
Abstract
Abstract
Background:
Although liver cirrhosis with portal hypertension (PH) contributes significantly to morbidity and mortality in abdominal surgery, many authors still consider this disease as an indication for surgery. In many reports, however, numerous treatment modalities focus on hypersplenism secondary to PH, irrespective of splenomegaly and PH. The proven benefits of laparoscopy seem especially applicable to patients with this complex disease. This study evaluates the safety and efficacy of laparoscopic perisplenic artery ligation (SAL) in patients with hepatobiliary disease and PH.
Methods:
From July 2004 to May 2012, the medical records of all patients with hepatobiliary disease in the context of PH at the authors' institutes, including patient demography, operative outcomes, and change of liver function, were retrospectively reviewed.
Results:
A total of 101 patients were included in the series: 85 patients with cirrhotic Child A, B class, who underwent no intervention (Control group n = 22), splenectomy (SP group n = 29), laparoscopic SAL (SAL-1 group, n = 34) for splenomegaly, and 16 patients with cirrhotic Child C class, who only underwent laparoscopic SAL (SAL-2 group, n = 16). Among these patients, both laparoscopic SAL and open SP for splenomegaly were available to decrease morbidity rate, loss of bleeding, and improve liver function, whereas laparoscopic SAL had a lower rate of surgical-related complications.
Conclusions:
Although technically challenging in patients with hepatobiliary disease coexisting with PH, the present series demonstrated the safety and feasibility of laparoscopic SAL, even facilitating simultaneous surgery for hepatobiliary diseases, with a clear advantage over SP and no intervention.
Introduction
H
In the past two decades, operative skills and techniques have improved, and many series have reported success with surgery in selected patients with cirrhosis despite higher morbidity and mortality rates. However, most of these reports focused on the feasibility of surgery in patients with abdominal disease and liver cirrhosis, and only a few studies investigated the effect of relieving PH on the prognosis of patients with PH and liver cirrhosis.4,5 It is well known that splenic artery ligation (SAL) or splenectomy (SP) are used to decompress PH in living-related donor liver transplantation, and these procedures were determined to attenuate the injury from portal overflow.6,7 This study was designed to investigate whether SAL or SP benefits the surgical procedure and prognosis in patients with hepatobiliary disease coexisting with PH. 8
Patients and Methods
From July 2004 to May 2012, all patients with hepatobiliary diseases and PH who underwent surgery were selected for retrospective medical record review. The presence of preoperative PH was evaluated retrospectively and was indirectly defined as (1) esophageal varices detected by endoscopy or upper gastrointestinal barium meal and (2) splenomegaly (major diameter >12 cm) with a platelet count of <100 × 109/L according to the Barcelona Clinic Liver Cancer group criteria. 9 Splenic size was accurately measured perioperatively by either abdominal computed tomography and ultrasonography or intraoperative measurement using an umbilical tape and ruler. According to a previous study, 10 the normal spleen weighs 150 to 200 g and has a craniocaudal length shorter than 12 cm; splenomegaly refers to > 600 g of spleen and longer than 15 cm in craniocaudal length. Spleens weighing >1000 g with a craniocaudal length longer than 20 cm were classified as massive, those weighing >1600 g with a craniocaudal length longer than 22 cm were classified as supramassive splenomegaly.
A total of 145 patients with hepatobiliary disease (hepatic carcinoma, cholelithiasis, and hepatolithiasis) and PH, who underwent surgery in the authors' institutes, were retrospectively reviewed. For all of these patients, different surgical procedures were provided for hepatic carcinoma, hepatolithiasis, or cholelithiasis, whereas for coexisting PH or splenomegaly, there were three treatment modalities: SP, laparoscopic peri-SAL, or no intervention. Whether SP, SAL, or no intervention was performed depended on author's or patients' preference. All of the surgical procedures were performed as previously described.3,4,8,11,12 The criteria for exclusion were as follows: 44 patients with platelets < 30 × 109/L, spleen weight >2000 g, or preoperative esophagus varices bleeding were excluded because of a lack of matched cases. For patients with platelets >30 × 109/L and cirrhotic Child–Pugh class A or B, the adopted treatment for PH included no intervention (Control group, n = 22), splenectomy (SP group, n = 34), and SAL (SAL-1 group, n = 29). In addition, 16 patients with cirrhotic Child C class who underwent only SAL to PH were classed as SAL-2 group (n = 16). The patient demographics, procedure performed, estimated blood loss, operating time, hepatobiliary pathology, intraoperative and postoperative complications, length of postoperative hospital stay, liver function, and the incidence of portal vein thrombus (PVT) 3 months after surgery were reviewed among the four groups.
