
Abstract
Abstract
Aim:
To compare intracorporeal anastomosis (IA) and extracorporeal anastomosis (EA) in laparoscopic right colectomy (LRC) in terms of intraoperative and postoperative outcomes.
Methods:
A systematic literature search with no limits was performed in PubMed and Embase. The last search was performed on April 9, 2016. The outcomes of interests included intraoperative outcomes (operative time, blood loss, length of incision, conversion, lymph nodes harvested, and intraoperative complications) and postoperative outcomes (time to first flatus, time to first defecation, time to liquid diet, length of hospital stay, postoperative complications, mortality, ileus, anastomotic leakage, anastomotic bleeding, wound infection, hernia, and intra-abdominal abscess).
Results:
Fifteen articles and four conference abstracts published between 2004 and 2016 with a total of 1957 patients were enrolled in this meta-analysis. IA was associated with significant less blood loss, smaller length of incision, shorter time to first defecation, shorter time to liquid diet, and shorter length of hospital stay. No differences were found for operative time, conversion, lymph nodes harvested, intraoperative complications, time to first flatus, postoperative complications, mortality, anastomotic leakage, anastomotic bleeding, ileus, wound infection, intra-abdominal abscess, or hernia between IA and EA.
Conclusion:
Our meta-analysis suggests that the IA for LRC improves cosmesis and results in better postoperative recovery outcomes without increasing intraoperative and postoperative complications. Furthermore, a large randomized control study is warranted to compare the short-term and long-term outcomes of those two anastomosis techniques.
Introduction
S
For laparoscopic right colectomy (LRC), there are two anastomosis procedures: intracorporeal anastomosis (IA) and extracorporeal anastomosis (EA). LRC with IA is also named “total LRC,” in which vascular ligation, tumor extraction, and anastomosis are all performed intracorporeally. In LRC with EA, vascular ligation and tumor extraction are done intracorporeally, while anastomosis is performed extracorporeally.5,10 Theoretically, IA could have several advantages, such as quicker recovery to bowel function due to reduced traction on the colon, shorter skin incision, and an alternative incision site for extraction. Contrarily, IA might need a longer operation time, and the additional technical difficulty of IA makes surgeons need a learning curve to perform it. 11
Nowadays, there is a debate about which of those two anastomosis techniques is better for LRC. Previous three meta-analyses have been reported comparing IA and EA, however, the results were controversial.12–14 Feroci's study concluded that patients with IA had a faster postoperative recovery, 12 while the other two studies failed.13,14 Those three meta-analyses have limitations. First, all of them enrolled small number of studies; the maximum number of including articles was seven. Second, Cirocchi et al. and Carnuccio et al. did not do meta-analysis for intraoperative and some postoperative outcomes, while Feroci et al. used median and range values of some enrolled studies to conduct analysis, which was not appropriate. There is still lack of overwhelming evidence on which one is the better anastomosis technique. Herein, we conduct a meta-analysis to compare IA and EA in LRC in terms of intraoperative and postoperative outcomes.
Materials and Methods
Study selection
A systematic literature search with no limits for studies comparing IA and EA in LRC was performed in PubMed and Embase. Our search strategy included terms “colectomy, colectomies, hemicolectomy, or hemicolectomies” and “EA, extracorporeal anastomoses, IA, or intracorporeal anastomoses” and “laparoscopic-assisted, laparoscopies, laparoscopic, or laparoscopy.” The last search was performed on April 9, 2016. A manual search of references of articles and reviews was also performed for additional potentially eligible studies.
Inclusion and exclusion criteria
The inclusion criteria for this meta-analysis were as follows: (1) Case–control study (IA versus EA); (2) LRC; (3) Studies with total sample size more than 20; and (4) Intraoperative and/or postoperative outcomes were reported. The exclusion criteria studies were as follows: (1) Studies including robotic technique; (2) Studies including patients with natural orifice specimen extraction; and (3) Animal studies. If studies included patients of same period and same hospital, study with larger sample size was enrolled in this meta-analysis.
