
Abstract
Abstract
Background:
Totally extra-peritoneal (TEP) repair of inguinal hernia is now a standard surgical technique. A 12 mm incision in infra-umbilical region for Hasson trocar is must for TEP repair of inguinal hernia. This is the only technique known to laparoscopic surgeons. We have innovated a “555 Technique” for completing Mini TEP repair of inguinal hernia by using all three 5 mm ports.
Methods:
Sixty-one consecutive patients were subjected for TEP repair of inguinal hernia by our innovative “555 Technique” since October 2014. A simple “Manish Retractor” is devised to make extra-peritoneal space with 5 mm trocar. Fifty-nine cases were men and 2 cases were women. The mean age of patients was 44.6 years (range 23–82 years).
Results:
Out of 61 cases, 27 were indirect inguinal hernia (23 unilateral, 4 bilateral), 32 direct inguinal hernia (21 unilateral, 11 bilateral), 1 femoral hernia, and 1 obturator hernia. One patient of indirect inguinal hernia had sliding hernia with sigmoid colon. Sixty cases were successfully operated by “555 Technique.” There was conversion to trans-abdominal pre-peritoneal repair (TAPP) in 1 case. The average time for insertion of 5 mm trocar in preperitoneal space by our technique was 150 seconds. No complications were noted on 6 months follow-up. Small infra-umbilical scar was cosmetically more acceptable to patients.
Conclusion:
“555 Technique” is a feasible option without compromising the principles of TEP repair for inguinal hernia. Innovation of simple “Manish Retractor” is the key in completing Mini TEP repair. This technique is simple, less invasive, less morbid, and cost effective as it avoids dependence over costly Hasson trocar with better cosmetic results.
Background
T
Methods
All patients having inguinal hernia since October 2014 were operated consecutively by “555 Technique.” A written informed consent was taken explaining about the surgical procedure, other available surgical options, probable complications and possibility of conversion to other laparoscopic or open procedure. Patients who were subjected for Mini TEP repair of inguinal hernia by “555 Technique” underwent a thorough preanesthetic checkup and clearance for general anesthesia. Prophylactic antibiotic was given at the time of induction for surgery. Complete reduction of the content of the hernia sac was done after induction if possible.