Surgical procedure
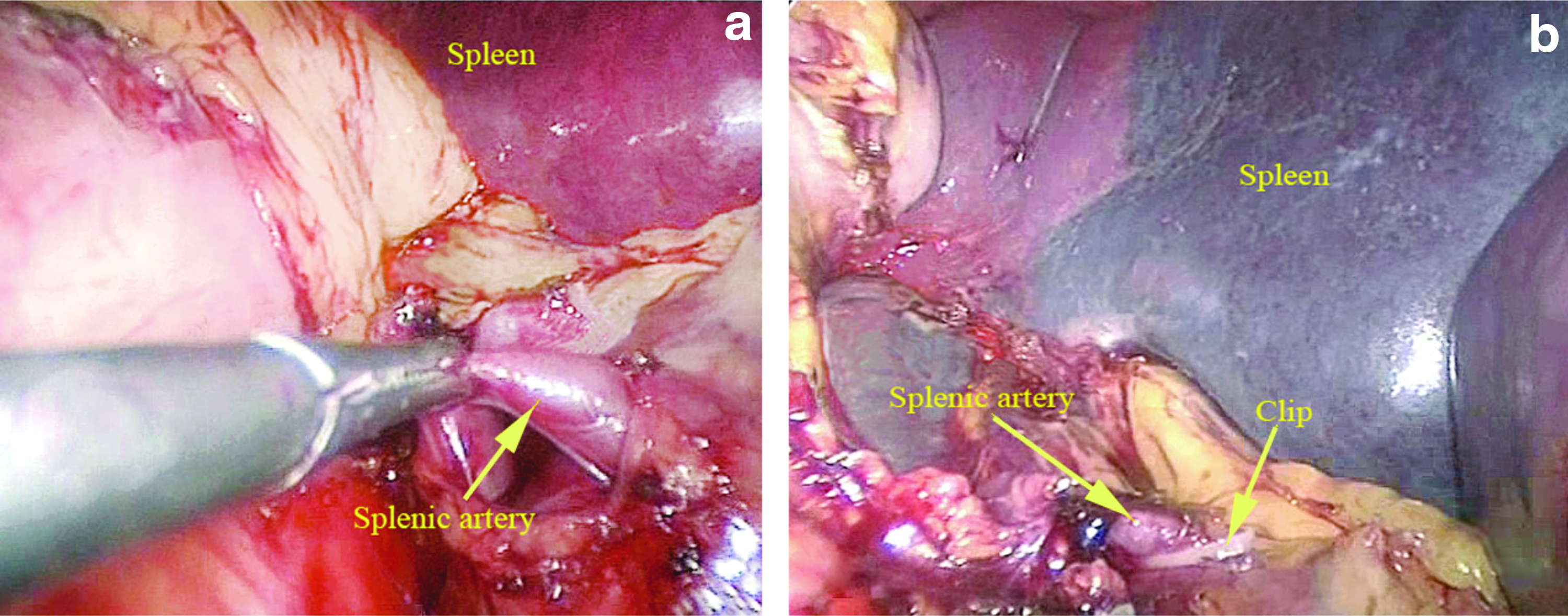
The operation was performed under general anesthesia with endotracheal intubation by an experienced hepatobiliary surgeon. Intraoperative ultrasonography was routinely used. In all patients, platelets (10 to 20 U, depending on the platelet count < 50 × 109/L) were infused when anesthesia was started. In the SP group, concomitant SP was performed immediately after exploring the abdomen in open mode. In laparoscopic SAL, the short gastric artery, splenic artery, and other collateral artery supplying the spleen were divided and ligated in laparoscopy as close to the splenic hilum as possible until the whole spleen became dark (Fig. 1). Subsequently, hepatobiliary surgery was performed through an open or laparoscopic approach according to standard procedures. We performed SAL laparoscopically even when subsequent hepatobiliary procedures were done by open surgery because (1) the incision for open hepatobiliary procedures is usually not liable to perform SAL, (2) for supramassive splenomegaly, the spleen is severely adhered with the surrounding tissue, and the operation space for open surgery is limited, which is difficult to separate the spleen and vessels and easy to damage spleen and pancreatic tail, causing bleeding and pancreatic fistula, and (3) laparoscopic surgery can provide a sweeping view and wide space, which is easy to operate under direct vision with minimal injury and less bleeding. The abdomen was closed after placing soft drains around the transected liver surface. In the SP group, drains were also placed near the pancreatic tail. Complete peripheral blood count and liver function tests were checked on postoperative days 1, 3, and 7.
