
Abstract
Abstract
Introduction:
Conditions requiring an esophagectomy and esophageal replacement are rare in children. The preferred method and ideal replacement organ continue to be debated. We present long-term outcomes in children treated with esophagectomy and gastric pull-up.
Methods:
We conducted a retrospective review of all the patients who underwent a esophagectomy and gastric pull-up at two major pediatric institutions from 2004 to 2015. Follow-up data were obtained for children when available, including any postoperative complications, need for dilation of strictures, and current feeding method.
Results:
Minimally invasive procedures were performed on 7 patients (5 female and 2 male) with a median age of 3 years (range 2–20, standard deviation = 8). Three patients successfully underwent laparoscopic transhiatal esophagectomy and cervical gastric pull-up, and three patients successfully underwent combined laparoscopic and right thoracoscopic (Ivor-Lewis) esophagectomy and cervical gastric pull-up. We identified an additional 3 patients who had an open esophagectomy and gastric pull-up. Seven patients had tubularized gastric conduits, six without pyloroplasty and one with pyloroplasty. For those patients with tubularized conduits, the average time to achieve full oral feeds was 16 days, with 1 patient with pyloroplasty who took 27 days. Of the three whole-stomach conduits, one reached oral independence at 19 days and the other two had yet tolerated anything per os. Follow-up data were available for all patients. At the average 5 years follow-up (ranging from 1 month to 7 years), all but two were thriving well with full oral feeds.
Conclusions:
Minimally invasive esophagectomy and gastric pull-up is a good alternative in managing pediatric patients in need of esophagectomy and replacement; it offers acceptable early and long-term outcomes. Tubularized conduit appears to be superior to using the whole stomach and potentially avoids pyloroplasty. Ongoing study is needed to validate our findings.
Introduction
M
Many descriptions in the adult literature, both in laparoscopic and open esophagectomy with gastric conduit, favor construction of a gastric tube rather than use of the entire stomach as a conduit. While the literature remains divided, some authors argue that using a smaller tubularized conduit reduces delayed gastric emptying (DGE). 4 Published series in the pediatric population, however, tend to use a nontubularized conduit. 3
We hypothesized that a tubularized gastric conduit enhances gastric emptying, which may shorten the time to achieve full oral feeds and potentially avoid the need for pyloroplasty. We present long-term outcomes of our case series of esophagectomy and gastric pull-up.
Materials and Methods
Following the institutional review boards' approval at each institution, we conducted a retrospective chart review of patients at two pediatric academic hospitals. Patients 21 years old or younger who underwent esophagectomy with gastric pull-up at either institution from 2004 to 2015 were analyzed.
Demographic, preoperative, operative, and postoperative data, including complications, postoperative complications, and feeding details, were abstracted from the electronic medical record.
Patient identification and selection
Patients were identified by searching the operative logs for procedures, including the keywords “esophagectomy,” “gastric pull-up,” “transhiatal,” or “Ivor-Lewis.” Individual operative logs were reviewed to ensure that the procedure logged was in fact an esophagectomy with gastric pull-up. We excluded patients who underwent different methods of esophageal replacement.
Operative technique
Operative technique was determined by the individual surgeon. All laparoscopic surgeries were performed by a single surgeon and performed using a transhiatal or Ivor-Lewis approach with esophagogastrostomy through a right cervical incision, as previously described by our group.5,6
Results
We identified a total of 19 patients who underwent esophagectomy and esophageal replacement. Nine patients had colon interpositions rather than pull-up and were thus excluded from the analysis. Ten patients (seven female and three male) met our inclusion criteria with a median age of 3 years (range 2–20, standard deviation = 7). Of this cohort, 3 patients had long-gap esophageal atresia, two of whom failed Foker's procedure; 4 patients suffered severe esophageal stricture from caustic ingestion. One of the patients sustained an iatrogenic esophageal injury from a neurenteric cyst removal. One patient had a congenital stricture, and one patient had a severe esophageal dysmotility from achalasia. Of the 10 patients, 7 patients underwent minimally invasive esophagectomy and gastric pull-up with cervical anastomosis. Three of the 7 patients underwent laparoscopic transhiatal esophagectomy, and 4 patients underwent combined laparoscopic and right thoracoscopic (Ivor-Lewis) procedures. One of the patients in the latter group was converted to open due to intense inflammation and scarring. This patient had an iatrogenic tracheoesophageal injury and underwent multiple procedures before the esophageal replacement. Six of the minimally invasive approach patients had the conduits tubularized without pyloroplasty. The patient with iatrogenic injury had a whole stomach pull-up and pyloroplasty due to concern for compromised blood supply. Of the open group, 2 patients underwent Ivor-Lewis procedures and one with a transhiatal technique. The open transhiatal esophagectomy had a tubularized conduit with pyloroplasty. Two open Ivor-Lewis esophagectomies had nontubularized conduits and pyloroplasty. One of these also had a Collis gastroplasty.
