
Abstract
Abstract
Introduction:
Narrow working space is a major problem to overcome during retroperitoneoscopic ureterolithotomy. We evaluated initial 5 years experience of retroperitoneoscopic ureterolithotomy for large impacted upper ureteral calculi.
Patients and Methods:
Between January 2011 and December 2015, a total of 37 consecutive patients were evaluated. A 12-mm camera port at middle of midaxillary line and two 5-mm working ports in posterior axillary line were created. The stone was extracted through the site of camera trocar. A Double-J catheter (DJC) was placed antegradely by four steps (elevating of the proximal shaft, introducing the end of curl, advancing, and twisting) during retroperitoneoscopic ureterolithotomy. A knotless unidirectional barbed suture was applied to the incision site of the ureter in all cases. All patients were followed up at 2 weeks after discharge to remove a DJC and at 6 weeks after discharge to evaluate urinary drainage with intravenous urography.
Results:
The mean ± standard deviation for age (years), body mass index (kg/m2), stone size (mm), and postoperative hospital days were 57.9 ± 13.3, 24.6 ± 4.5, 15.5 ± 4.0, and 3.2 ± 1.2, respectively. Stones were successively removed without critical complications such as ureteral stricture in all cases. Total operation time, the time for placing a DJC, and ureteral suturing time at initial three trials were more than 150 minutes, more than 30 minutes, and about 15 minutes, respectively; however, they were about 60 minutes, less than 10 minutes, and about 5 minutes, respectively, in 25 case experiences.
Conclusions:
Retroperitoneoscopic ureterolithotomy is a safe and excellent alternative for large impacted upper ureter stone. When performing retroperitoneoscopic ureterolithotomy in the narrow space, our step by step methods, including working port creation, DJC placement, and suturing, will be helpful for surgeons to learn the procedure easily.
Introduction
A
Patients and Methods
Patients
Data from 37 consecutive patients who presented with upper ureter stones between January 2011 and December 2015 were evaluated. The study's inclusion criteria should meet the following: 10 (1) an upper ureter stone larger than 10 mm after treatment failure with extracorporeal shock wave lithotripsy (ESWL) and/or retrograde ureteroscopic ureterolithotripsy (RUU), or an upper ureter stone larger than 15 mm; (2) an upper ureter stone located between lower border of the kidney and the common iliac vessel. The study's exclusion criteria were cases with concomitant renal stone(s).
Procedures
The patient was placed in a lateral decubitus position with a slight bend at the level of their umbilicus. A 5% iodine solution was applied to the surgical area, and the surgical drapes were positioned around the surgical site. The camera port was placed in the midaxillary line between the tip of the 12th rib and the iliac crest. To create the retroperitoneal space, a 1.2-cm incision was made at the site of the first port and it was deepened with blunt dissection using Kelly hemostatic forceps until the transversalis fascia was incised. When the surgeon's index finger identified the pararenal fat, a glove finger balloon, which was attached to an 8-Fr Nelaton catheter, was inserted into the area, and the retroperitoneal working space was created by inflating the balloon with 500–600 mL. Once the space was created, a blunt tip trocar (OMST-10BT; Covidien, Mansfield, MA) was inserted and a laparoscope was inserted through the trocar. The second and third port sites were on the posterior axillary line; the former was near the 12th rib, while the latter was near the margin of the iliac crest. Sometimes, needle challenge may help a surgeon to make sure of the position and direction of the third trocar (Fig. 1A–C).

Trocar insertion.
