
Abstract
Abstract
With the introduction of laparoscopy, the outcomes of patients undergoing paraesophageal hernia repair have improved dramatically. When the fundamentals of a proper repair are followed, patients can expect to have improvement in gastroesophageal reflux symptoms, including heartburn, regurgitation, chest pain, dysphagia, and dyspnea. Adhering to these principles will alleviate patients' symptoms and avoid reoperation. This article describes the approach to paraesophageal hernia repair, including patient evaluation, operative technique, and postoperative management. Esophageal lengthening and crural reinforcement with mesh are addressed as well. Adhering to the basic techniques outlined in this article should lead to successful and durable patient outcomes following a paraesophageal hernia repair.
Introduction
L
Patient selection and preoperative evaluation are essential for successful paraesophageal hernia repair. Symptoms caused by paraesophageal hernias result from intermittent obstruction and/or gastroesophageal reflux. Intermittent obstruction can cause dysphagia, nausea, emesis, and early satiety. Frequently, gastroesophageal reflux manifests as heartburn and regurgitation. Some patients may experience respiratory symptoms, including cough, pneumonia, and dyspnea, as a consequence of aspiration of esophageal contents or a large hernia that compresses the right atrium. Patients can also develop anemia secondary to bleeding from Cameron's ulcers. Rarely, patients may present with acute severe symptoms consistent with hernia incarceration. Paraesophageal hernia incarceration is a surgical emergency that may lead to gastric ischemia and ultimately necrosis if not addressed promptly.
Traditional teachings dictated that all paraesophageal hernias required operative repair due to the substantial morbidity and mortality associated with acute hernia incarceration and strangulation. 1 More recent evidence suggests that in the absence of severe symptoms, the risk of strangulation is lower than the risk of complications from laparoscopic hernia repair. 2 As a result, the presence of a paraesophageal hernia does not compel repair in asymptomatic or minimally symptomatic individuals. The threshold for offering a patient operative correction of their hernia should be lower for younger patients as they are at a higher cumulative risk of incarceration. Elderly patients with symptomatic hernias who are at reasonable operative risk should be offered hernia repair regardless of their chronologic age.3,4 Obesity is a risk factor for hernia recurrence and reoperation following an initial repair. 5 For this reason, the morbidly obese patient may be better served with concurrent weight loss surgery at the time of paraesophageal hernia repair.6–8
Patient Evaluation
A majority of patients suspected of having a paraesophageal hernia undergo a barium esophagram. This initial test establishes the presence of a hernia, while approximating the diameter of the hiatal defect and the orientation of the hernia contents. Every patient should be evaluated with an upper endoscopy before hernia repair. Mucosal disease (Barrett's esophagus, neoplasia, ulcers, etc.) as well as the axial distance from the esophagogastric junction (EGJ) to the diaphragm should be noted during the endoscopy. High-resolution manometry is another useful tool for surgical planning. Manometry probes may be difficult to place and lower esophageal sphincter pressures may be difficult to obtain and interpret based on the hernia contents. Despite this, we advocate the use of routine manometry to gauge the effectiveness of esophageal peristalsis and the distance between the EGJ and the crural diaphragm (if the catheter can be passed into the abdominal cavity). Patients with aperistalsis, and those with severe dysphagia with inability to pass a manometry catheter, should undergo a partial fundoplication at the time of hernia repair. In general, a 360-degree fundoplication is performed for all other patients. Preoperative 24-hour pH monitoring is unnecessary since the results of the test would not impact the procedure.
Technique
The following narrative describes the technical details of operative therapy.
Positioning
The patient is positioned supine on the operating table with legs abducted in a straight position. The right arm is tucked, facilitating placement of a liver retractor mount on the right side of the table. A bean bag mattress is used to maintain the patient's position on the operating table in extreme reverse Trendelenburg position.
