
Abstract
Abstract
Background:
The purpose of this study was to compare different techniques for pediatric laparoscopic inguinal hernia repair. We hypothesize that the amount of dissection performed at the internal ring, with or without division of the peritoneum, will impact healing and thus long-term success of the repair.
Methods:
Following the Institution's Animal Care and Use Committee approval (708024-4), 20 Hartley guinea pigs underwent laparoscopic repair of their natural open internal rings. The guinea pigs were divided equally into four surgical groups: intracorporeal suture repair (IS), hernia dissection and division with intracorporeal suture (DDIS) repair, subcutaneous endoscopically assisted ligation (SEAL), and Yueng (HOOK) repair. After a 6-week survival period, a necropsy was performed. Repairs were evaluated and tested under pressures up to 30 mmHg. The suture was then removed to assess primary healing. Experimental data were analyzed using chi-square test.
Results:
There were no perioperative or postoperative complications. On initial evaluation, before suture removal, repair integrity was as follows: 5/10 IS, 10/10 DDIS, 7/10 SEAL, and 7/10 HOOK (P = .09). After suture removal, repair integrity was as follows: 3/10 IS, 10/10 DDIS, 5/10 SEAL, and 6/10 HOOK (P = .01).
Conclusion:
Overall, dissecting and dividing the sac with intracorporeal suture (DDIS) closure had the best outcome. This method appears to best replicate standard open high ligation.
Introduction
I