Initially, we tried to identify the base of the surgical plane, that is, the psoas muscle. Then, we opened Gerota's fascia enabling the identification of the ureter medially. Once the position of the stone was confirmed, the ureter was incised longitudinally with a laparoscopic cold knife. In rare cases (n = 2 for 5 years), 360° kinked ureter with severe adhesive change was noted (Fig. 2A, B). In these cases, surgeons can perform ureterolysis easily during retroperitoneoscopic procedure. After a stone retrieval, a hydrophilic guidewire was inserted through second trocar. Then, the guidewire was inserted into the ureter caudally (antegradely) through the incision site of the ureter (Fig. 3A). Subsequently, a DJC was inserted through the guidewire, and the guidewire was removed. In this point, we completed insertion of a DJC with overcoming the proximal curl by several steps—in case of left upper ureter stone, (1) elevating the junction between shaft of DJC and proximal coiling of DJC against the ureter with left dissecting forcep may help right dissecting forcep to insert the end of the upper coiling of DJC into proximal ureter (Fig. 3B); (2) after inserting the end of coiling into the narrow cranial side hole of the incised ureter with right dissecting forcep, left dissecting forcep released DJC and immediately held the middle portion of the coiling (Fig. 3C); (3) gently advancing the left forcep, right forcep released the tip of the coiling and immediately held the proximal portion of the coiling (Fig. 3D); (4) twisting right laparoscopic forcep would help DJC to be straightened and fit into the ureter (Fig. 3E). Then the positioning of DJC was done by watching the scales on the shaft of the catheter. Continuous suture was done using V-Loc™ 90 absorbable suture (CV-15/4-0; Covidien) at ureteral incision site (Fig. 3F). In our institute, we have usually applied 6.0 mg of hyaluronic acid and carboxymethyl cellulose (Guardix-SG®; Hanmi Medicare Co., Ltd, Seoul, Korea) to the dissecting area.
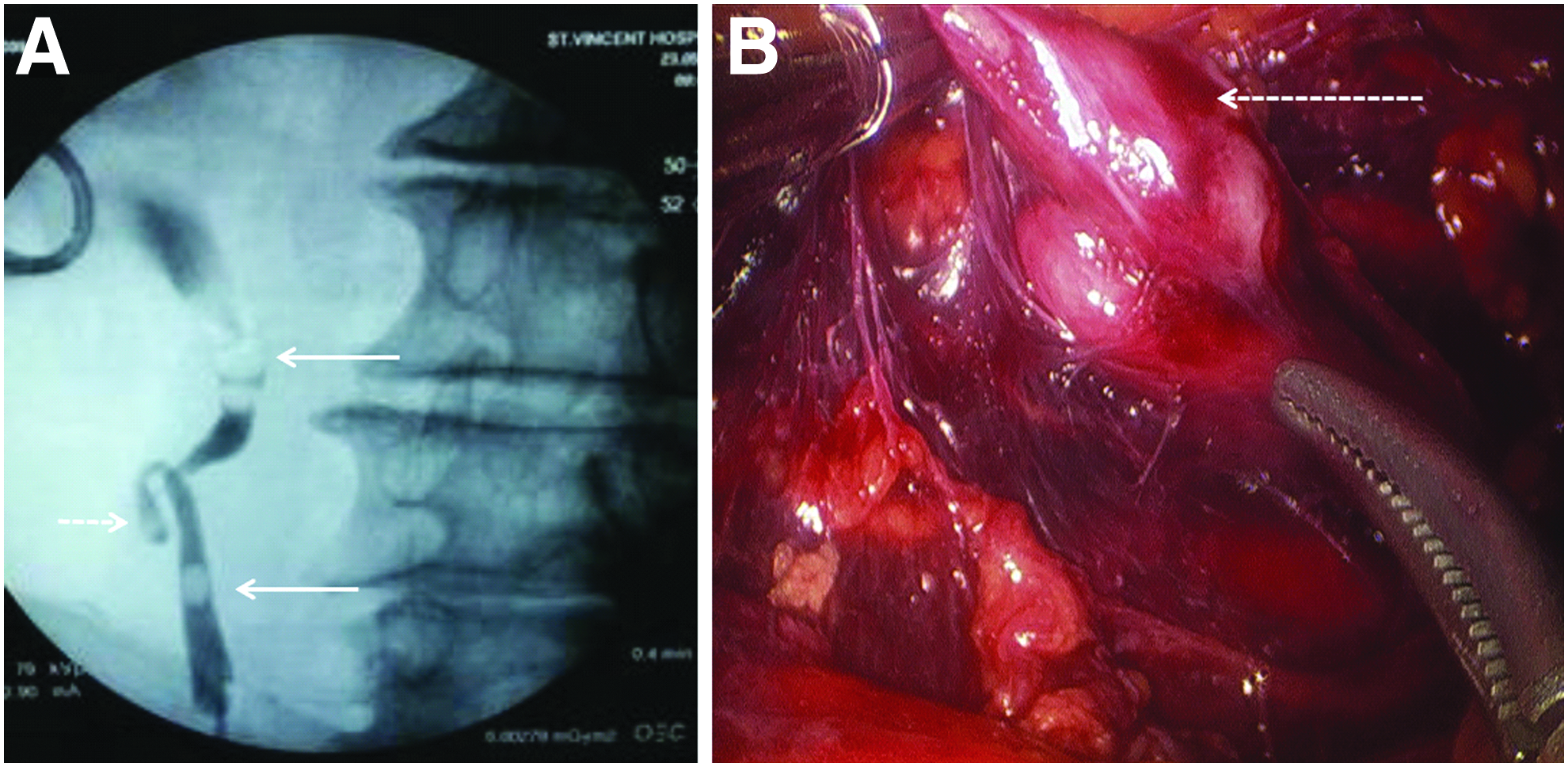
Severe periureteral inflammation with 360° kinked ureter. A 60-year-old man had been presented with right side flank pain with fever. Upper ureteral stone with severe hydronephrosis was diagnosed with computed tomography in emergency room, and percutaneous nephrostomy was done to relieve pain and infection. After all symptoms were subsided, ureteroscopic procedure was tried but failed.
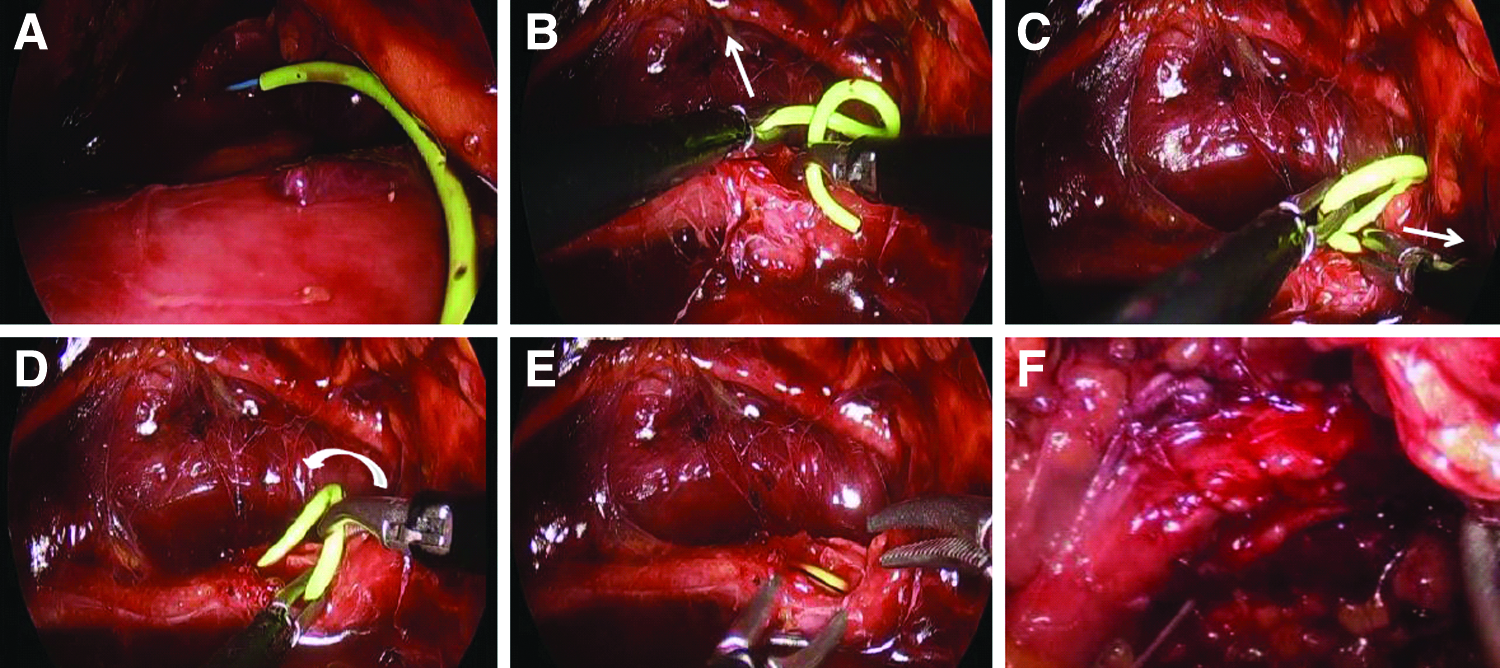
Antegrade placement of a DJC.