Sixty-one consecutive patients were subjected for TEP repair of inguinal hernia by our innovative “555 Technique” since October 2014. Fifty-nine cases were men and 2 cases were women. The mean age of patients was 44.6 years (range 23–82 years). All the patients were followed up for the period of 6 months for any hernia recurrence, surgical site infection (SSI), and chronic pain. We have standardized the “555 Technique” of inguinal hernia and the steps are as follows:
Surgical steps of “555 Technique” for mini TEP
Instruments used in “555 Technique” are as follows:
1. Three 5 mm Visiport (Endopath XCEL Bladeless Trocar; Ethicon) (Fig. 1)
2. Two milliliters plastic syringe to make “Manish Retractor”
3. Five millimeters, 0° or 30° telescope
4. Laparoscopic instruments (Maryland dissector, Grasper, Scissor)
5. Silk thread No. 1-0 on needle
6. 15 × 10 cm size, light weight Polypropylene mesh (Ultrapro Mesh; Ethicon)
7. Tacker for mesh fixation
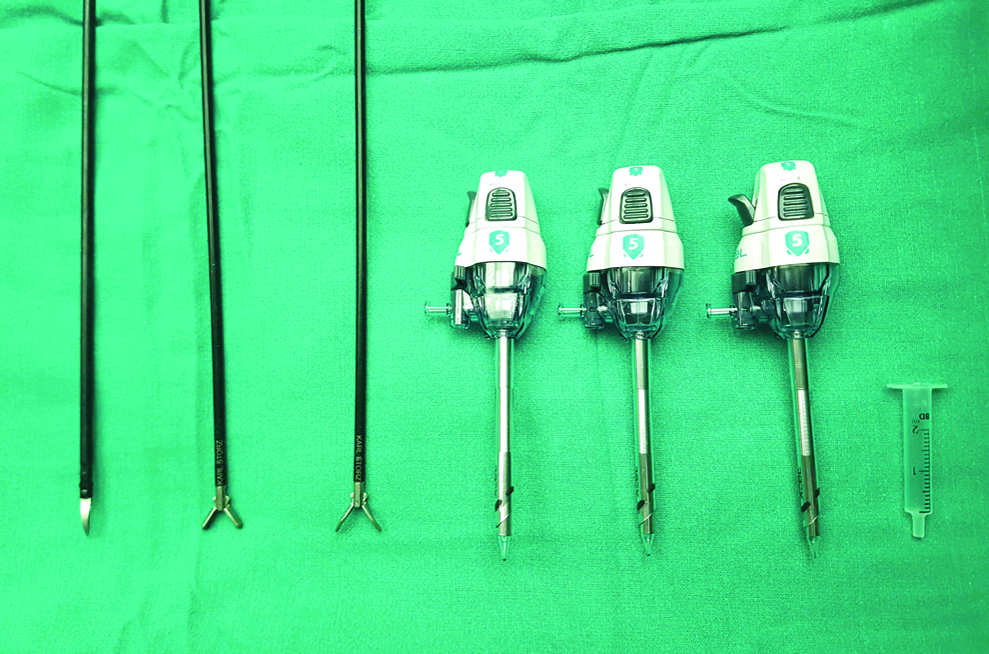
Instruments used for Mini TEP repair of inguinal hernia. TEP, totally extra-peritoneal.
Preparing the “Manish Retractor”
A 2 mL plastic syringe hub is used to make an innovative “Manish Retractor” (Figs. 2 and 3). A 4 cm long retractor is made by dividing 2 mL syringe hub. This 4 cm size syringe hub is further slit along its length with the help of scissor. This simple retractor devise was given the name “Manish Retractor” for easier identity.

A 4 cm long 2 mL plastic syringe hub is cut to make Manish Retractor.

Four centimeters long syringe hub is further slit along its length to make Manish Retractor.
Extra-peritoneal access
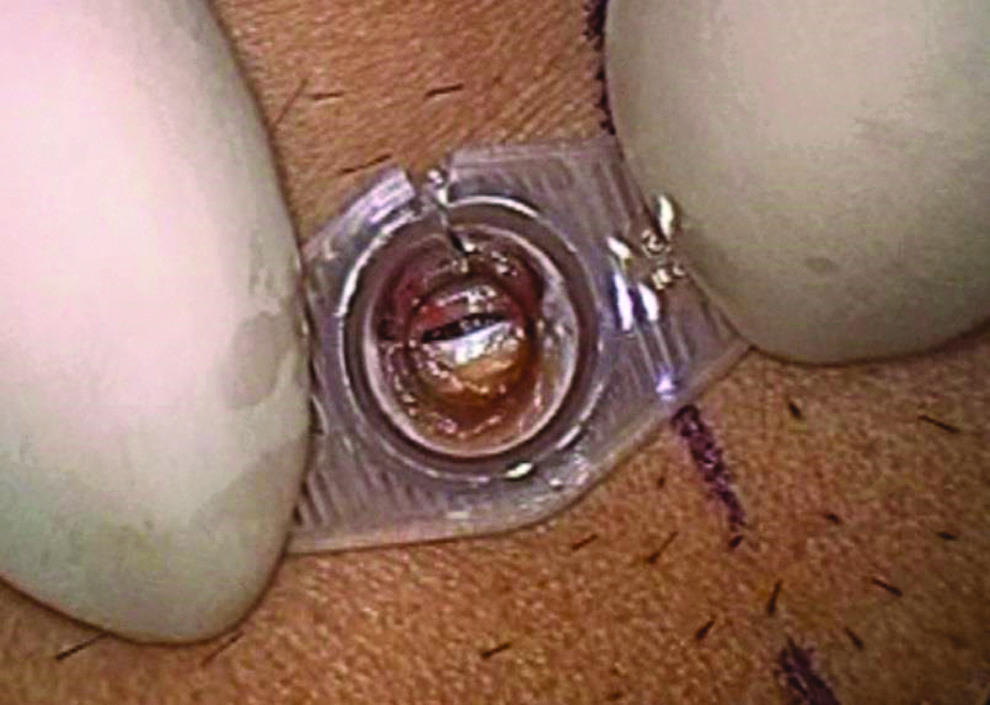
In our technique, a 5 mm incision is made in the infra-umbilical region just lateral to midline (Fig. 4). The incision is then deepened in subcutaneous fat up to the ARS. Manish Retractor made of syringe hub snugly fits in the 5 mm infra-umbilical incision. This retractor displaces the fat outward and clears the view up to the ARS. Suction is used to clear the remaining fat above the rectus sheath. One can easily appreciate the shining ARS at the base once all the subcutaneous fat is cleared by suction (Fig. 5). A 5 mm transverse incision is then made in the ARS with the help of No. 11 blade. A slit appears in the ARS with underlying longitudinal muscle fibers of rectus muscle (Figs. 6 and 7).