Data extraction
Two authors (Wu QB and Jin CW) independently reviewed all identified studies. Discrepancies were resolved by discussion. If agreement could not be reached, a third reviewer (Wang ZQ) would be required. The following items were extracted from each study: first author's name, year of publication, publication type, study type, bowel preparation, disease, number of patients in each arm, and outcomes of interests.
Outcomes of interests
Intraoperative outcomes: operative time, blood loss, length of incision, conversion, lymph nodes harvested, and intraoperative complications.
Postoperative outcomes: length of hospital stay, time to first flatus, time to first defecation, time to liquid diet, postoperative complications, mortality, ileus, anastomotic leakage, anastomotic bleeding, wound infection, intra-abdominal abscess and hernia.
Quality assessment
The methodological quality of the enrolled retrospective studies was assessed using the revised and modified grading system of the Scottish Intercollegiate Guidelines Network. 15 Articles achieving less than 8 scores, 8–14 scores, and more than 14 scores (total score, 20) were defined as poor quality, fair quality, and good quality, respectively. And the methodological quality of the randomized controlled trials was assessed by modified Jadad score system (total score, 5; 1–2, low quality; 3–5, high quality). 16
Statistical analysis
All data analyses were conducted using the Review Manager version 5.0 (The Cochrane Collaboration, Software Update, Oxford) and P < .05 was considered statistically significant. Weighted mean difference (WMD) was calculated for the continuous outcomes, and pooled odds ratios (OR) or risk ratios (RR) were calculated for the dichotomous outcomes. For continuous outcomes, if the study only provided means and range values or median and range values, the means and standard deviations were calculated using methods described by Hozo et al. 17 Chi-squared test and Higgins I-squared test were used for heterogeneity test. A value of P < .05 and I2 > 50% was regarded as existing heterogeneity. If I2 > 50% and P < .05, a random-effects model was applied. Correspondingly, if I2 < 50% and P > .05, a fixed-effects model was applied. Begg's funnel plot was used to evaluate publication bias.
Results
A flow chart of the literature search was shown in Figure 1. The initial search algorithm retrieved a total of 354 studies. There existed 273 studies after duplicated removed. After the initial review, only 44 relevant studies were further evaluated. Besides, one additional record was identified through manual search. Of these studies, 26 reports were excluded due to following reasons: six studies included natural orifice specimen extraction or robotic technique; one studies included mixed series colectomy without right hemicolectomy data; one conference abstract did not present outcome data; six studies were review or meta-analysis; five studies were not case–control study; one study was comment without data; and six studies had overlap patients. Thus, 15 articles18–32 and 4 conference abstracts33–36 published between 2004 and 2016 were included in our meta-analysis. One of 15 articles was randomized controlled trial. 24 The characteristics of the included studies were summarized in Table 1. A total of 1957 patients (994 by IA and 963 by EA) were enrolled.

PRISMA diagram.
Methodological qualities of included retrospective studies were assessed using the revised and modified grading system of the Scottish Intercollegiate Guidelines Network (Total score, 20; <8, poor quality; 8–14, fair quality; >14, good quality).
Methodological qualities of included randomized controlled trials were assessed by modified Jadad score system (Total score, 5; 1–2, low quality trial; 3–5, high quality trial).
RCCS, retrospective case–control study; PRCT, prospective randomized controlled trials; NR, not reported; NA, not applicable; IA, intracorporeal anastomosis; EA, extracorporeal anastomosis.