Currently, there is no accepted standard laparoscopic technique compared to the standard open high ligation. Our study focused on comparing various laparoscopic techniques to evaluate the differences observed in recurrence rates and healing that occurs at the internal ring. We hypothesize that the amount of dissection performed at the internal ring, specifically dissection and division of the hernia sac, will most favorably impact healing and thus long-term success of the repair. Currently, this method is not favored in clinical practice due to its technical difficulty.
Materials and Methods
The study was approved by the Institution's Animal Care and Use Committee (708024-4). Male Hartley guinea pigs were utilized in this study because they have naturally patent internal rings. A total of 20 guinea pigs, weighing greater than 650 g, were utilized in this study. The guinea pigs were randomized equally into the four surgical groups described below.
Before the procedure, the guinea pigs were acclimated to their housing for 7 days. After the acclimation period, the guinea pigs were anesthetized using intraperitoneal injection of ketamine 87 mg/kg and xylazine 13 mg/kg and a subcutaneous injection of buprenorphine 0.05–0.1 mg/kg. A preoperative antibiotic dose of chloramphenicol 30 mg/kg was administered. After adequate sedation was achieved, the animal's abdominal fur was clipped from nipples to groin. They were then prepped and draped in a sterile manner. The animals were maintained under general anesthesia with inhaled isoflurane through a nose-cone device.
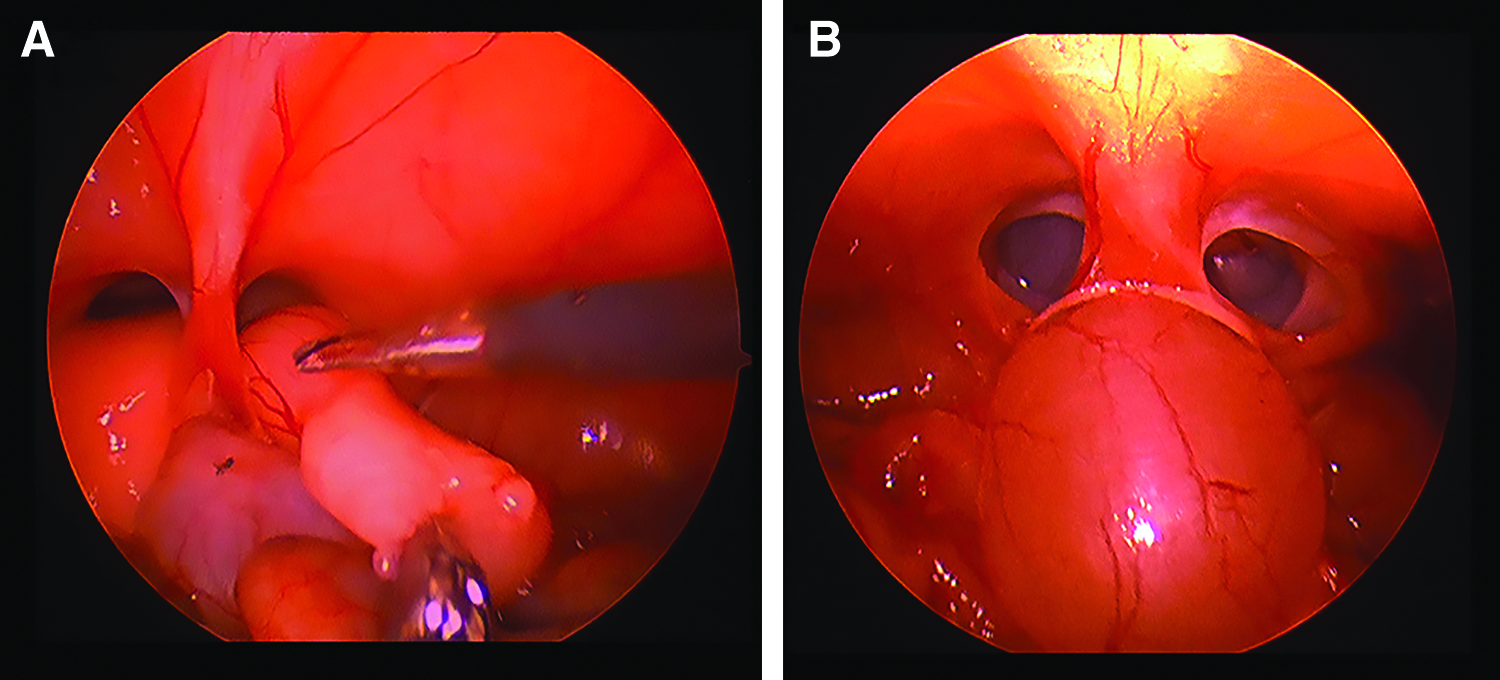
In all animals, a 3-mm incision was made a finger breath below the xyphoid, and an open technique used to gain intra-abdominal access. A 3 mm graphite port was then secured in place and a 3-mm 30° laparoscope was introduced; the abdomen was then insufflated to 5 mmHg. Two 3-mm incisions were then made 2–3 cm laterally and 1 cm inferior from the subxyphoid incision. Since the testicles