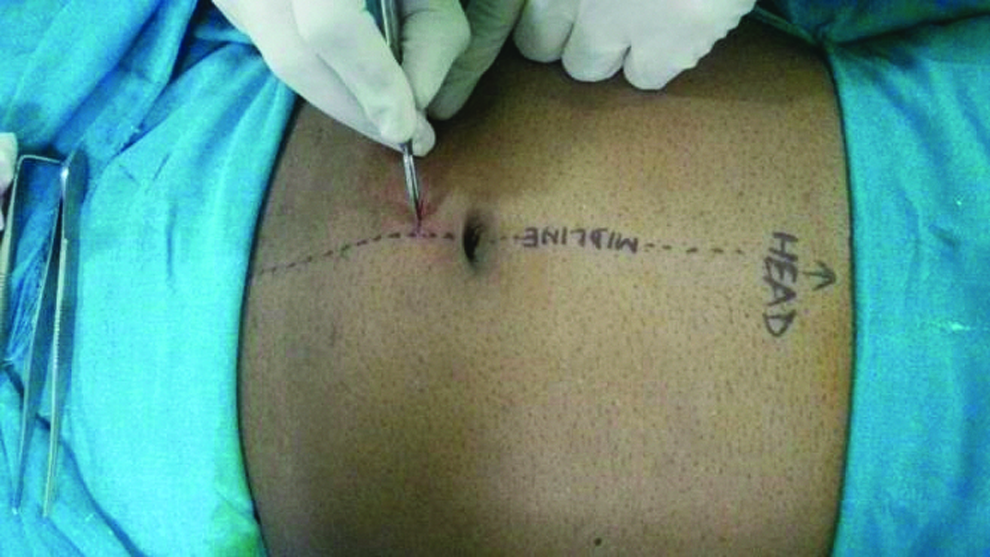
A 5 mm incision in made in the infra-umbilical region just lateral to mid line for first port placement.
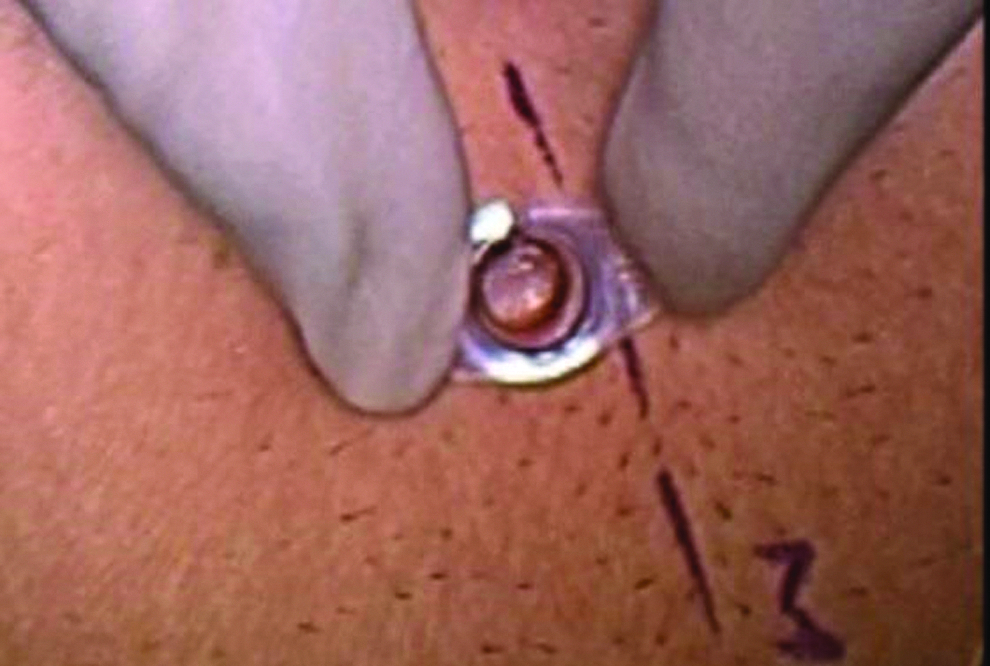
Manish Retractor helps in displacing the subcutaneous fat outward so that dissection up to ARS becomes easy. Remaining fat can be removed with the help of Suction. Shining ARS is visible at the base. ARS, anterior rectus sheath.
