
Abstract
Abstract
Introduction:
Single-port laparoscopic surgery (SPLS) has gained popularity due to its cosmetic benefit, and therefore, has been applied to several kinds of benign operations, such as appendectomy and cholecystectomy. The safety and suitability of SPLS for colon cancer has not been widely proved. We aimed at validating the safety, efficacy, and short-term quality of life (QOL) of SPLS compared with conventional laparoscopic surgery (CLS) in patients with colon cancer.
Materials and Methods:
Between June 2010 and April 2011, a total of 62 patients with pathology-proven colon cancer were randomly allocated to two groups: SPLS and CLS. Data were analyzed according to the intention-to-treat principle.
Results:
In total, there were 62 patients (35 men and 27 women) with a mean age of 63.0 years (range, 38–82). The baseline characteristics of the patients and tumor factors were well balanced between two groups. The operation time and estimated blood loss were similar, whereas intraoperative complications only occurred in three patients, all of whom were in the SPLS group. Conversion to CLS or open surgery occurred in 6 (19.4%) patients of the SPLS group. The number of harvested lymph nodes and length of proximal and distal resection margins were not statistically different between two groups. Postoperative complications and recovery of bowel function were similar in both groups, but fatal postoperative complication occurred in one case in the SPLS group. The QOL between two groups was identical in all domains until postoperative 12 months.
Conclusions:
SPLS for colon cancer is feasible and can be performed by following oncologic principles. However, surgeons should be aware of the potential for unexpected adjacent organ injury (ClinicalTrial.gov identifier: NCT01203969).
Introduction
I
Single-port laparoscopic surgery (SPLS) was developed as a stepping stone to overcome the obstacles associated with NOTES, the ultimate goal of minimally invasive surgery. However, SPLS became a unique procedure for almost all operations performed with conventional laparoscopic surgery (CLS). Furthermore, this more advanced form of laparoscopic surgery can further reduce the surgical trauma and maximize the clinical benefits of minimally invasive surgery.
Until now, SPLS has been applied primarily for minor operations such as appendectomy and cholecystectomy, because there have been some obstacles in applying this new technique for major extended operations, such as poor ergonomics, insufficient triangulation, and limitation of instruments. Many authors have published a few case reports or case series reports about SPLS for colorectal resection. There is still not much solid evidence to support performing SPLS for colon cancer. The only proven benefit of SPLS is a cosmetic one.
This study was a prospective, randomized controlled trial (RCT) that compared the safety, efficacy, and short-term quality of life (QOL) of SPLS with CLS for advanced colon cancer.
Materials and Methods
From June 2010 to April 2011, eligible patients were recruited at 2 hospitals that were affiliated with the Department of Surgery, Kyung Hee University School of Medicine. Eligible patients were included by following these criteria: (1) Biopsy-proven adenocarcinoma or advanced adenomatous polyps (>1 cm) in the colon, (2) Stage I-III colon cancer in which right hemicolectomy or anterior resection was planned with curative intent. The exclusion criteria were as follows: (1) Tumor located in the distal transverse colon, splenic flexure colon, and descending colon where the extent of operation is not standardized and the techniques for laparoscopic surgery are challenging, (2) distant metastasis present at diagnosis, (3) adjacent organ invasion (clinical stage of T4bNxM0), (4) emergency operations due to acute colonic obstruction and/or perforation, (5) tumors associated with familial adenomatous polyposis or hereditary nonpolyposis colorectal cancer, (6) synchronous colorectal malignancy, (7) American Society of Anesthesiology (ASA) score more than 3, and (8) Pregnancy. Written informed consent was obtained from all patients who agreed to participate in this study. This prospective randomized study was approved by the Institutional Review Board of each hospital and was registered with the U.S. National Institutes of Health (ClinicalTrials.gov Identifier: NCT01203969).
Randomization
Randomization was done by using a computer-generated table of random sampling numbers, and enrolled patients were randomly assigned to the SPLS or CLS group at a ratio of 1:1. To maintain the allocation concealment, randomization was carried out just before the surgery through sealed envelopes containing the random numbers in the operating room.
Preoperative preparation and surgical procedure
Mechanical bowel preparation was performed with 4 L of polyethylene glycol and sodium phosphate enema. Patients fasted for 1 day before surgery. Second-generation cephalosporin was injected 1 hour before incision. A Foley catheter was inserted routinely, but a nasogastric tube was not used routinely.