A small bag for the stone was introduced through the camera trocar, leaving the thread of the bag outside the camera trocar. Then, the stone was enveloped and the bag was sealed and removed together with the camera trocar. A Jackson-Pratt drain was inserted through the second trocar, leaving its tip to the most dependent area.
All patients were followed up at 2 weeks after discharge to remove a DJC, and at 6 weeks after discharge to evaluate urinary drainage with intravenous urography (Fig. 4A, B).

Preoperative plain X-ray images and follow-up IVU (intravenous urography).
Results
Among 37 patients, 23 patients underwent retroperitoneoscopic ureterolithotomy after failure of ESWL, 2 patients underwent the procedure after failure of approach by RUU in whom severe kinked ureter was identified during the retroperitoneoscopy, and 12 patients having upper ureter stone larger than 15 mm underwent the procedure without other treatments. Twenty-nine were men and 11 were women, and their mean age (years) and mean body mass index (kg/m2) were 57.9 ± 13.3 and 24.6 ± 4.5, respectively. The mean stone size was 15.5 ± 4.0 mm. All operations were successfully completed without stone migration into the renal pelvis. The mean postoperative hospital stay was 3.2 ± 1.2 days (minimum 2 days, maximum 6 days). All patients retained their DJC for about 2 weeks, and they underwent intravenous urographies (in case of chronic kidney disease, nonenhanced computed tomography was performed) 4 weeks after removal of the DJC. There were no critical postoperative complications, such as ureteral stricture or urinary leakage. Baseline demographics and surgical outcomes of 37 patients are presented in Table 1.
These values are presented as mean ± SD (minimum, maximum). The other values were frequencies of relevant variables.
Learning curve should be considered to understand operating time (Fig. 5).
SD, standard deviation.
Taking into account the learning curves, we presented operating time for the cohorts in chronological order (Fig. 5). Total operation time (skin to skin) and the time for placing a DJC at initial three trials were more than 150 minutes and more than 30 minutes, respectively; however, those times were gradually reduced and eventually total operation time reached at 60–70 minutes and DJC placing time reached at 5–10 minutes. Time for ureteral suturing was about 15 minutes at initial three trials and eventually it reached at 5–6 minutes after 25 experiences.