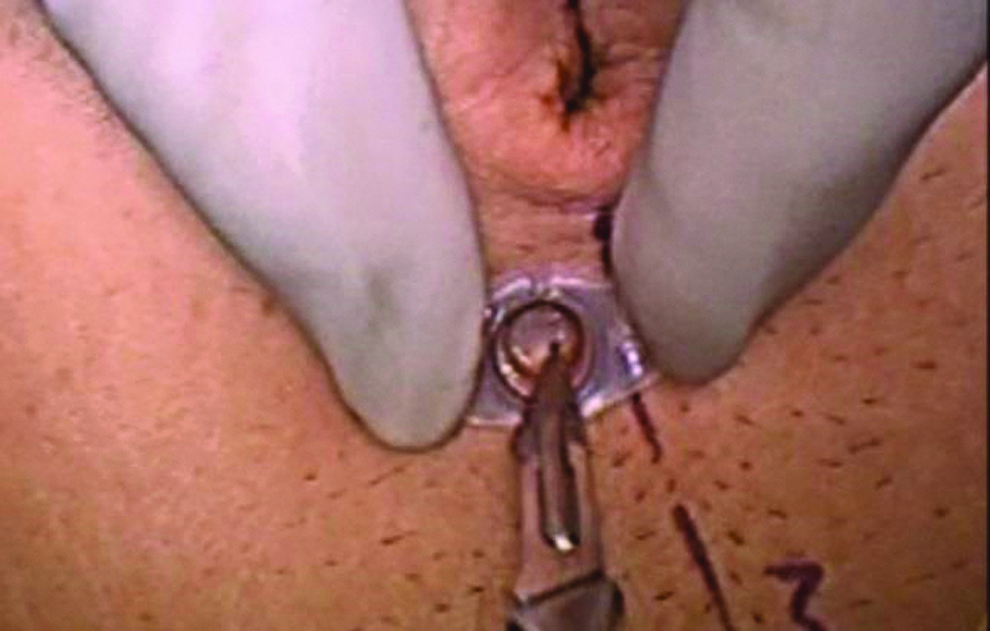
No. 11 surgical bade is used to make a transverse incision in ARS. ARS, anterior rectus sheath.
Longitudinal Rectus muscle fibers are visible beneath the slit in the ARS. ARS, anterior rectus sheath.