Quality of included studies
The scores of methodological quality assessment of the enrolled retrospective studies and randomized controlled trial were shown in Table 1 (Supplementary Tables S1 and S2; Supplementary Data are available online at www.liebertpub.com/lap). Of those 15 articles, 12 retrospective studies had fair quality (10–13 scores),18,19,21–23,26–31 two retrospective studies had good quality (15 scores),20,25 and one randomized controlled trial had high quality (4 scores). 24
Meta-analysis of intraoperative outcomes
There were no statistically significant difference between IA and EA concerning the operative time (P = .41, WMD = 3.32, 95% confidence interval (CI) (−4.58, 11.23), I2 = 72%), conversion (P = .74, OR = 0.82, 95% CI [0.25, 2.67], I2 = 59%), lymph nodes harvested (P = .32, WMD = −0.91, 95% CI [−0.88, 2.71], I2 = 74%), or intraoperative complications (P = .67, OR = 0.75, 95% CI [0.21, 2.74], I2 = 0%). However, although there existed heterogeneity, we observed a significant less blood loss (P = .03, WMD = −24.87, 95% CI [−46.87, −2.88], I2 = 82%) and smaller length of incision (P < .001, WMD = −2.21, 95% CI [−3.15, −1.28], I2 = 97%) in IA group (Fig. 2).
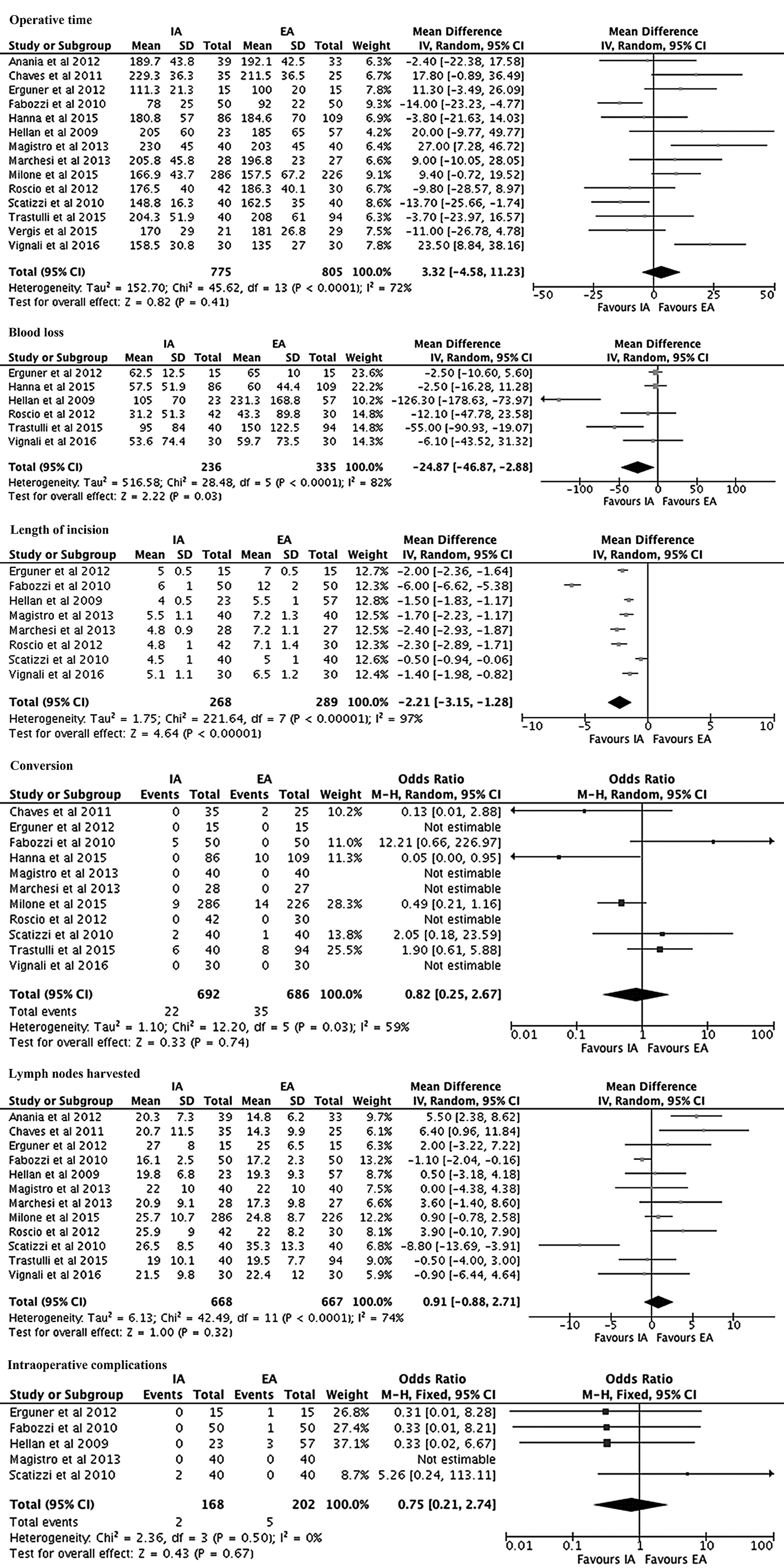
Meta-analysis of intraoperative outcomes. IA, intracorporeal anastomosis; EA, extracorporeal anastomosis.