Port placement
Five ports are used and additional ports are placed as needed in unique or challenging cases. The port for the laparoscope is positioned 12 cm below the xiphoid in the mid-left rectus. The surgeon's left-hand port is to the right and just inferior to the xiphoid. The surgeon's right-hand port is 10 cm to the left of the xiphoid below the costal margin and is 10 mm in diameter to permit passage of an SH needle. Another port is placed 15 cm from the xiphoid, beneath the right costal margin as a liver retractor. A final port for the assistant's instrument is placed midway between the laparoscope and liver retractor ports. The surgeon then stands between the patient's legs and the bed is placed in steep reverse Trendelenburg position. The assistant stands to the patient's right and a dedicated camera operator sits on a stool to the patient's left.
Dividing the gastrohepatic omentum
The liver retractor is placed allowing visualization of the hiatus. We first attempt gentle reduction of hernia contents (Fig. 1). Caution must be taken as traction injuries are the most common cause of gastroesophageal perforation during foregut surgery. 9 If the hernia contents do not reduce easily, further attempts at immediate reduction are abandoned. Instead, dissection of the hernia sac is initiated. The lesser sac is entered through the gastrohepatic omentum using an energy device. The gastrohepatic omentum is divided cephalad toward the right crus while identifying and preserving a large replaced left hepatic artery if present. Once the right crus is encountered, the hernia sac is divided, gaining entrance to the plane between the sac and the crus (Fig. 2). This allows carbon dioxide into the space exterior to the hernia sac and aids in its reduction. The hernia sac should not be denuded from the crural muscle. The remaining hernia sac on the crural mechanism will be incorporated into the hiatal closure to ensure a robust repair.
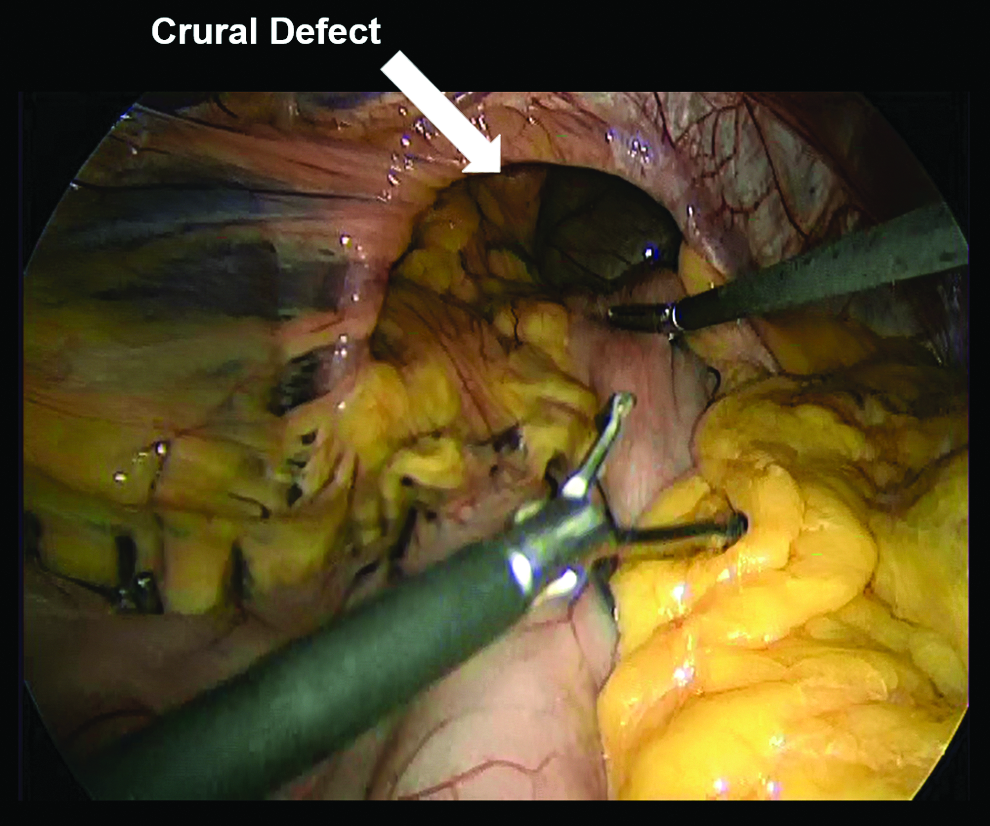
Following liver retractor placement, a large hiatal defect is appreciated. Gentle traction is used to reduce as much of the hernia as possible before beginning dissection of the hernia sac.