in guinea pig pass through the internal ring (Fig. 1A), they were retracted into the abdominal cavity and the gubernaculum was transected using laparoscopic Metzenbaum scissors. Two open inguinal rings were well visualized at the completion (Fig. 1B). One of the following repairs was then performed. In an attempt to eliminate other possible causes of tissue reaction, Prolene suture was used in this study for all repairs.
Techniques
Group 1: Intracorporeal suture repair
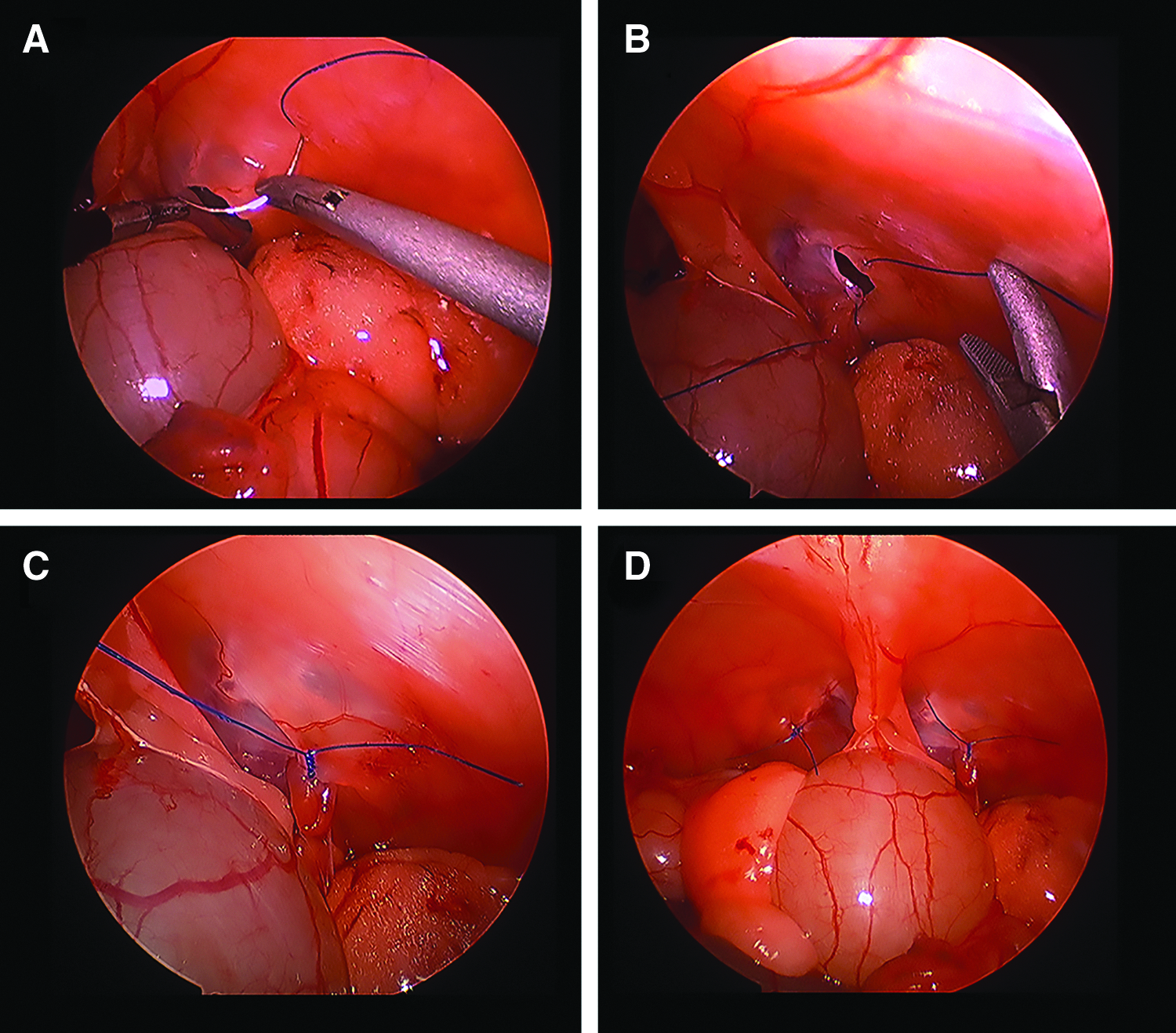
Both inguinal ring defects were closed with 5-0 Prolene in a figure of eight manner (Fig. 2A–D). The repair was completely intracorporeal.
Intracorporeal suture repair method.
Group 2: Dissection and division with intracorporeal suture repair
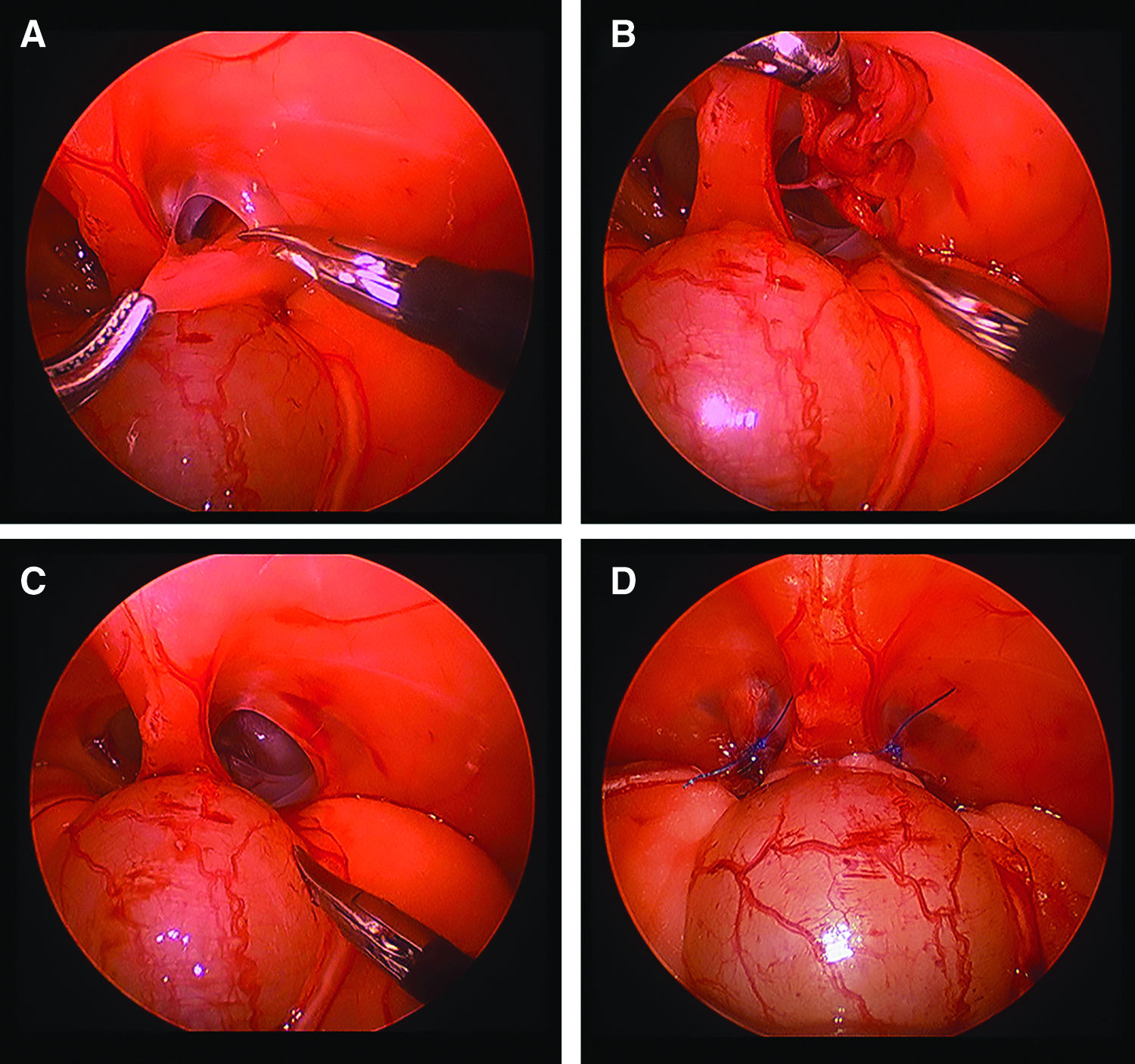
The peritoneum was incised circumferentially using laparoscopic Metzenbaum scissors and then fully dissected and transected (Fig. 3A–C), a technique similar to that described by Becmeur et al. 9 The inguinal ring defect was then closed with 5-0 Prolene in a figure of eight manner as above (Fig. 3D).
Dissection and division with Intracorporeal Suture Repair.
Group 3: Subcutaneous endoscopically assisted ligation
In this group, the defect was repaired using the described subcutaneous endoscopically assisted ligation (SEAL) technique as described by Harrison et al. 4 A 5-0 Prolene suture was utilized to close the defect.
Group 4: Yueng (HOOK) repair
Using C.K. Yueng's described laparoscopic-assisted extraperitoneal technique with the hook, the internal ring defect was closed. 5 A 5-0 Prolene suture was utilized to close the defect.
At the completion of the procedure, the incisions were closed with 5-0 Monocryl. The skin was then fully closed with adhesive glue.