Meta-analysis of postoperative outcomes
Length of hospital stay was shorter in IA group (P < .001, WMD = −1.03, 95% CI [−1.57, −0.48], I2 = 68%), and time to first defecation (P < .001, WMD = −0.65, 95% CI [−0.97, −0.32], I2 = 53%) and time to liquid diet (P = .002, WMD = −0.87, 95% CI [−1.41, −0.33], I2 = 0%). Nevertheless, no significant differences were observed in terms of time to first flatus (P = .20, WMD = −0.23, 95% CI [−0.57, 0.12], I2 = 90%), postoperative complications (P = .15, OR = 0.74, 95% CI [0.49, 1.12], I2 = 56%) or mortality (P = .37, RR = 0.59, 95% CI [0.19, 1.86], I2 = 0%) (Fig. 3).
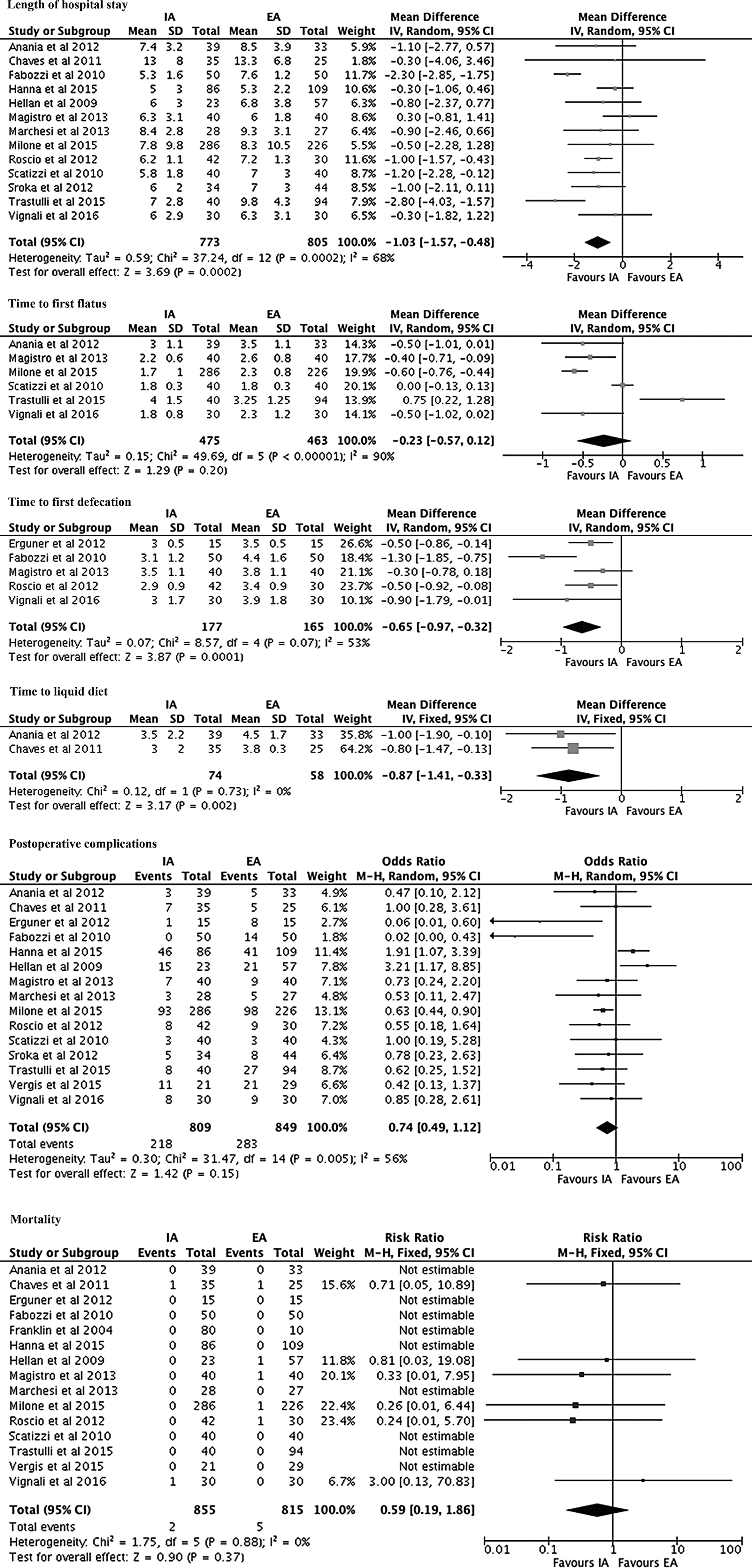
Meta-analysis of postoperative outcomes. IA, intracorporeal anastomosis; EA, extracorporeal anastomosis.
Furthermore, we analyzed complications particularly associated with surgery, and no differences were observed for anastomotic leakage (P = .34, OR = 0.77, 95% CI [0.45, 1.31], I2 = 0%), anastomotic bleeding (P = .75, OR = 0.82, 95% CI [0.24, 2.82], I2 = 0%), ileus (P = .41, OR = 1.20, 95% CI [0.78, 1.87], I2 = 34%), wound infection (P = .05, OR = .68, 95% CI [0.46, 1.00], I2 = 45%), intra-abdominal abscess (P = 1.00, OR = 1.00, 95% CI [0.30, 3.27], I2 = 0%), or hernia (P = .10, OR = 0.45, 95% CI [0.18, 1.16], I2 = 0%) between IA and EA group (Fig. 4).