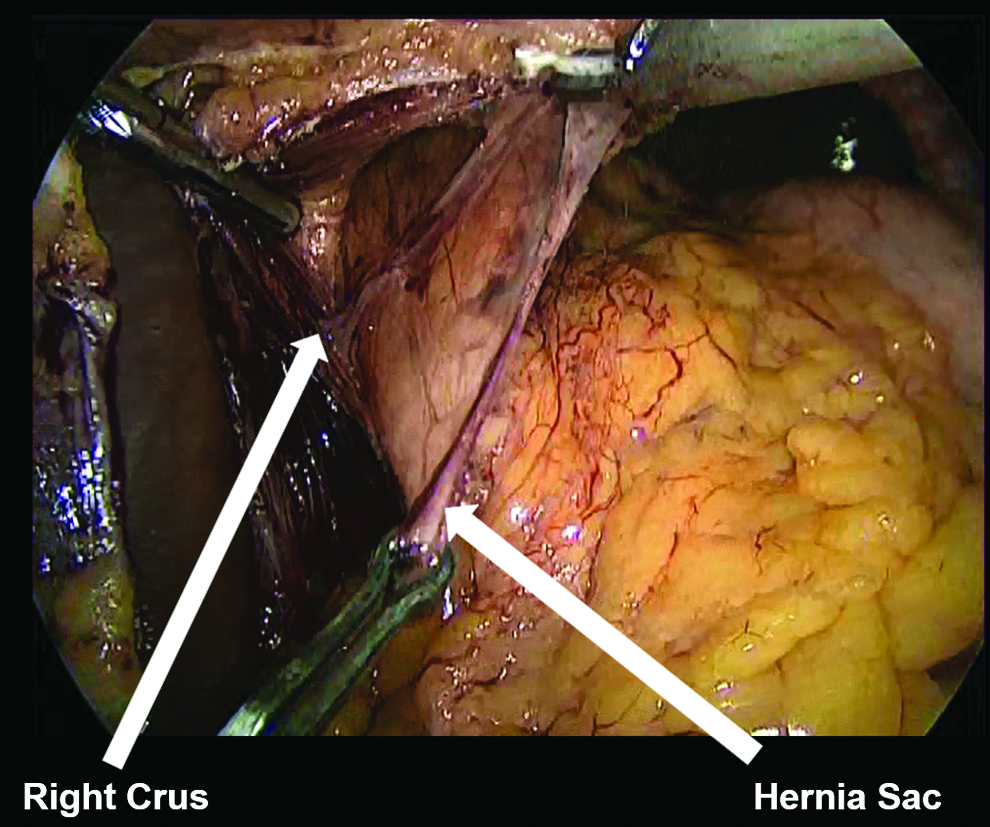
The hernia sac is divided from the crus at the hiatal inlet. The assistant applies downward traction on the sac as the surgeon continues the dissection anteriorly.
Dissecting the anterior hernia sac
Utilizing blunt dissection, the anterior intrathoracic hernia sac is mobilized toward the abdomen. This is accomplished using a spreading technique with two blunt graspers while the assistant grasps the free edge of the hernia sac and retracts inferiorly. Generally, the correct plane is avascular. The anterior vagus nerve should now be identified. Care is taken to protect the vagus. Once the vagus is located, small mediastinal vessels encountered may be safely divided with an energy device. The hernia sac is divided at its origin along the anterior two-thirds circumference of the hiatal inlet until the left crus is reached. The surgical assistant provides gentle caudal retraction throughout by grasping the gastroesophageal fat pad or the hernia sac itself.