Postoperatively, the animals were survived and evaluated for 6 weeks. Meloxicam 0.5 mg/kg subcutaneous injections were given postoperatively for pain control. Due to postanesthetic urinary retention, the bladders were manually emptied immediately postoperatively and every 12 hours for the first 24–48 hours. To improve recovery in the first two postoperative days, the animals were administered the following: Lactated Ringers 10–20 cc boluses daily, Vitamin C 10 mg/kg daily, and syringe-fed Critical Care® (Oxbow Animal Health, Murdock, NE) recovery food thrice a day.
At the completion of 6 weeks, the guinea pigs were anesthetized using intraperitoneal injection of ketamine 87 mg/kg and xylazine 13 mg/kg. Once appropriately anesthetized, the subxyphoid incision was opened. A 3 mm graphite port was inserted and the abdomen then insufflated to 5 mmHg. The repairs were laparoscopically visualized closely for any evidence of failure. Any openings noted or any increase in size of the defect was reported as a repair failure. After inspection, the animals were euthanized with a single dose of Fatal Plus® 100 mg/kg (Vortech Pharmaceuticals, Dearborn, MI). After verification of absence of signs of life, insufflation pressures were then increased in increments of 5 mmHg up to a maximum of 30 mmHg in which each pressure was held for 30 seconds each. The pressure was then reduced back to 5 mmHg and the intra-abdominal or subcutaneous knot was cut without disrupting the repair, and then removed. Insufflation pressures were then increased once again in the same manner to a maximum pressure of 30 mmHg. Any failures of the repair were observed and recorded; this included any visualized holes in the repair or air within the scrotum.