Splenic artery dissection
Follow-up
After the patients were discharged from the hospital, they were followed up at the outpatient clinic every month for the first 3 months. Complete peripheral blood count and liver function tests were examined. Routine ultrasound examination for PVT was performed on first week, 1, and 3 months after operation or in the event of clinical signs and symptoms suggestive of thrombosis in the portal system (such as abdominal distension, diarrhea, fever, abdominal discomfort or pain, leukocytosis, and nausea) and was confirmed by CT abdomen scan.
Statistical analysis
Continuous data were expressed as mean ± standard deviation and analyzed using t tests. All statistical analyses were performed using SPSS software (version 13.0; SPSS, Inc., Chicago, IL). Values were considered to be significant when P < .05.
Results
Preoperative characteristics and operative outcomes
Except for platelet (PLT) count, no significant differences were found in cirrhotic Child classification, spleen weight, and other characteristics among the Control, SP, and SAL-1 groups; however, between SAL-1 and SAL-2 groups, patient characteristics were not significantly different except for cirrhotic Child classification (Table 1). Nevertheless, blood loss, operative time, blood transfusion rate, and morbidity rate in the SAL-1 group were significantly lower than those in the SP and Control groups (P < .05). Operative mortality was 6.1% (2 patients, 1 hemoperitoneum, and 1 varices bleeding) in patients who underwent SP, and no deaths occurred in the other groups (P = .22) (Table 2). Moreover, patients who underwent laparoscopic SAL-1 had significantly lower morbidity (36.4% versus 27.3% versus 17.3%; P = .04), whereas no significant difference was found between SAL-1 and SAL-2 groups (Table 2).
P1 indicating difference among Control group, SP group, and SAL-1 group; P2 indicating difference between SAL-1 and SAL-2 groups.
SP, splenectomy; SAL, splenic artery ligation; ICG, indocyanine green; COPD, chronic obstructive pulmonary disease; ASA, American Society of Anesthesiologists.
P1 indicating differences among Control, SP, SAL-1, and SAL-2 groups; P2 indicating difference between SAL-1 and SAL-2.
SP, splenectomy; SAL, splenic artery ligation; LC, laparoscopic cholecystectomy; LBDE, laparoscopic bile duct exploration; GI, gastrointestinal.
In the SAL procedure, the spleen is ischemic but not complete. The existence of collateral circulation in pancreatic tail and lienophrenic ligament can make no splenic necrosis. So we did not experience any spleen ischemia-related complication, such as splenic abscess.
Short-term outcomes
SAL and SP decreased portal pressure, and liver function as determined by Child–Pugh class score or the indocyanine green (ICG) retention rate at 15 minutes significantly improved in SAL or SP groups compared with that preoperation, especially for patients in the SAL-2 group with cirrhotic Child C class, whose liver function improved greatly (P < .01) after surgery. However, liver function improvement in the patients with SP was attenuated because of the occurrence of PVT, although the reduction of hypersplenism was significantly better than that in the SAL-1 and SAL-2 groups (P < .01) (Table 3).
P < .05, **<.01, indicating significant difference between preoperation and 3 months postoperation.
WBC, white blood cell; PLT, blood platelet; ICG, indocyanine green; PVT, portal vein thrombus; SP, splenectomy; SAL, splenic artery ligation.
Discussion
Hepatitis B and hepatolithiasis are endemic in East Asia, especially in China. Chronic hepatitis B can cause liver cirrhosis, liver cancer, and cholelithiasis, and recurrent hepatolithiasis can lead to liver cirrhosis.1,2,4,13 Therefore, liver cancer, hepatolithiasis, and cholelithiasis with associated liver cirrhosis or PH are frequently observed in the clinic. Owing to pancytopenia and the development of collateral circulation, this condition was previously difficult to treat medically and surgically. However, with the advancement of surgical skill, many reports have suggested that surgery for these hepatobiliary diseases is reasonable,14–17 but many controversies still surround the patient selection criteria, safety, timing, and treatment modalities for PH in hepatobiliary diseases with coexistent PH.