Surgical procedure
For sigmoid colon cancer, patients were placed in lithotomy, Trendelenberg, and right-tilted position. In the SPLS group, the umbilicus was sterilized with 70% isopropanol and 35% hydrogen peroxide and the skin was then prepared with iodine solution. A transumbilical incision 3 to 4 cm in length was made, and a single-port device (Octoport® [dalimSurgNET, Inc., Seoul, South Korea] or SILS® [Covidien, Inc., Mansfield, MA]) was installed to establish the pneumoperitoneum with intraperitoneal pressure up to 12 mmHg. In the case of CLS, four trocars were placed: a 10 mm trocar in the supraumbilical area, a 12 mm trocar in the right lower quadrant (RLQ), and two 5 mm trocars in the right upper quadrant and left lower quadrant (LLQ), respectively. Intraperitoneal procedures were identical between the two groups. Under the vision of a 0 degree laparoscope, the mesocolon was dissected from the level of the promontory, and the inferior mesenteric artery was high-ligated with hemoloc clips and divided. The mesocolon and colon were fully mobilized from the retroperitoneum in the medial to lateral direction. The use of an articulating instrument was allowed to overcome the external crowding and poor ergonomics. The resected specimen was taken out through the umbilical incision. In the CLS group, the supraumbilical incision was extended into the umbilicus to make an incision with SPLS. Intracorporeal end-to-end anastomosis was completed by the double-stapling technique. The air-leak test was checked, and the draining tube was occasionally inserted at the surgeon's discretion.
For right colon cancer, the patient was positioned in a supine, Trendelenberg, and left-tilted position. The details of the operative procedure were described in our previous report. 8 In the case of CLS, four trocars were used: Two 10 mm trocars in the supraumbilical area and left upper quadrant, and two 5 mm trocars in the LLQ and RLQ.
Postoperative management
Patients were encouraged to begin early ambulation and deep breathing starting the day after surgery. Prophylactic antibiotics were discontinued on the day of operation, and the Foley catheter was removed at postoperative day 1. Pain was controlled exclusively by patient-controlled analgesia (PCA) composed of 15 μg/kg Fentanyl citrate, 180 mg Ketorolac tromethamine, and 0.6 mg Ramosetron (5-HT3 receptor antagonist). Oral feeding was initiated after first flatus and audible bowel sounds, and soft diet was started if patients were tolerable to sips of water. Discharge was considered when pain was controllable with oral analgesics, soft diet was tolerable, and there was no fever or other signs of complications.
Data collection and statistical analysis
The primary end points were perioperative complications defined by intraoperative and postoperative morbidity and 30 days of mortality, reflecting the technical safety of the procedure. The secondary end points included the number of harvested lymph nodes, length of the proximal and distal resection margin, operation time, estimated blood loss, rate of conversion to CLS or to open surgery, degree of postoperative pain, time to recovery of bowel movement, duration of postoperative hospital stay, and QOL. The length of incision was measured at the end of surgery. The oncologic adequacy of the new procedure was confirmed by the number of retrieved lymph nodes and length of both resection margins. The pathologists who performed the lymph node count and measured the resection margins were blinded to the operative technique. To detect a difference of 30% in perioperative complications with an 80% power of the test and 1-sided alpha of 0.05, 31 patients were included in each group.
Perioperative data for the patients and tumors were collected prospectively through the case reporting form. A total of 67 patients were eligible for the study; five patients declined to participate, and thus 62 patients were allocated randomly into two groups for inclusion in statistical analysis. QOL was surveyed with The European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 9 third edition (Korean version) preoperatively and postoperatively at months 1, 3, 6, and 12 at outpatient visit or by telephone interview, as appropriate. Statistical analysis of data was performed with SPSS® version 15.0 for Windows (SPSS, Inc., Chicago, IL). Two-tailed Student's t-test was used for continuous variables, and the chi-square test was used for nominal variables. A P < .05 was considered statistically significant. All analyses were based on the intention-to-treat principles.
Results
Thirty-one patients were randomly assigned into both the SPLS and CLS groups (Fig. 1). The patient group included 35 men and 27 women with a median age of 63 years (range, 38–82 years). Baseline characteristics of patients and the tumors were well balanced between both groups (Table 1). Sixteen (25.8%) patients out of the total had a previous history of abdominal surgery.