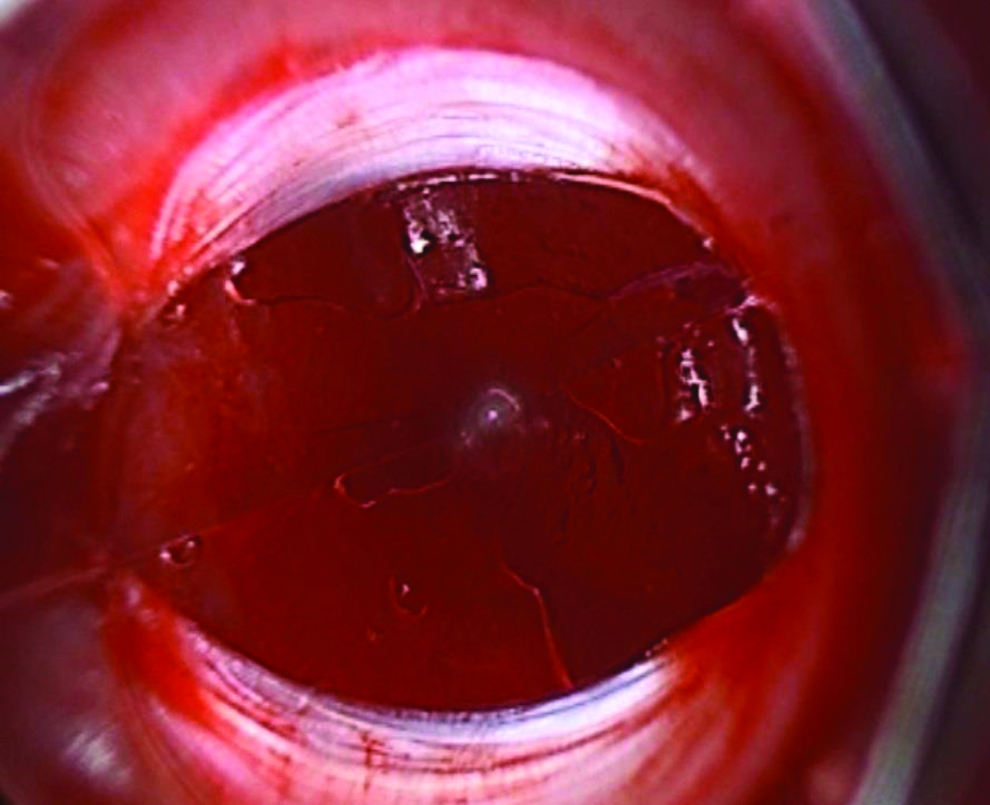
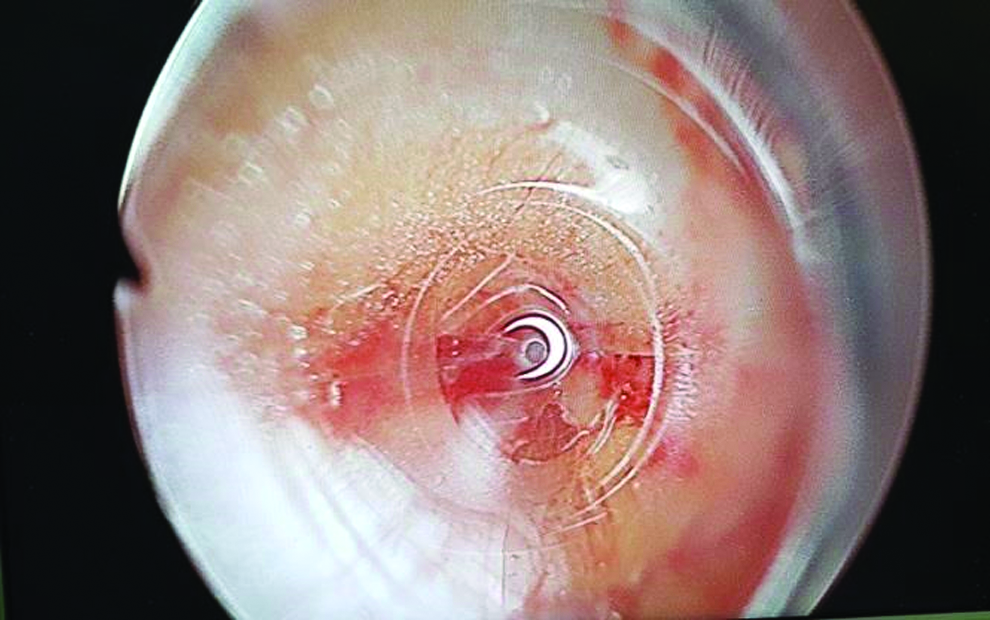
Five millimeters Visiport over 5 mm, 0° telescope is mounted to enter in to the PPS under vision. The Visiport is than introduced through the slit in ARS into the rectus muscle and finally into the PPS (Fig. 8). Just after entering through the slit in ARS one can easily appreciate the rectus muscle fibers laterally and fat along the linea alba on the medial side (Figs. 9 and 10). On further introducing the trocar, it crosses the arcuate line that can be clearly defined under vision. Further insertion of trocar leads to entry in the PPS, which can be easily identified by the appearance of preperitoneal fat (Figs. 11 and 12).