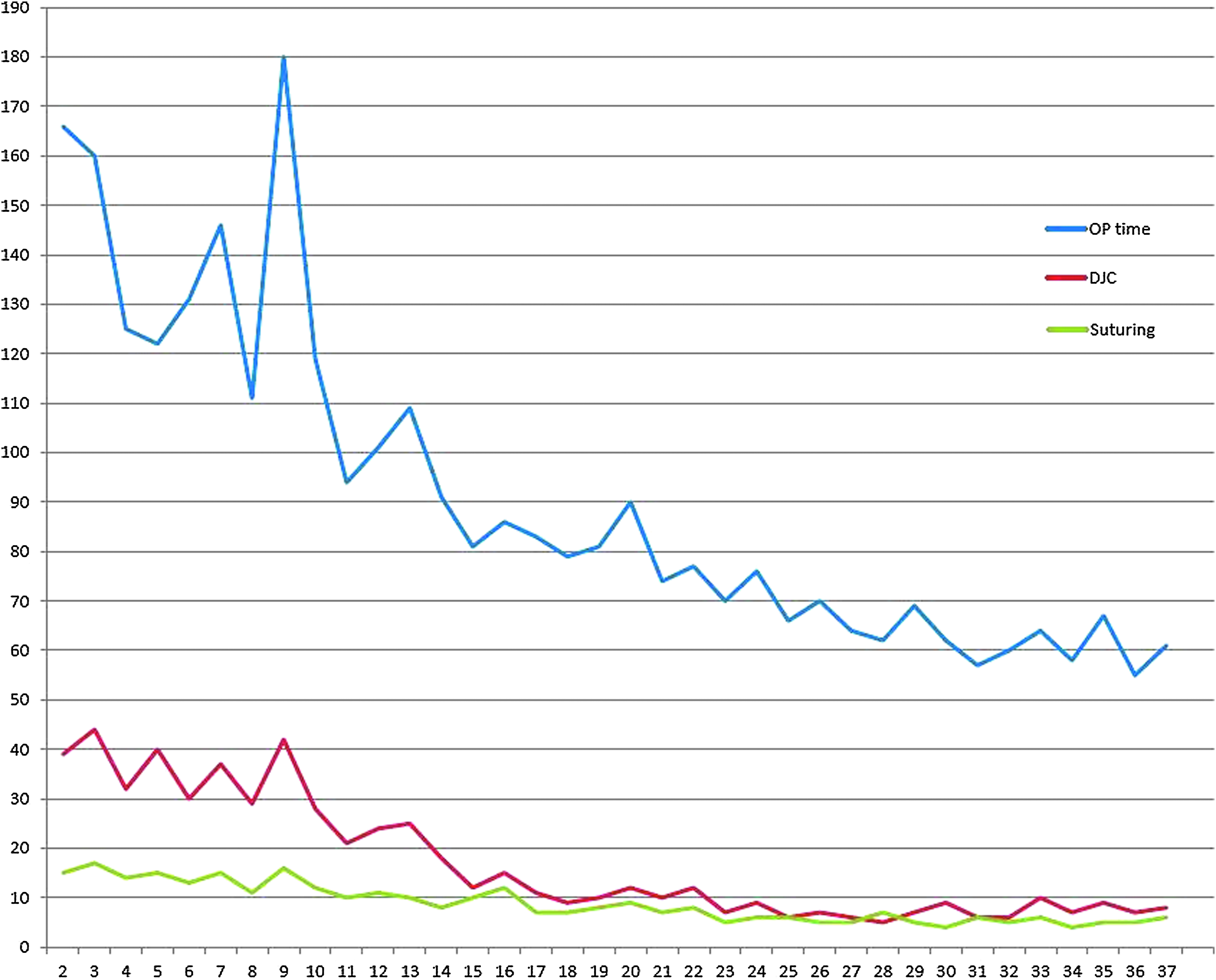
Operating times for the cohorts in chronological order. Total operating time (blue). Total time for antegrade DJC placement (red). Suturing time (green). DJC, Double-J catheter.
Discussion
Although both ESWL and RUU are first-line treatment modalities for upper ureteral calculi, the stone-free rates (SFRs) of ESWL and RUU for upper ureteral stones larger than 10 mm remains at 66%–74% and 70%–80%, respectively.11,12 Stone (fragments) migration to the renal pelvis or calices during RUU is the leading cause of decreased SFR. Flexible ureteroscopy can be used to retrieve a migrated stone. Flexible ureteroscopy is generally known as less invasive treatment than laparoscopic treatment. However, a recent study showed that flexible ureteroscopy was not available in 28 of 114 (24.6%) clinics. 13 Furthermore, retroperitoneal laparoscopic ureterolithotomy showed superior success rate with lower chance of ureteral stricture than ureteroscopy to treat large upper ureter stones.14,15 In addition, 46.5% of patients who underwent flexible ureteroscopy experienced ureteral wall injury resulting from insertion of a ureteral access sheath. 16 Keeley et al. recommended laparoscopic ureterolithotomy as a first line treatment for large upper ureter stone (>15 mm). 10 Therefore, a decision on treatment modalities for large impacted upper ureteral stones should be made after a full informed discussion between patients and physicians because there is no evidence justifying the laparoscopic surgery before ureteroscopic surgery or vice versa for large upper ureter stone. Sometimes, retroperitoneal inflammatory change with severe ureter kinking can be encountered, in which a surgeon may not even reach at the stone with ureteroscopy. This situation may not be overcome by flexible ureteroscopy. In our experiences, we could not reach at a stone site with ureteroscopy, even with flexible ureteroscopy in two cases (ureteroscopic failure), and the procedure was converted into retroperitoneoscopic ureterolithotomy on the spot (Fig. 2), where ureterolysis for almost 360° severe ureteral kinking with adhesive change was easily done.