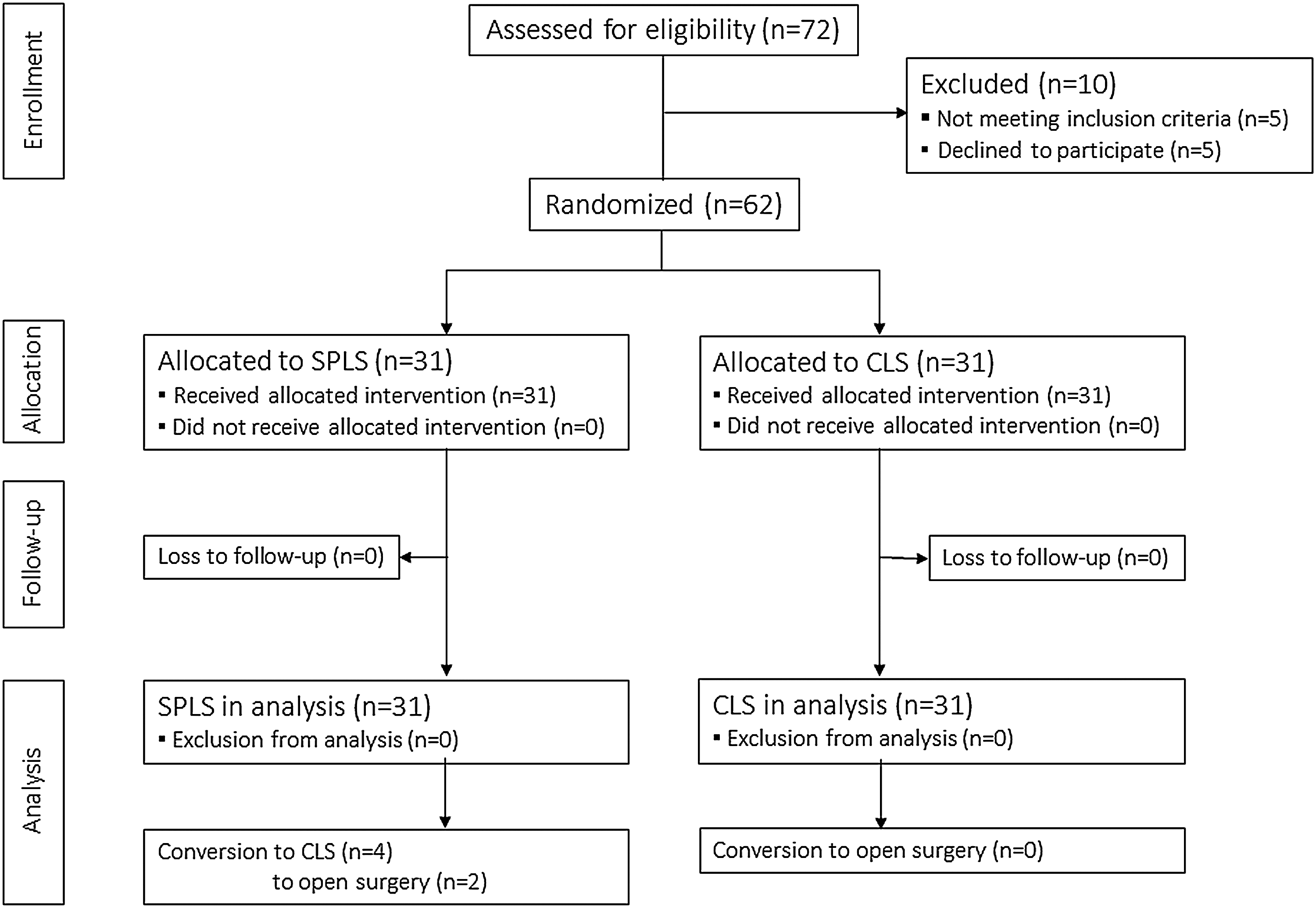
CONSORT diagram. CLS, conventional laparoscopic surgery; SPSL, single-port laparoscopic surgery.
Values are number of patients (percent) or mean ± SD.
ASA, American Society of Anesthesiologists; BMI, body mass index; CA, carbonic antigen; CEA, carcinoembryonic antigen; CLS, conventional laparoscopic surgery; SPLS, single-port laparoscopic surgery; SD, standard deviation.