Analysis
Data were analyzed using chi-square test. A P-value of ≤.05 was considered statistically significant.
Results
All 20 guinea pigs survived the postoperative period without complication. During the postoperative period, two guinea pigs were noted to have evidence of recurrence on physical examination. One guinea pig was in the SEAL group and the other in the HOOK group. Otherwise, on gross inspection, no evidence of hernia was appreciated in the remainder of the guinea pigs.
During initial inspection at 5 mmHg before suture removal, multiple repairs were noted to have failed. The intracorporeal suture repairs without dissection had the highest recurrence rate, followed by the SEAL and Hook repairs with equal recurrence rates. However, there was no statistically significant difference in the success rates of the repairs: 5/10 IS, 10/10 DDIS, 7/10 SEAL, and 7/10 Hook (P = .09). Recurrences observed before suture removal are shown in Figure 4.
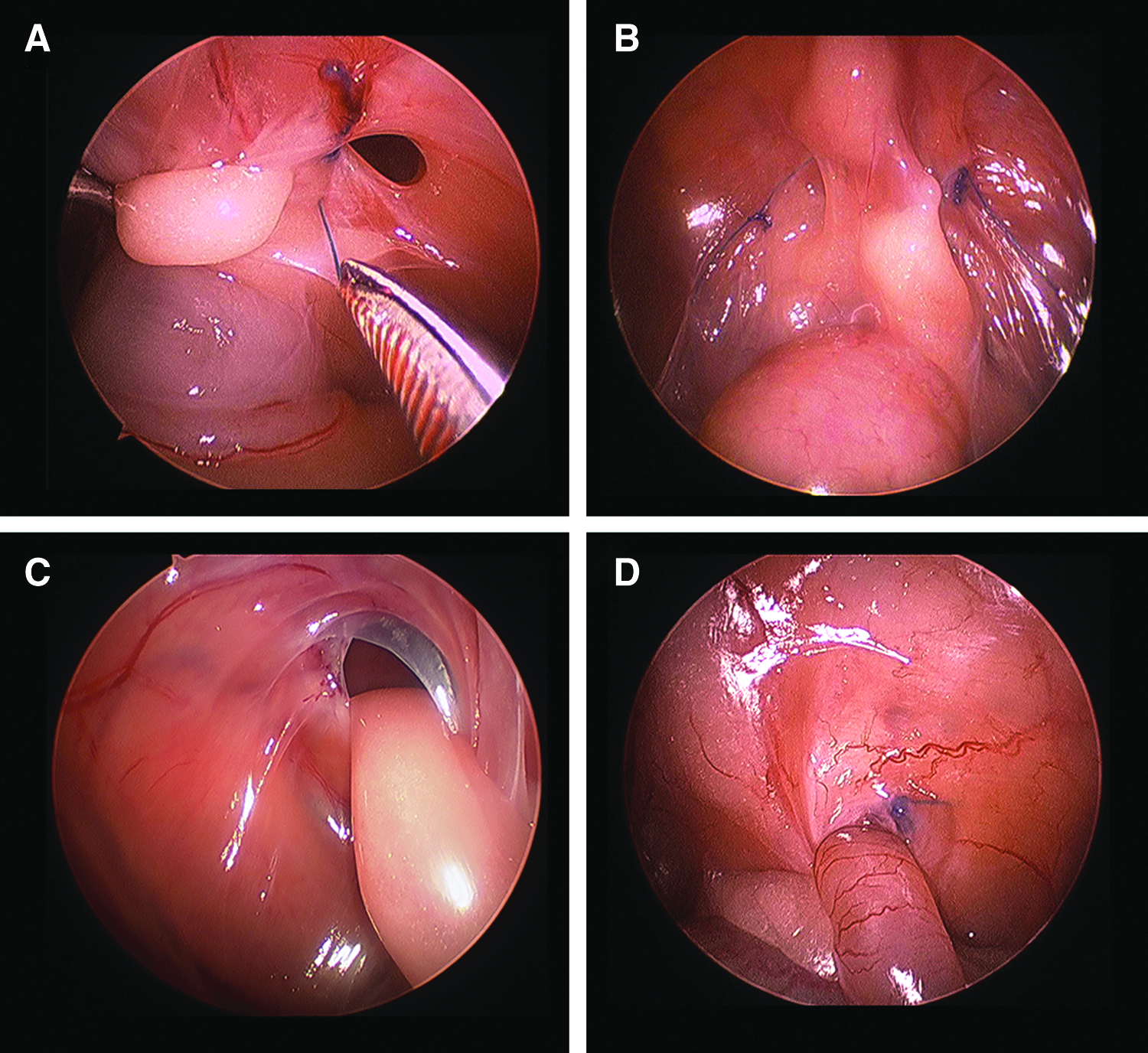
Example images of failed repairs before suture removal.