As described before, retroperitoneoscopic ureterolithotomy has several merits, including “no bowel manipulation,” but the procedure is known for having narrow working space, which is the major reason that makes the procedures difficult. To enhance surgeons' procedure, determining the port site is very important. The vast majority of surgeons who perform retroperitoneoscopic ureterolithotomy make their second and third port sites at anterior and posterior axillary lines.4,8,17–20 There may be no ideal port position in urological laparoscopic procedure, but Yunusa et al. recommended a manipulation angle of 60°. 21 However, for using a port on anterior axillary line in lateral position, an operating surgeon should let his/her one arm abduction and shoulder elevation across the patient. Up to our knowledge, the present study is the first report using two working ports on the posterior axillary line. With these ports, surgeons can operate with comfortable posture during the operation.
From a surgeon's perspective, and particularly from the perspective of those who are less-experienced urologic surgeons, it must be difficult to insert a DJC antegradely during retroperitoneoscopy. Several studies have been published that describe a number of techniques for DJC insertion during retroperitoneoscopy. Nouira et al. performed their initial retroperitoneoscopic ureterolithotomy by inserting a 6.0-Fr open-tip ureteral catheter up to the lower edge of the impacted stone under fluoroscopic guidance before turning the patient into the full lateral position. 22 They advanced a guidewire through the catheter after stone retrieval under laparoscopic vision and the guidewire was exchanged for a DJC. Using a C-arm fluoroscopy is helpful to place a ureteral catheter before lateral positioning of patients for laparoscopy and to confirm whether a DJC is well positioned after laparoscopy. However, this excellent method needs additional procedure before lateral positioning of the patients. Gaur et al. performed an intracorporeal placement of closed-tip DJC that was inserted with a guidewire that was 2 cm longer than the DJC to overcome the difficulty in inserting the coiled tip of DJC. 23 However, a closed-tip DJC is not always available in many institutes. In the present study, the antegrade placement of DJC took more than 30 minutes at initial trials; however, time for antegrade DJC placement eventually reached within 10 minutes (5–10 minutes) during learning periods. We believe that if surgeons become acclimatized to the procedure, methods for placement of DJC during retroperitoneoscopy may not be a matter of concern. However, there is no detail tip for antegrade DJC placement. Our detail description of steps for inserting upper coiling of DJC (elevating the junction between the shaft and the proximal coiling of DJC, introducing the distal end of the proximal coiling into the proximal ureter, advancing the coiling up to the middle of the coiling, and twisting the coiling) must be a useful guidance to novice surgeons.
Recently, knotless unidirectional barbed sutures have been safely used for even reconstructive bowel surgery and bile duct surgery.24,25 To our knowledge, there are no clinical data for the use of barbed sutures during retroperitoneoscopic surgery. Instead, it took 30 minutes for a surgeon in training to apply three to four interrupted ureteral sutures during retroperitoneoscopy, whereas 14 minutes was needed in the transperitoneal approach. 8 In our experiences, it took only about 15 minutes even in initial attempts, and eventually it took about 5 minutes. In our cohort, ureteral stricture was not found in follow-up imaging studies; therefore, knotless unidirectional barbed suture would be an excellent method for suturing during retroperitoneoscopy.
In a recent report with 197 cases, the rates of urine leak and ureteral stricture were 2.5% and 1.0% after retroperitoneoscopic ureterolithotomy. 26 The number of cases may be small for those complications to occur in the present study, but we believe that our methods, including placement of DJC, using knotless barbed sutures, and applying hyaluronic acid and carboxymethyl cellulose around dissecting area, may have contributed in lowering those complications.
Conclusion
Narrow working space is a major concern during retroperitoneoscopic ureterolithotomy. Our surgical tips and techniques, including making two working ports at the posterior axillary line, DJC placement, and suturing method, will help surgeons be more comfortable during the narrow space retroperitoneoscopic ureterolithotomy. In respect to our experiences, retroperitoneoscopic ureterolithotomy is a safe and excellent alternative for large upper ureter stone.
Footnotes
Disclosure Statement
No competing financial interests exist.