Operative outcome
Operation time was similar in both groups, despite the poor ergonomics for surgeons in SPLS (mean value: 134.9 versus 130.9 minutes in the CLS group, P = .706). The total length of incision was about 1.2 cm longer in the CLS group, but the length of the laparotomy wound was 0.8 cm longer in the SPLS group because of the somewhat larger tumor size and two open-converted cases in the SPLS group. There was more blood loss in the SPLS group, but this difference did not reach statistical significance (median value: 30 versus 20 mL in the CLS group, P = .073). Intraoperative complications occurred in 3 patients (9.7%) in the SPLS group, whereas no intraoperative complications occurred in the CLS group, although this difference was not statistically significant (P = .238). Among 3 patients with complications, two had a small bowel injury that required primary repair and one had bleeding that was managed by transfusion. Drain tubes were more frequently used in the CLS group, regardless of less blood loss and fewer intraoperative complications (35.5% versus 16.1% in the SPLS group, P = .082). Conversion to open or multi-port laparoscopic surgery occurred in 6 patients (19.4%) of the SPLS group; open conversion occurred in two patients (6.5%) due to severe intra-abdominal adhesion. Conversion to reduced port laparoscopic surgery with addition of either a single 5 or 12 mm port insertion occurred in 4 patients (12.9%). Parameters reflecting oncological adequacy of surgery such as number of harvested lymph nodes and length of proximal and distal resection margin showed no statistical difference between the two groups (Table 2).
Values are numbers of patients (percent) or mean ± SD/median (range).
CLS, conventional laparoscopic surgery; SD, standard deviation; SPLS, single-port laparoscopic surgery.
Postoperative course