Dissecting the posterior hernia sac
Once the anterior hernia sac is freed from the mediastinum, the fundus is mobilized. The short gastric vessels and all other lateral gastric attachments are divided using an energy device, with care not to cause thermal injury to the stomach. Division of the short gastric vessels is continued until the base of left crus is reached. The fundus should now be mobile and the posterior EGJ and hernia sac should be visualized easily. The posterior hernia sac is divided and dissected free from the mediastinum using the same technique described above, exercising caution to identify and preserve the posterior vagus nerve. A Penrose drain may be placed around the esophagus for caudal retraction if needed.
Excision of the hernia sac
Once the sac has been adequately freed from its mediastinal attachments, any remaining hernia contents are readily reduced. As much of the hernia sac as possible should be removed to allow for easier esophageal mobilization and closure of the crura.
Esophageal mobilization
Circumferential esophageal mobilization high into the mediastinum is essential to ensure adequate esophageal length. A blunt, two-handed spreading technique is again used to dissect remaining mediastinal attachments from the esophagus. The vagus nerves should be left intimately associated with the esophageal wall. The mobilization continues high into the mediastinum until there are at least 2–3 cm of intra-abdominal esophagus or anatomic constraints prevent further cephalad dissection. Pleural tears resulting in a capnothorax may occur during this portion of the procedure. They are seldom symptomatic. If a pleural tear is suspected, the anesthesiologist should be informed. In the unusual circumstance that a patient develops any physiologic sequelae from a pleural tear, the pneumoperitoneum pressure should be decreased or the abdomen temporarily desufflated. The anesthesiologist may increase ventilator pressures as needed, but placement of a chest tube should rarely, if ever, be necessary.
Esophageal lengthening
The length of the intra-abdominal portion of the esophagus is then measured with no caudal retraction applied to the EGJ. If the location of the EGJ is unclear, endoscopy is performed to visualize the squamocolumnar junction. If the esophagus is maximally mobilized and there is less than 2–3 cm of abdominal esophagus, an esophageal lengthening procedure must be performed. Several techniques for accomplishing this have been described. A modified Collis gastroplasty is preferred and performed by wedge fundectomy. 10 A 40 or 50 French Maloney dilator is passed along the lesser curvature of the stomach. A marking suture is placed along the left side of the dilator on the stomach at the point that will result in 3 cm of intra-abdominal esophagus/neoesophagus. The surgeon's right-hand port is upsized to pass a laparoscopic linear stapler. The stapler is maximally articulated to the patient's right side, while the fundus is retracted caudally. The stapler is fired sequentially from the proximal fundus toward the marking suture (generally two or three times) until it abuts the dilator. The partially divided fundus is then retracted cephalad and the stapler fired along the left side of the dilator toward the angle of His until a wedge of fundus is transected and a thin gastric sleeve (or neoesophagus) is created based on the lesser curvature. The specimen is placed in an extraction bag for removal. The staple line is then assessed for leaks by insufflating air into the esophagus with the endoscope while it is submerged in saline.
Closure of the hiatus
In most instances, the crura can be reapproximated directly with interrupted 0 or 2-0 braided polyester suture. The closure begins posteriorly, 1 cm above the crural junction. Intact crural fascia should be included with these suture bites. Sutures are added at 1-cm intervals until the crura barely touch the wall of the empty esophagus. At least one anterior crural suture is placed to stimulate scar tissues in this location, helping prevent anterior hernia recurrence. Additional anterior sutures may be needed if posterior sutures excessively angulate the esophagus.