Currently, most of the literature has focused on secondary hypersplenism and thrombocytopenia, 18 and SP has been suggested for thrombocytopenia. Takayama et al. 7 and Sugawara et al. 3 performed SP in patients whose platelet count was <60 × 109/L, whereas Hanazaki et al. 18 used this procedure in patients whose platelet count was <50 × 109/L. Shimada et al. 6 suggested laparoscopic SP and staged hepatectomy in patients with hepatocellular carcinoma (HCC) and hypersplenism whose platelet count was fewer than 70 × 109/L. In fact, the decrease in platelet count was not always parallel to the degree of splenomegaly, PH, or liver cirrhosis. To the best of our knowledge, there are no reports of patients who died of thrombocytopenia attributed to PH, but PH can increase operation difficulty and damage gut barrier function or cause endotoxin/bacterial translocation, and it was considered that gut-derived endotoxins were causing liver cirrhosis pathogenesis.19,20 Hence, decreasing PH would theoretically be beneficial for decreasing or preventing endotoxin/bacterial translocation and for improving liver function. Takayama et al. 7 and Sugawara et al. 3 demonstrated that SP could alleviate portal vein pressure or portal overflow and improve liver function because serum total bilirubin was significantly reduced after SP. Bruix et al. reported that hepatic venous pressure gradient >10 mmHg should be considered as a contraindication for liver resection, 9 but no investigations were performed that aimed to demonstrate the effect of relieving PH on patient prognosis in individuals with coexisting PH. This study demonstrated that SAL or SP significantly improved the liver function as measured by Child–Pugh class score or ICG retention rate at 15 minutes compared with the preoperation assessments. Potential benefits of decreased portal pressure on improving liver function may be an important factor in successfully recovering from surgery with significantly lower incidences of morbidity and mortality rates in the SAL-1 and SAL-2 groups.
Perioperative bleeding control and postoperative liver failure should be the major concerns in surgery for hepatobiliary disease with coexistent PH. Livers with cirrhosis and PH can be difficult to dissect, especially in patients with a history of upper abdominal surgery or dense adhesions. Many reports have described that perioperative bleeding and the need for transfusion are significantly higher in patients with PH than in those without, and excessive intraoperative bleeding can cause patient mortality.13,15,18,21 Therefore, many authors suggested first performing SP or even concomitant distal splenorenal shunting in some patients with severe PH and a history of upper abdominal surgery or dense adhesions 2 to decrease portal pressure and improve hemostasis before performing “two-stage surgery” 1 week or 1 month later. 8 In the present series, we also demonstrated that simultaneous SAL could decrease blood loss and facilitate the dissection and hemostasis compared with the SP and Control groups.
Hypercoagularity resulting from marked thrombocytosis and blood flow stasis at the stump of the occluded splenic vein may predispose to PVT. However, because of increased resistance within a cirrhotic liver, portal flow remains static within the portal vein, which may result in PVT. This complication more frequently occurs after SP for advanced liver cirrhosis or hematologic disease. The incidence is significantly higher after removal of a large spleen and usually occurred within 30 days after SP.21,22 We also observed that platelet count was remarkably elevated; 15.2% (5/33) of patients in the SP group developed PVT, which was detected with color Doppler ultrasonography or CT, and routine anticoagulation therapy in the early postoperative period was performed. No patients in the SAL-1 or Control groups had postoperative PVT. Some patients may remain asymptomatic, 23 but these complications may be fatal if not treated in a timely manner,24–26 especially in the early stage. In the present SP group, 1 patient died of esophageal varices bleeding, contributing to the presence of PVT and subsequently anticoagulation therapy.
There have been several reports of usefulness of partial splenic embolization (PSE) before hepatic surgery for patients with PH. 27 PSE seems less invasive than SAL. However, the existence of collateral circulation in pancreatic tail and lienophrenic ligament can make no splenic necrosis in the SAL procedure. So spleen ischemia-related complication such as splenic abscess never occurs in SAL cases. Meanwhile, PSE may lead to postembolization syndrome, include daily intermittent fever, abdominal pain, nausea and vomiting, abdominal fullness, and appetite loss, which is hardly inevitable. Also, postoperative splenic abscess is a severe complication. 28 Moreover, PSE needs a “two stage” procedure, which means a subsequent hepatobiliary surgery is needed.
Conclusion
In general, the laparoscopic SAL method, including all perisplenic artery ligated, has several notable benefits. First, a laparoscopic approach minimizes surgical stress without the need for a “two-stage” surgery. Second, improved liver function and increased platelet count are induced by a preceding SAL. Third, it results in less blood loss and no or low incidence of PVT occurrence compared with SP. Consequently, the use of blood products such as fresh-frozen plasma and platelet-rich plasma in the perioperative period is reduced, which can prevent blood-borne infectious diseases. However, the long-term effect of this new surgical strategy on prognosis has never been clarified, and prospective investigation is needed.
Footnotes
Disclosure Statement
No competing financial interests exist.