Postoperative outcomes were relatively equivalent in both groups (Table 3). The time to functional recovery, time to first oral intake, and postoperative length of hospital stay were similar between both groups. Postoperative complications occurred in 6 patients (19.4%) of the SPLS group (2 cases with bleeding requiring transfusion, 2 urinary retentions managed by re-catheterization, 1 wound dehiscence, and 1 aspiration pneumonitis) and 4 patients (12.9%) of the CLS group (2 cases with urinary retention, 1 wound infection, and 1 wound seroma) (P = .490). One death was caused by aspiration pneumonitis in the SPLS group. There were no unscheduled readmissions in either group.
Values are number of patients (percent) or mean ± SD.
CLS, conventional laparoscopic surgery; SPLS, single-port laparoscopic surgery; PCA, patient-controlled analgesia.
Postoperative pain score and wound
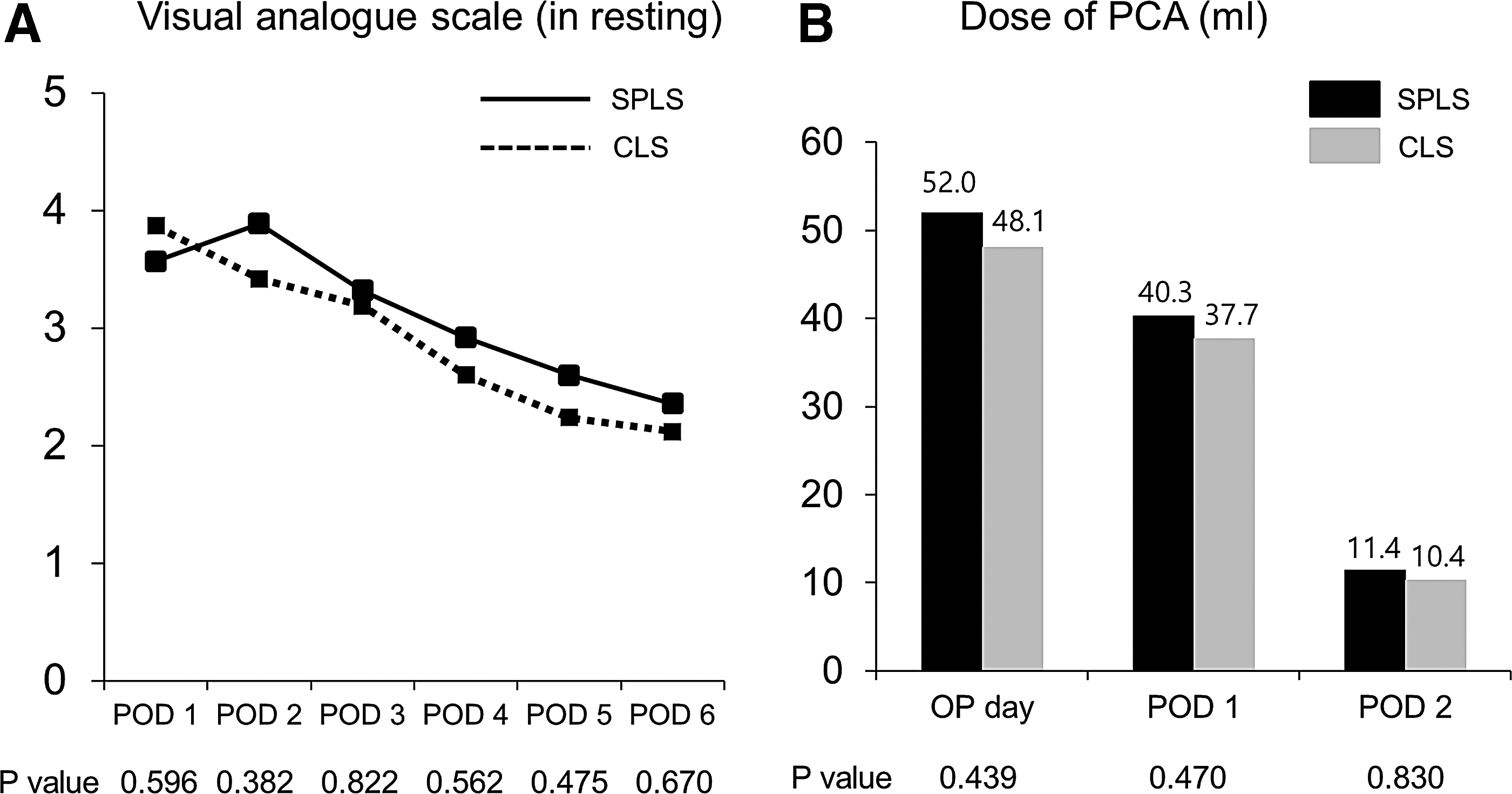
Over the course of the postoperative recovery, resting pain had diminished and the amount of analgesics also decreased. The degree of postoperative pain tended to be high in the SPLS group from postoperative day 2 to 6, but that difference was not large enough to show statistical significance (Fig. 2). The correlation between postoperative pain and the length of total incision showed a weak relationship with only marginal significance (P = .076) at POD 1, but there was no correlation after postoperative day 2 (Table 4). In the multivariate analysis of factors that predict the length of laparotomy wound, tumor size was the single determining factor (Table 5).
Postoperative pain score
POD, postoperative day.
Values are number of patients (percent).
BMI, body mass index; CI, confidence interval.
Quality of life