After suture removal, the DDIS group was the only group to remain successful; all other repairs had further failures. After suture removal, there was a statistically significant difference in the integrity of the repairs: 3/10 IS, 10/10 DDIS, 5/10 SEAL, and 6/10 Hook (P = .01).
Discussion
High ligation of the hernia sac is the current accepted standard of care for pediatric hernia repairs. With advancements in minimally invasive surgery, many have attempted to establish a laparoscopic repair with similar or better recurrence rates. Although some have successfully accomplished this, laparoscopic inguinal hernia repairs have not replaced the standard open high ligation. A comparison of the open to laparoscopic technique found no benefits to the latter. 10 The hook method described by C.K. Yueng has a reported recurrence rate of 0.35% comparable to the open approach. 11 Another well-known approach, the SEAL technique, on the other hand, has a reported recurrence rate of 4.3%. 12 Many other techniques have been described with varying recurrence rates ranging from 0% to 5%.13–21 These techniques are a variation of intracorporeal and extracorporeal approaches. Compared to the open repair, the majority of the described laparoscopic approaches leave the hernia sac intact. Boo et al. did evaluate the feasibility of laparoscopic herniotomy and intracorporeal closure and found comparable recurrence rates to the open approach. 7 With the various approaches available, we sought to determine which laparoscopic technique would best reproduce the results seen with an open herniotomy in a guinea pig animal model.
This pilot study revealed that complete dissection and division of the hernia sac led to a 0% recurrence rate. The increased trauma to the area likely led to an increase in scarring, thus resulting in improved repair and reduced recurrence. These findings are consistent with the observations noted in the rabbit hernia repair model by Blatnik et al., 22 which revealed that sharply incising the peritoneum around the internal ring decreased recurrence rates. Thus, the difference in the integrity of the repair noted between the DDIS and IS group can be attributed to the localized trauma from the herniotomy.
Studies have demonstrated that it is feasible to reproduce the surgical principles of the open herniotomy laparoscopically in children.7,9 Follow-up after these repairs was short term, however the recurrence rates were low and similar to the open approach. Although our survival period was only 6 weeks, the necropsy allowed us to further evaluate the repairs at high pressures. Despite pressures up to 30 mmHg, the DDIS repair remained intact, while the other repairs had further failures, demonstrating the true strength of this repair. We can therefore hypothesize that the increased trauma to the area from the herniotomy largely impacted the integrity of the repair.
In a prospective study, Riquelme et al. found that resection of the hernia sac without closure of the internal ring led to high success rates. 21 This study evaluated 91 patients and again noted that the trauma to the inguinal region was sufficient to cause obliteration of the internal ring. However not all patients were eligible for this repair as patients with openings greater than 10 mm were excluded from this treatment. These data further support the theory that increased trauma impacts repair.
Controversy continues on the use of permanent versus absorbable suture for hernia repairs. The concern for increased inflammatory reaction and stitch abscess formation makes permanent sutures less appealing. Kelly et al. observed that the type of suture did impact the closure of the internal ring in laparoscopic repairs. 23 Silk was found to have better outcomes compared to Vicryl and Prolene sutures. The increased inflammatory reaction noted with the silk suture was assumed to be the cause of observed results. Since these prior studies have demonstrated that the type of suture does contribute to the integrity of the repair, we opted to use Prolene in an attempt to remove this as a variable. Overall, we can infer that the increased trauma to the area likely led to better internal ring closure rates, and we believe the suture did not impact this.
By fully dissecting and dividing the hernia sac the intracorporeal suture closure had the best outcome. With 0% recurrence rate, this method appears to best mimic the standard open high ligation repair in both technique and recurrence rate. Further studies with a higher number of subjects and longer survival periods are needed to validate these findings. This technique may also be the best candidate to evaluate the use of absorbable suture in future studies.
Footnotes
Disclosure Statement
No competing financial interests exist.