Subgroup analysis of IA versus EA for malignant disease. IA, intracorporeal anastomosis; EA, extracorporeal anastomosis.
Subgroup analysis of IA versus EA for malignant disease
Subgroup analysis was conducted to compare the results of IA and EA in patients with malignant disease (Table 2). Ten studies19–24,26,28,29,34 were enrolled (676 by IA and 508 by EA). We observed that IA group had smaller length of incision (P < .001, WMD = −2.31, 95% CI [−3.63, −0.98], I2 = 98%), shorter time to first flatus (P = .02, WMD = −0.38, 95% CI [−0.71, −0.05], I2 = 89%), shorter time to first defecation (P < .001, WMD = −0.65, 95% CI [−0.97, −0.32], I2 = 53%), shorter length of hospital stay (P = .01, WMD = −0.97, 95% CI [−1.73, −0.21], I2 = 75%), and less postoperative complications (P < .001, OR = 0.54, 95% CI [0.41, 0.72], I2 = 31%) between two groups (Table 2).
OR.
RR.
WMD.
Bold values signify when p value < 0.05.
IA, intracorporeal anastomosis; EA, extracorporeal anastomosis; OR, odds ratio; RR, risk ratio; WMD, weighted mean difference; CI, confidence interval; NA, not applicable.
Publication bias
A funnel plot of the studies reporting on postoperative complications shows that there was no obvious publication bias among the studies, though four studies lay outside the limits of the 95% CI (Fig. 5).