Visiport over 5 mm, 0° telescope is introduced through the Manish Retractor in to the slit in ARS to enter PPS. ARS, anterior rectus sheath; PPS, preperitoneal space.
Cranial and caudal lip of slit in ARS. ARS, anterior rectus sheath.
Rectus muscle is seen laterally (right side of picture) while fat is visible along the lineal alba medially (left side of picture).

Preperitoneal fat after crossing the arcuate line.

Pneumo insufflation helps in dissecting the preperitoneal space.
The telescope is then taken out after entering into the PPS, leaving the cannula of trocar at its place. carbon dioxide (CO2) is then connected to the cannula on 14 mmHg pressure and high flow. Manish Retractor is then taken out gently from the incision over the 5 mm trocar. The slit in the Manish Retractor facilitates its complete removal from the 5 mm trocar (Figs. 13 and 14). Skin, soft tissue, and ARS snugly holds the 5 mm trocar without any need of anchoring sutures and chances of CO2 leak from PPS.

Manish Retractor is taken out from the 5 mm port site wound over the trocar.

Slit in Manish Retractor helps in its complete removal from trocar without removing the trocar.
Dissection of extra-peritoneal space and port placement
Blunt dissection is done to create the Space of Bogros under vision with the help of 5 mm telescope. CO2 on high flow helps in creating this space, which is relatively avascular, containing loose areolar tissue. Dissection in PPS begins by dividing the loose areolar tissue in the midline to reach the pubic bone as first landmark. We are trained in performing TEP repair by lateral approach. Further dissection is done on the contralateral side of hernia to make two 5 mm working ports. In lateral approach, first working port is made just above the anterior superior iliac spine (ASIS) and another 5 cm cranial to it (Fig. 15). Surgeons who are trained in doing TEP with midline approach can also make midline ports.

Ports placement for TEP repair by Lateral approach. TEP, totally extra-peritoneal.
Dissection of hernia sac
Gentle dissection is done to reach up to the hernia sac and cord structures. Hernia sac is then dissected off from the cord structures and vas deferens. The sac is then tied with the catgut endo-loop after complete parietalization from spermatic vessels and vas deferens in the usual manner (Fig. 16).

Parietalization of indirect hernia sac.
Mesh insertion through 5 mm Visiport and placement
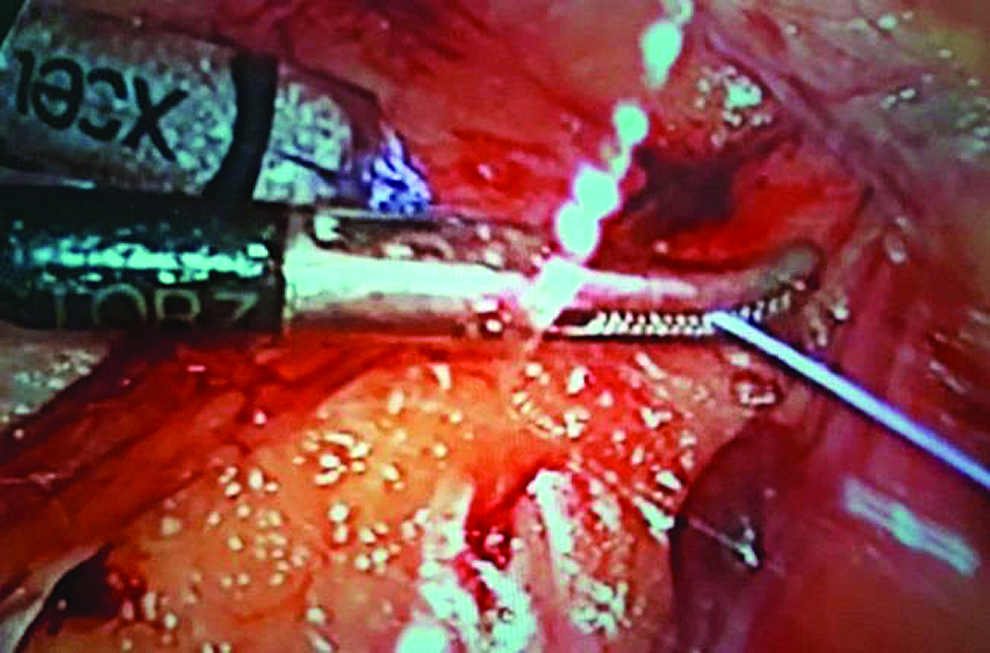
We have also innovated a technique for introducing the light weight polypropylene mesh through 5 mm working port. A 15 × 15 cm of light weight polypropylene mesh is cut to size and rolled to the thinnest possible thickness along its width. A 20 cm length of No. 1 silk thread is tied at the end of rolled mesh, which facilitates the pulling of mesh in the PPS (Fig. 17). The silk thread is first inserted through 5 mm working port and the end is left inside the PPS (Figs. 18 and 19). This end of the silk thread facilitates pulling of mesh inside the PPS with the help of grasper through another 5 mm working port (Fig. 20). The mesh is unrolled inside after cutting the silk thread. The mesh is then placed over the myopectineal space and fixed with tackers over Cooper's ligament and laterally above the ilio-pubic tract (Fig. 21). All 5 mm trocars are removed after deflating the CO2 (Fig. 22).