Global health status and five items of functional scale (physical, role, emotional, cognitive, and social functioning) gradually increased with time, and there were no significant differences during the study period (Fig. 3A–F). On the symptom scale, all nine items (fatigue, nausea and vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties) showed similar improvement over time without any differences. But nausea/vomiting and appetite loss were slightly aggravated at postoperative month 3 and then showed constant improvement (Fig. 4A–I).
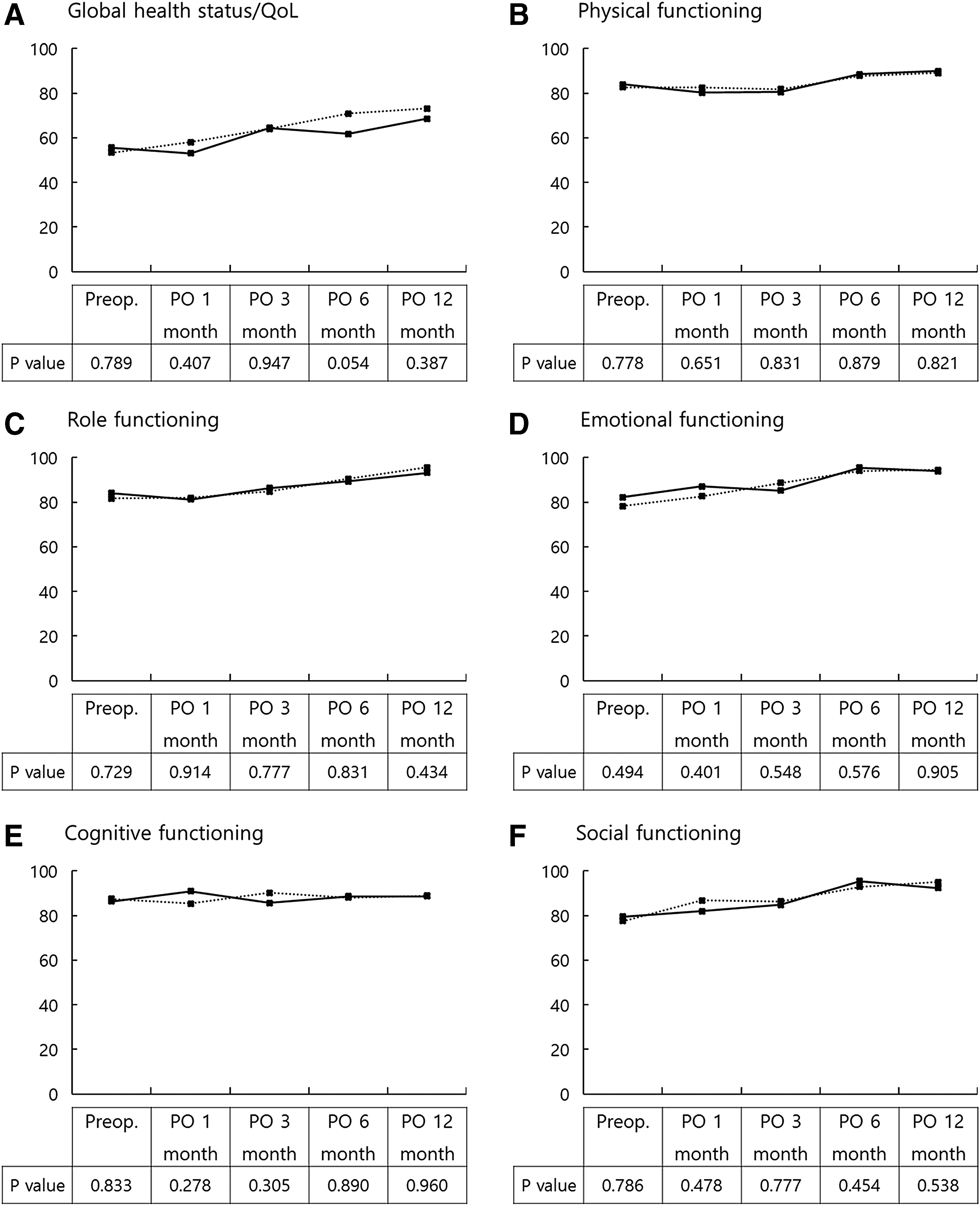
Quality of life (Global health status and Functioning scales). Pairs of dots show score of SPLS (solid line) and CLS (dotted line). High score means a high level of quality of life (QOL) or functioning. CLS, conventional laparoscopic surgery; PO, postoperative; SPLS, single-port laparoscopic surgery.
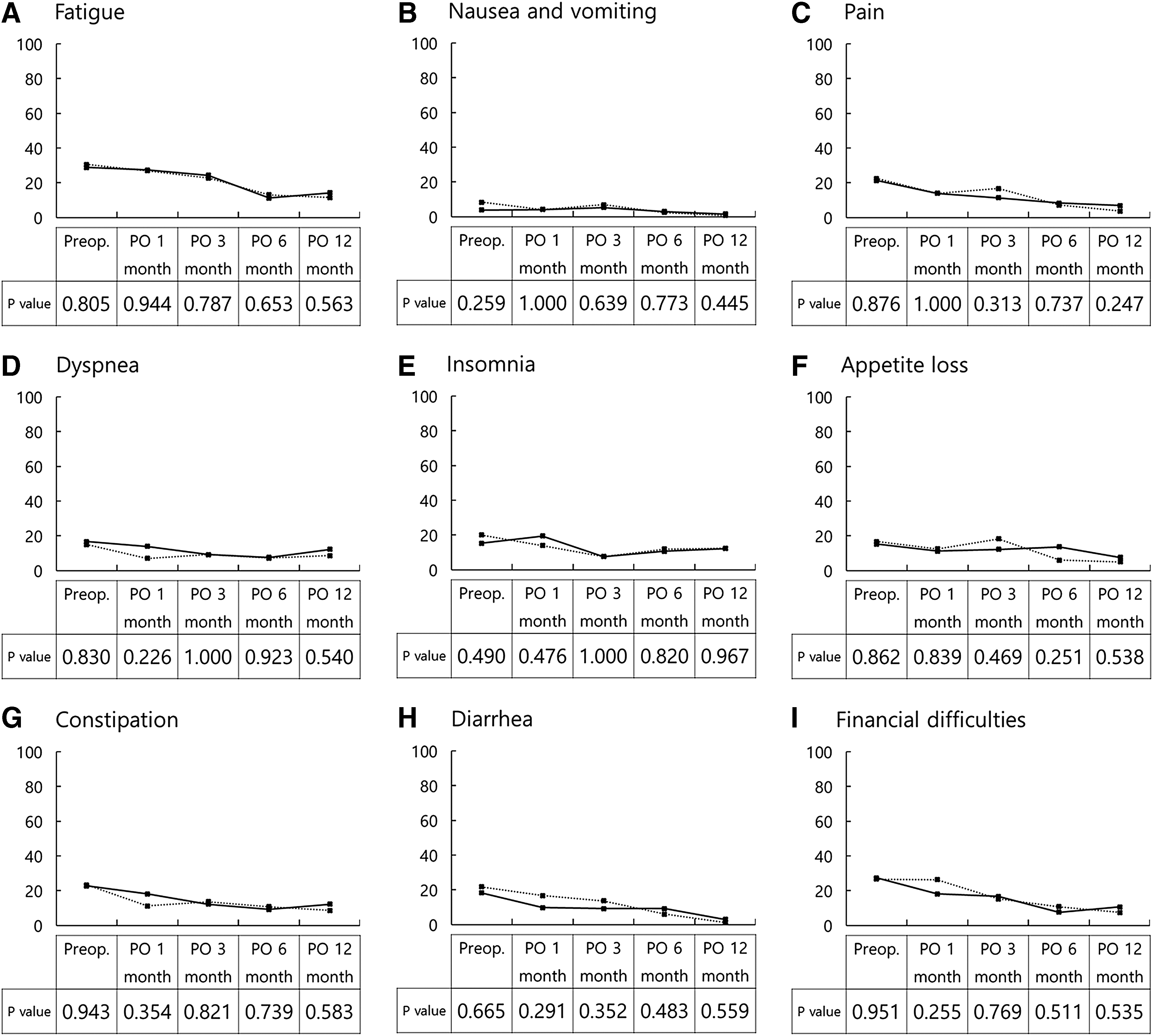
Quality of life (symptom scales). Pairs of dots show score of SPLS (solid line) and CLS (dotted line). High score means severe symptoms. SPLS, single-port laparoscopic surgery; CLS, conventional laparoscopic surgery; PO, postoperative.
Discussion
Technical obstacles of SPLS are caused primarily by poor ergonomics and absence of an optimized instrument for SPLS. New technology for cancer surgeries should be validated in terms of technical safety as well as oncologic safety with respect to obtaining sufficient resection margins, number of harvested lymph nodes, and survival of patients. We tried to confirm whether SPLS is a technically feasible and oncologically safe procedure for colon cancer.
In our trial, the number of harvested lymph nodes and length of proximal and distal resection margins, which reflect oncologic compatibility, were not different between the SPLS group and the CLS group. Operation time and estimated blood loss, which reflect technical safety and stability, were similar between the two groups. The rate of intraoperative complications did not vary significantly between the two groups; however, the sample size of this study may have