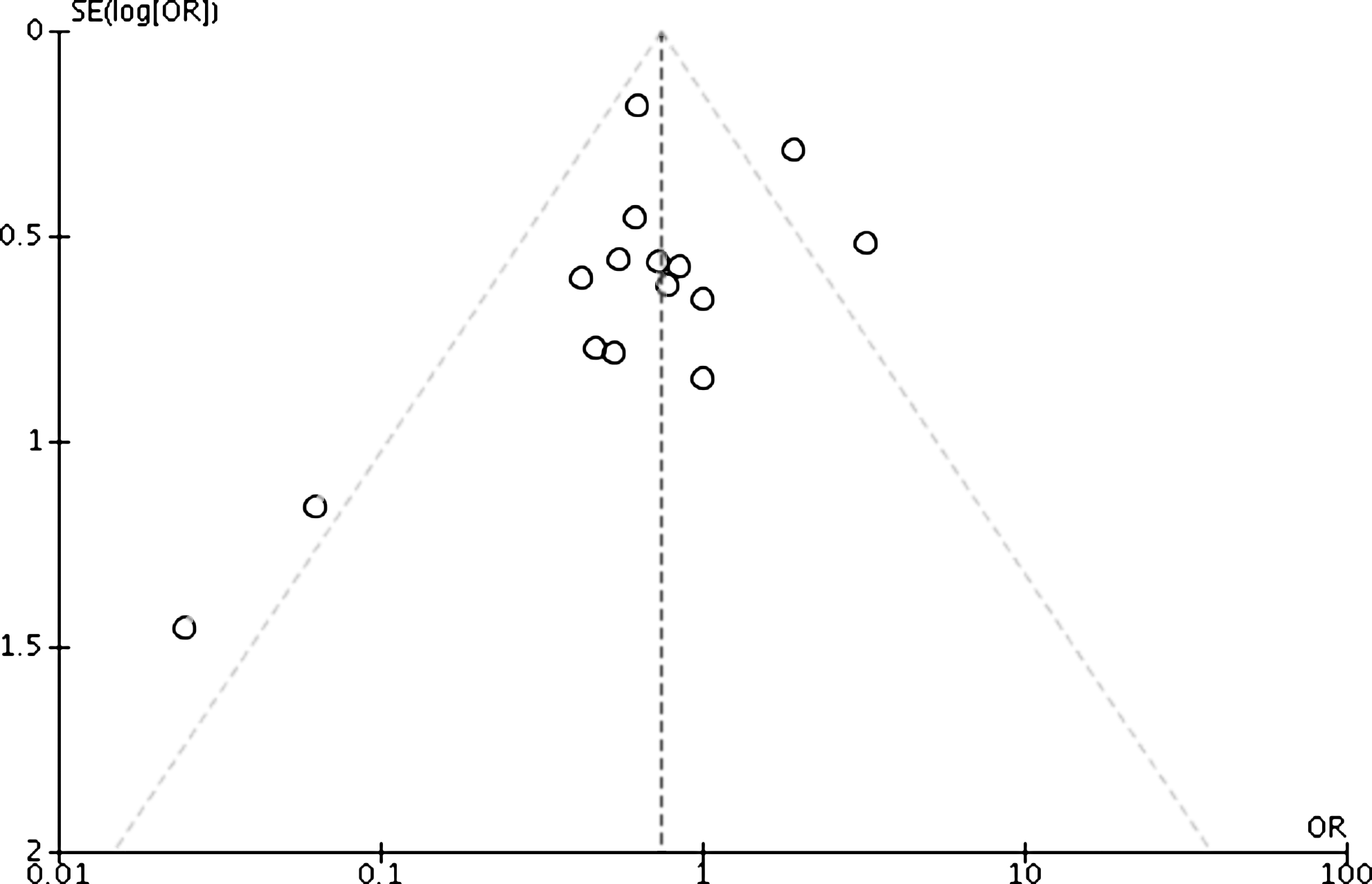
Funnel plots of the studies reporting on postoperative complications.
Discussion
Schinkert first reported LRC, and since then, LRC has become more and more widely accepted. 37 In LRC, there are two anastomosis techniques (IA and EA) for reestablishing intestinal transit. As there is controversy about the benefits and safety of both, there is a debate about which of those two anastomosis techniques is better. In our meta-analysis including 19 studies with 1957 patients, IA group showed a significantly less blood loss and smaller length of incision, which are in line with the previous meta-analysis and reviews.12,38,39 Considering that, compared with EA, the IA in LRC can improve cosmesis for patients.