A 15 × 15 cm light weight prolene mesh is cut to size and rolled. A 20 cm silk thread is tied at its end.

Tail of the silk thread is inserted through 5 mm working port.

End of the tail of silk thread is left in the PPS. PPS, preperitoneal space.
Tail of the silk thread is pulled inside the PPS, which helps in mesh insertion. PPS, preperitoneal space.

Mesh is placed covering myopectineal space and fixed at cooper's ligament.

Scar of 5 mm incision in infra-umbilical region.
Closure of infra-umbilical port site wounds
There is no need to repair the defect in the ARS or subcutaneous fat of infra-umbilical port site wound as the defect is only of 5 mm size. The skin is stapled with single stapler.
Results
All 61 cases were operated by “555 Technique.” Out of 61 cases, 27 were indirect inguinal hernia (23 unilateral, 4 bilateral), 32 direct inguinal hernia (21 unilateral, 11 bilateral), 1 femoral hernia, and 1 obturator hernia. One patient had sliding hernia with sigmoid colon forming the posterior wall of the sac. Sixty cases were successfully operated by “555 Technique.” There was conversion to TAPP in 1 case because of dense peritoneal adhesions due to previous contralateral TEP repair.
The average time for insertion of 5 mm trocar in PPS by our technique was 150 seconds, which is less in comparison to conventional Hasson trocar placement. Pnemoperitoneum occurred in 4 cases that were managed by putting Veress needle in peritoneal cavity. In postoperative period analgesic requirement was less because of all 5 mm wounds.
Seven unilateral indirect inguinal hernias were irreducible and 4 unilateral indirect inguinal hernia patients had past history of contra-lateral repair. One patient had history of open inguinal hernia repair followed by recurrence, which was repaired by TEP approach. This patient first presented to us in outpatient department (OPD) with mesh infection and entero-cutaneous fistula subsequent to TEP repair. Mesh removal was done and ileum was repaired laparoscopically after freshening the enterotomy margins. Successful TEP repair of inguinal hernia was done after 2 months by “555 Technique.” One patient had indirect inguinal hernia 2 years after bilateral orchidopexy, which was repaired successfully with our technique. All the patients were followed up for 6 months in postoperative period and no incidence of SSI, hernia recurrence, chronic pain, or incisional hernia was noted. Small 5 mm infra-umbilical scar was cosmetically more acceptable to patients.
Discussion
Laparoscopic surgeons are now making the surgical procedures less and less invasive in terms of size of the incision and abdominal wall trauma. 6 In our “555 Technique” there is no need to make a large 12 mm infra-umbilical incision and need for Hasson trocar. Hasson trocar is now almost exclusively used for TEP repair of inguinal hernia.