been too small to detect a difference. Intraoperative complications occurred in 3 patients, exclusively in the SPLS group. In addition, postoperative complications leading to mortality occurred in one patient from the SPLS group. There seems to be a learning curve with SPLS, but we did not analyze the learning curve for SPLS, because the number of operations was not sufficient and the operation time did not differ between the two groups.
All of the previous studies on SPLS for the colorectum were small case studies or case-matched, control studies. Most of these studies included benign diseases such as diverticulitis, Crohn's disease, and endometriosis as well as malignancy.10–15 To the best of our knowledge, only two RCTs were published and they showed results similar to our results,16,17 but did not provide information about the QOL of patients. In 4 studies about right colon cancer, the total operation time,10–13 estimated blood loss,10,12 total length of incision,10,12,13 and rate of perioperative complication10,11 did not differ; the number of harvested lymph nodes10–12 and length of postoperative hospital stay10–12 were comparable between the SPLS and CLS groups. Another three studies targeted colorectal cancer exclusively.18–20 In all 3 studies, operation time, estimated blood loss, number of harvested lymph nodes,18,20 and length of proximal and distal resection margins18,20 were similar between the two groups, demonstrating that SPLS is a safe and feasible procedure for oncologic resection in colon cancer. Results for postoperative pain were somewhat diverse. Papaconstantinou demonstrated that the pain score for postoperative days 1 and 2 was significantly lower in the SPLS group compared with that of the CLS group. 12 However, other studies have reported that postoperative pain scores 14 and dosage of analgesics10,14,20 were similar between the two groups.