The difficult hiatus
Both axial tension and radial tension are important factors that contribute to hernia recurrence. Axial tension is reduced by adequately mobilizing the esophagus and/or performing a Collis gastroplasty as needed. Radial tension is dependent on both the width and configuration of the hiatal defect. 11 If there is undue tension on the crural closure, the pneumoperitoneum pressure is decreased. If prohibitive tension remains, a diaphragmatic relaxing incision is added to the procedure. Both right and left relaxing incisions have been described. 12 We prefer a right-sided release. An energy device is used to make a full-thickness incision parallel to, but at least 1 cm from, the inferior vena cava. The incision begins at the midpoint of the crus and is carried anteriorly, curving medially at the apex of the hiatus. Following the incision, the crura are closed as described above (Fig. 3). This technique results in a 46% reduction in tension on the crural closure. 11 The use of mesh in hiatal closure remains controversial. Mesh use results in fewer hernia recurrences at 6 months than primary crural closure; however, this difference disappears at 5-year follow-up. 13 Permanent mesh may be associated with postoperative dysphagia, erosion, and stricture formation and should therefore not be used in proximity to the esophagus at the hiatus.13–16 Mesh is used only when a relaxing incision is performed. When needed, a U-shaped piece of slowly degrading bioabsorbable mesh is placed with the base posterior to the esophagus. The right limb is oriented so that it covers the relaxing incision defect. The mesh is secured in place at the corners with polyester sutures and further affixed to the diaphragm with fibrin glue.

The completed relaxing incision with posterior crural closure.
Fundoplication
The type of fundoplication used is determined by the patient's symptoms and manometry. If the patient had dysphagia or poor esophageal motility on preoperative manometry, a partial wrap is used (either a Toupet or Dor). A Nissen fundoplication is performed for all other patients (Fig. 4). If gastroplasty was used, the fundoplication should cover as much of the staple line as possible.

The anatomy at completion of the procedure. The fundoplication is made over 2–3 cm of intra-abdominal esophagus and a bioabsorbable mesh is oriented to cover the defect created by the relaxing incision.
Desufflation and postoperative care
Ports are removed under direct visualization and the abdomen is desufflated. The patient is started on scheduled ketorolac, antiemetics, and kept nil per os on the evening of surgery. An esophagram is obtained on postoperative day one only if the patient had a lengthening procedure, significant pain, dysphagia, or emesis in the perioperative period. All other patients are started on a clear liquid diet on the morning of postoperative day one and advanced to a mechanical soft diet for lunch. Patients are discharged home that afternoon if they are able to tolerate a soft diet. Patients are instructed to remain on a soft diet for at least 2 weeks postoperatively, at which time dietary restrictions may be liberalized. A barium swallow is routinely performed at 6–12 months after surgery to assess the anatomic integrity of the repair. Patients who had a lengthening procedure should be placed on a proton pump inhibitor and have an upper endoscopy within a year to screen for esophagitis. Additional testing may be performed as dictated by patient symptomatology.
Outcomes
Adhering to the above technique has resulted in substantial symptom improvement or resolution for patients treated at our institution. We have previously published retrospective data demonstrating complete symptom relief in 66% of patients as well as significant improvement in patient-reported heartburn, regurgitation, chest pain, dysphagia, and respiratory symptoms at 2-year follow-up. 17 Additionally, our patients had a decrease in proton pump inhibitor use from 90% to 35%. In our series, there was no perioperative mortality, morbidity was rare, and reoperation was necessary in less than 2% of patients.
Conclusions
Laparoscopic paraesophageal hernia repair is a challenging operation that should only be performed by surgeons who are experienced in laparoscopic foregut surgery. Laparoscopic repair is associated with better outcomes compared with open repair, as measured by overall complication rates, hospital length of stay, cost, and readmission rate. 18 Multiple series have demonstrated that laparoscopic repair improves patient symptoms, including heartburn, regurgitation, chest pain, dysphagia, dyspnea, and overall quality of life.17,19 Despite the superiority of laparoscopic repair, the long-term hernia recurrence rate exceeds 50% even in high-volume centers. 20 This high rate of anatomic recurrence is likely a function of both tissue tension and inherent mechanical weakness of the hiatal structures. Fortunately, the majority of these recurrences are minimally symptomatic, with less than 5% of patients requiring reoperation in most series. 21 A safe technique for paraesophageal hernia repair has been described that offers patients a significant and durable improvement in symptoms. 17 Despite over 20 years of surgical experience performing laparoscopic paraesophageal hernia repairs, there remain several technical controversies, which may see the best method of repair change as the field continues to evolve.
Footnotes
Disclosure Statement
No competing financial interests exist.