Placement of Hasson trocar in infra-umbilical region is a standard practice for creating PPS in TEP repair of inguinal hernia. In the standard technique of TEP repair, a large 12 mm incision is made in the infra-umbilical region for insertion of Hasson trocar in the PPS. In our technique only a 5 mm incision is made in the infra-umbilical region, which is less invasive and is less painful in postoperative period. 5
In standard current practice retraction of 12 mm large incision is done with the help of large “S” retractors. This retraction is required for dissecting up to the ARS and making an incision to enter the PPS through a wide bore Hasson trocar. 7 In our technique the retraction is done by an innovative “Manish Retractor” made by 2 mL plastic syringe. Retraction of skin and subcutaneous fat by Manish retractor is less traumatic and provide a better view of ARS.
In standard current practice anchoring sutures are required to fix the Hasson trocar with the ARS to prevent loss of pneumo-insufflation. 8 Insertion of Hasson trocar in the PPS by holding the anchoring sutures is a relatively blind procedure. Though it is claimed that open technique of Hasson trocar insertion is under vision, but only the entry point of Hasson trocar placement is under vision, rest of the insertion into the PPS is blind. Also the insertion of wide cone of Hasson trocar in the PPS further widens the defect in the ARS by tearing its fibers. This relatively blind step of TEP repair can be a cause of accidental rupture of peritoneum leading to pneumo-peritoneum, which is one of the cause of difficult dissection and prolongation of surgical time in standard technique. 9 In comparison to this, in our technique the insertion of infra-umbilical first trocar placement is done under complete vision up to PPS and thus avoiding accidental injury to peritoneum. There is no need for anchoring sutures as the skin, subcutaneous fat, and ARS snugly fits the 5 mm trocar and prevent CO2 leak.
CO2 insufflation under high flow at 14 mmHg pressure helps in creating the PPS by blunt dissection. The rest of the steps and principals of TEP repair remains the same except technique of mesh insertion. Also, there is no need to repair the ARS as the defect size is only 5 mm wide.
In our technique we use 15 × 15 cm light weight polypropylene mesh, which is cut to size, rolled, and can be easily pulled inside through 5 mm port. The use of light weight polypropylene mesh is recommended in inguinal hernia repair to prevent complications like chronic pain, seroma, and so on. 10
In standard technique the fixation of cone of wide bore Hasson trocar further stretches the wound and tears the fibers of ARS, which leaves a bigger defect than 12 mm incision. This bigger defect in the ARS needs to be repaired by Vicryl sutures after completion of surgery. Large infra-umbilical wound also needs closure of subcutaneous fat with absorbable Vicryl sutures. Large wound causes increased morbidity in terms of more tissue trauma, pain, and high incidence of SSI. 11 In our technique there is no need to repair the defect of ARS or subcutaneous fat as the defect is only 5 mm in size. It is well known that pain severity and incidence of SSI are less in 5 mm port site wound than 12 mm wound.
The time taken for creation of PPS by “555 Technique” is 2.5 minutes, which is less in comparison to average 4–10 minutes in routine Hasson trocar placement.
The need and dependence over a costly Hasson trocar almost exclusively for TEP repair at present is ultimately reflected in surgical cost. Morbidity management of a larger port site wound also has financial impact on the patients. 12
A large infra-umbilical scar causes suboptimal cosmetic outcome in comparison to 5 mm port site scar. Big scars not only leave scar on the body but also on the mind and soul. 11
Conclusion
“555 Technique” for Mini TEP repair of inguinal hernia is a feasible option without compromising the principles of current practice of TEP repair. Innovation of simple “Manish Retractor” is the key in completing Mini TEP repair. This technique is simple, less invasive, less morbid, and cost effective as it avoids dependence over costly Hasson trocar with better cosmetic results.
Footnotes
Acknowledgments
We are thankful to all our colleagues who supported this work. We are grateful to Dr. V.K. Malik, Dr. C.S. Ramachandran, and Dr. B.B. Agarwal for encouraging us on each and every step. We are immensely grateful to Dr. Vijay Arora for sharing his pearls of wisdom and guiding us during the course of this work.
Disclosure Statement
No competing financial interests exist.