The most objective advantage of SPLS is the cosmetic benefit of a smaller wound in the abdominal wall. In our study, the length of the laparotomy wound with SPLS was longer, because the tumor size was 0.8 cm bigger in SPLS and there were two open conversions in the SPLS group, but the total length of the incision was 1.2 cm longer in the CLS group. If tumor size was similar in both groups, such benefit would be more magnified. Most of other trials evaluating differences in the incision length revealed a longer scar with CLS regardless of statistical significance.12–15 Therefore, the consequential cosmetic benefit seemed to be clear. In addition to the objective length of the incision, we made a transumbilical incision, which is another cosmetic benefit because the umbilicus could hide a scar of about 2.5 cm postoperatively.
However, the differences in the length of incision did not lead to a reduction in the postoperative pain in our study. During the whole postoperative period, there was no difference in the pain score between the two groups. The pain score was higher in the SPLS group after postoperative day 2, and a higher dosage of PCA was used in the SPLS group. Similar results were reproduced in another randomized trial for appendicitis by St. Peter et al. 21 and Kim et al. 22 The possible explanation for increased pain in SPLS is the longer time for the umbilical procedure for SPLS. In contrast, the wound with CLS was maintained for a short time for extracorporeal procedures and was closed immediately. Therefore, the operative stress of laparotomy would be less in CLS.
At postoperative day 1, there was weak correlation between surgical pain and the length of incision, and tumor size was an independent determining factor. Therefore, in the case of a bulky tumor, the length of the laparotomy wound could be longer and the postoperative pain and cosmetic benefits of SPLS might be compromised.
The postoperative time for functional recovery and the length of hospital stay were similar between the two groups. Interestingly, although the time to first passage of flatus was the same, the time to sips of water was slightly faster in CLS and even earlier than the time of gas passage. These findings might reflect the familiarity and trust of the operator with CLS. In a future trial, a more concrete protocol for the progress of diet is necessary.
The most important reason that SPLS has not been rapidly adopted in colorectal surgery is the poor ergonomics and resulting technical difficulty with SPLS compared with CLS. Like the initial laparoscopic trials in colon cancer, the operation time could be longer and more intraoperative complications might occur. In our study, however, the operation time was almost the same. In a previous observational study for colon cancer, the operation time was not different and Egi et al. reported a slightly longer operation time with CLS (192 minutes in SPLS versus 222 minutes in CLS, P = .063). 19 Therefore, technical difficulties for the initial introduction of SPLS could be overcome rapidly by experts of laparoscopic surgery. SPLS is basically one form of laparoscopic surgery, and laparoscopic surgeons are already familiar with instruments used in SPLS. Generally, to overcome the learning curve for laparoscopic colorectal resection, 30 to 70 cases are needed.23–25 As expert surgeons overcome this learning curve for colon cancer, fewer cases are needed to plateau the learning curve for SPLS.
Conversion to reduced port laparoscopic surgery was needed for 4 patients with left colon cancer in the SPLS group. In two patients, a single 5 mm trocar was inserted for insufficient traction of the target organ due to a huge uterine myoma and congenital adhesion around the sigmoid colon. Another 2 patients required an additional 12 mm trocar for introduction of a laparoscopic linear stapler device, because the location of the distal margin was too low to transect the rectum perpendicularly from the umbilical port.
In both groups, the QOL showed a similar pattern in which all items progressively improved, even when compared with the baseline value, and postoperative differences were not identified until 1 year. Therefore, the quality of postoperative life did not deteriorate with this novel approach. A slight worsening of nausea/vomiting and appetite loss might reflect some adverse effects of adjuvant chemotherapy.
Based on the promising results from this study, we started a new trial with a large number of patients in each group (n = 194) to ascertain the feasibility and safety of SPLS in colon cancer and to evaluate the long-term oncologic safety of SPLS under the leadership of the Korean Society of Endoscopic and Laparoscopic Surgeons (ClinicalTrial.gov identifier NCT01480128).
In conclusion, this study clearly demonstrates comparable short-term outcomes and adequacies with SPLS for colon cancer. However, caution is needed during SPLS to avoid intraoperative complications. SPLS has clear cosmetic benefits and did not compromise postoperative QOL.
Footnotes
Disclosure Statement
No competing financial interests exist.