Interestingly, different from previously published review, 39 there was no significant difference in the operative time. The result is supported by Feroci's meta-analysis. 12 The possible reason is that although the time for anastomosis is longer in IA group (P = .03, WMD = 23.48, 95% CI [1.74, 45.22], I2 = 94%), it might need less time to mobilization due to the reducing traction on the colon in IA group. Thus, the total operative time had no difference between two groups. No significant difference was observed in the conversion, lymph nodes harvested, or intraoperative complications, either.
As expected, our analysis revealed a significantly shorter time to first defecation, time to liquid diet, and length of hospital stay in IA group. Because less mobilization of transverse colon and mesocolon was needed in IA group, the recovery of bowel function is quicker and patients could discharge earlier. 14 However, we found no difference in the time to first flatus, and total postoperative complications or mortality.
When it comes to complications particularly associated with surgery, our pooled results showed no differences were observed for anastomotic leakage or intra-abdominal abscess. Carnuccio et al. thought that the increased technical difficulty of IA might result in a greater likelihood of an anastomotic leak, 14 however, based on our analysis, there is no significant difference between the two groups in terms of anastomotic leakage. Both of groups had a low anastomotic leakage rate (2.5% in IA group and 3.2% in EA group). Theoretically, it might be more likely that the succus entericus can flow into abdominal cavity more easily in IA group because the bowel was transected and anastomosed in the abdominal cavity. Thus, the intra-abdominal abscess might be developed more easily in IA group. However, although only three included studies reported this complication, the pooled data of our meta-analysis showed no significant difference (2.8% in IA group and 2.5% in EA group). Our reasonable explanation is that abdominal cavity irrigation after anastomosis can wipe off most of succus entericus, and the remaining is too little to develop intra-abdominal abscess. Besides, no significant difference was observed in the anastomotic bleeding, ileus, wound infection, or hernia.
We did not analysis the learning curve of the IA and EA and its effect on intraoperative and postoperative outcome because the data had not been reported, and the effect of obesity. Based on our surgical experience, we think that the IA technique might need a longer learning curve for LRC; additionally, it might be more difficult to perform IA for obesity patients.
In the subgroup analysis of malignance disease, IA can also improve cosmesis and result in better postoperative recovery outcomes. Besides, IA can decrease the postoperative complications. Regarding oncological clearance, the pooled data showed no difference was found in lymph nodes harvested. This was because the dissection, mobilization, and vascular ligation were performed similarly in both groups.28,40 We did not analyze the survival of cancer patients due to only one study reporting the survival data. Furthermore, none of enrolled studies represented the data about the number of exfoliated cancer cells in abdominal cavity.
The strength of this meta-analysis: (1) our meta-analysis included more articles and more patients than previous studies; (2) we analyzed intraoperative and postoperative outcomes, and the pooled data showed that compared with EA, IA could provide a faster recovery of bowel function and a shorter length of incision; and (3) we also conducted subgroup analysis of IA versus EA for malignant disease.
Some limitations of this study have to be highlighted. Frist, there existed high heterogeneity in some analyses. Though the sensitivity analysis was conducted by removing one study each time, the outcomes remained unchanged. We thought it might be influenced by many factors, such as the experience of surgeon, usage of drainage tube and nasogastric tube. Third, most of the enrolled articles were retrospective studies. This might induce patient selection bias. Although there was one randomized controlled trial, it was an ongoing trial, and the number of patients was small.
In conclusion, our meta-analysis suggests that the IA in LRC improves cosmesis and results in better postoperative recovery outcomes without increasing postoperative complications. Furthermore, a large randomized control study is warranted to compare the short-term and long-term outcomes of those two anastomosis techniques.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Support Program of the Science & Technology Department of Sichuan Province (Grant numbers: 2016SZ0043) and the National Natural Science Foundation of China (Grant numbers: 81172373).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.