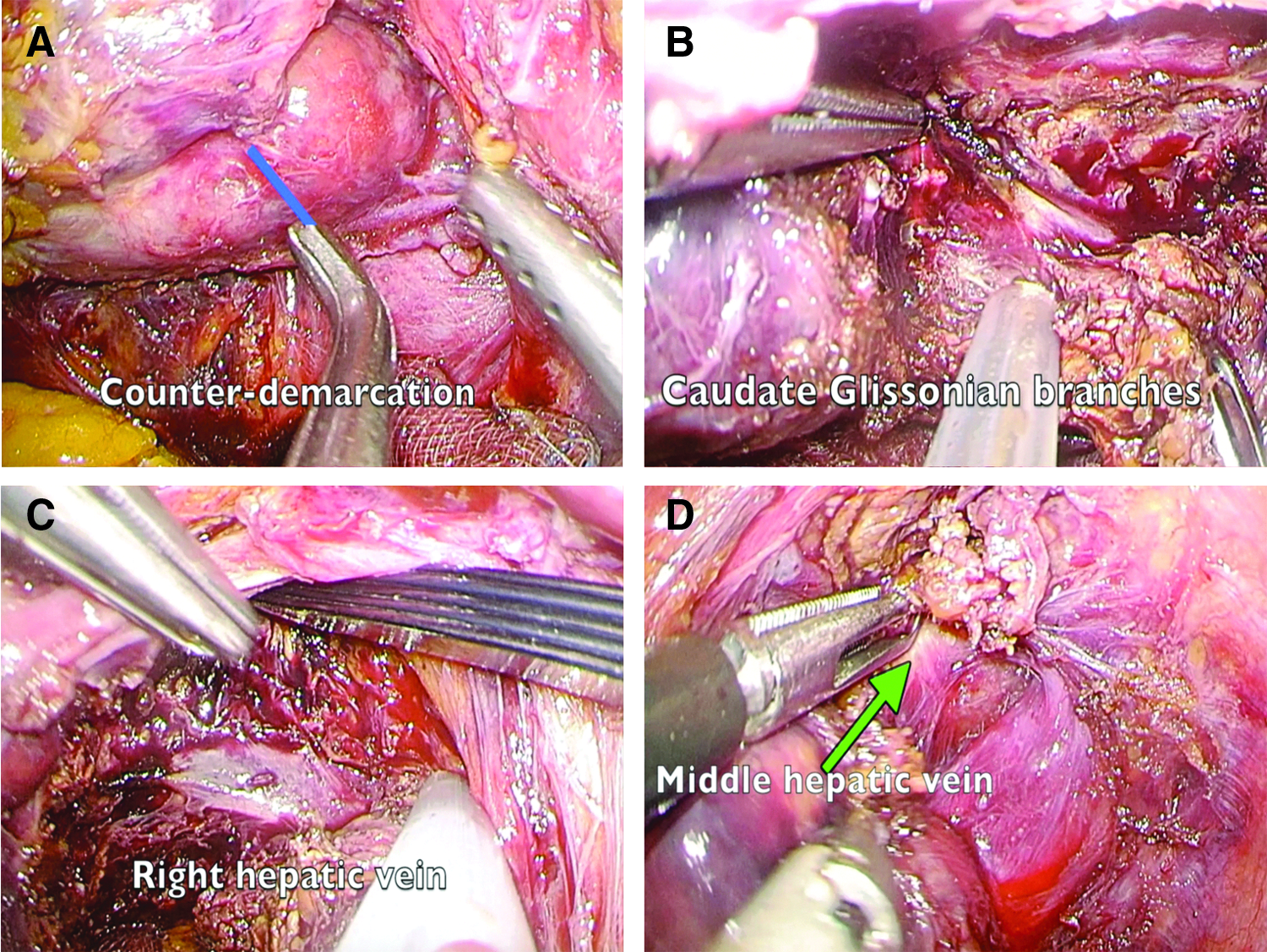
Technical aspects of laparoscopic total caudate lobectomy.
Results
The operative time was 270 minutes. The estimated intraoperative blood loss was 200 mL and blood transfusion was not necessary. On the first postoperative day, the levels of aspartate transaminase (215 IU/L) and alanine transaminase (172 IU/L) were slightly raised and they were normalized on the fourth postoperative day. The pathology showed a 1.6 × 1.5 × 1.2 cm nodular hepatocellular carcinoma with a 3 mm tumor-free resection margin. The patient was discharged on the fourth postoperative day without any complications. The computed tomography scan at 1 month after the operation showed complete removal of the caudate lobe and there was no evidence of recurrence (Fig. 4).
CT scan at 1 month after the operation. The whole caudate lobe between right and middle hepatic vein was resected. CT, computed tomography.
Discussion
Although there is still controversy on the superiority of anatomical resection over nonanatomical resection for hepatocellular carcinoma,21–25 anatomical resection is still preferred. It follows the oncological principle by removing all the liver parenchyma that is potentially involved by tumor spreading into the segmental portal venous branch. Therefore, anatomical total caudate lobectomy was contemplated for our patient.
In fact, comprehensive and precise knowledge of the anatomy of the caudate lobe is paramount to the safe dissection around the Glissonian pedicles and major hepatic veins. 26 Laparoscopic resection offers a clear and magnified view of the area from the caudal approach. 27 With tactful retraction and meticulous dissection, the portal pedicles and hepatic vein branches can be easily identified and controlled. To mark the boundary of the caudate process, we temporarily clamp the right posterior Glissonian pedicle. The demarcation of the caudate process and right posterior section is determined by the counter-demarcation technique.28,29 For resection of the paracaval portion, we perform meticulous dissection by CUSA and Harmonic Scalpel to show the RHV and the middle hepatic vein. Although bleeding is commonly encountered during dissection close to the major hepatic veins and portal pedicles, it can be readily controlled by application of sutures.
Nonetheless, with the high technical demand and complexity of the procedure, we believe that it is safe and feasible only in selected patients and by experienced hepatobiliary surgeons proficient in laparoscopic liver resection.
Conclusion
This report showed the safety and feasibility of laparoscopic total caudate lobectomy. Nonetheless, it is a technically demanding procedure. It should be performed in carefully selected patients and by experienced hepatobiliary surgeons proficient in laparoscopic liver resection.
Footnotes
Disclosure Statement
No competing financial interests exist.