The average operative time was 405 minutes (range 339–672) for minimally invasive procedures and 636 minutes (range 473–776) for the open surgeries. There was no intraoperative death or complication. Three patients developed esophagogastric anastomotic strictures requiring balloon dilation ranging from 1 to 8 times.
The average length of stay for the entire cohort was 14.5 days (range 10–37). Jejunostomy tube feedings were started on postoperative day 1 on the patients who successfully underwent minimally invasive esophagectomies and after resolution of ileus on the open patients. Oral intake was initiated after esophagram, which took place on postoperative day number 6 or 7 and advanced as tolerated. The average time it took to achieve full oral feeds for the patients with tubularized gastric conduits was 16 days (range 8–35), while the patient who had both tubularized conduit and pyloroplasty took 27 days. The patient with iatrogenic esophageal injury who had a whole stomach conduit and pyloroplasty never tolerated oral feeds.
Of the 3 patients with nontubularized conduits, one achieved full oral feeds at 19 days and the other two never tolerated anything by mouth.
Follow-up data were available for all patients. At the average 5 years follow-up (ranging from 6 months to 7 years), all but two were taking full oral feeds and thriving well (Fig. 1).
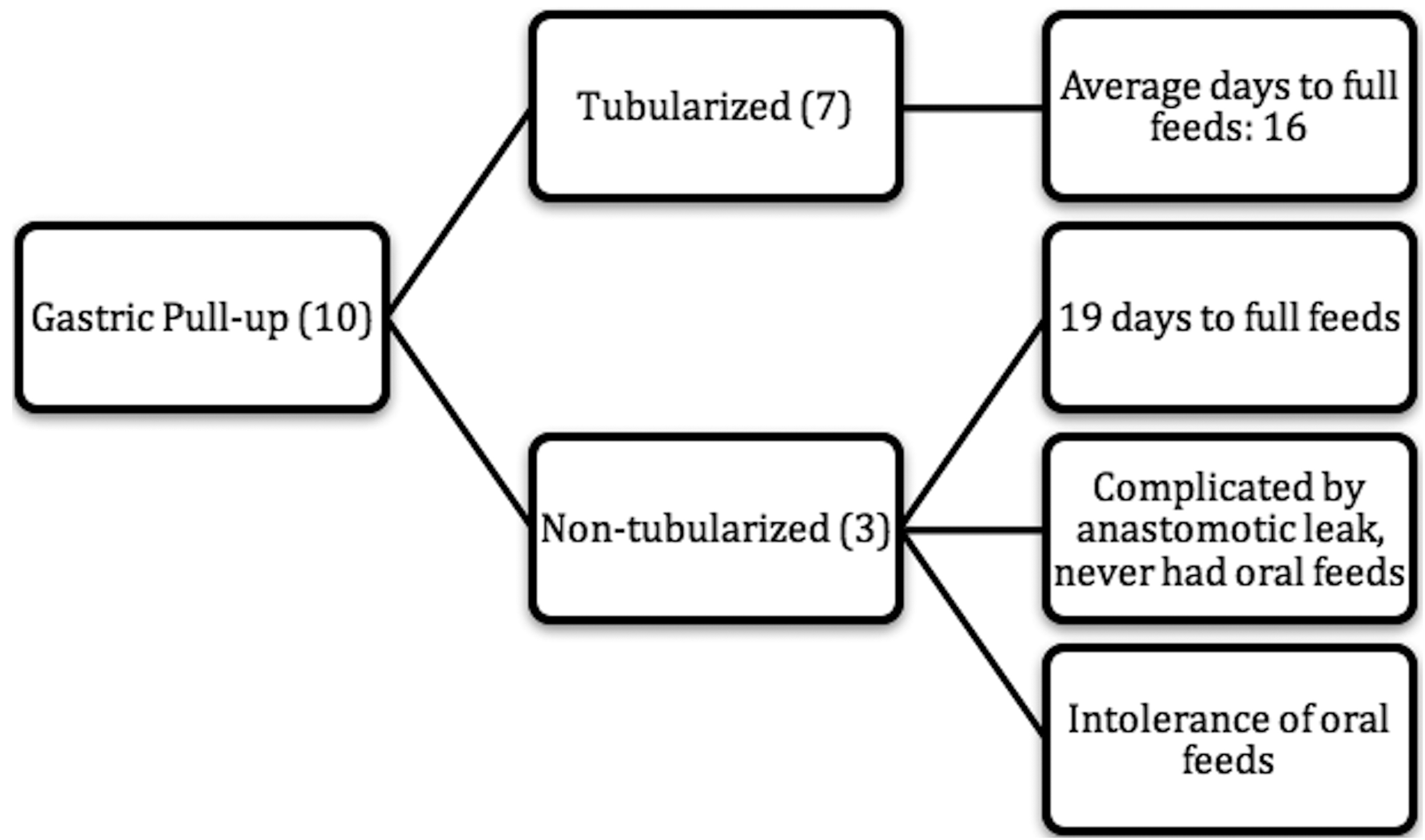
Outcomes of children treated with tubularized or nontubularized gastric conduit after esophagectomy.
Discussion
Minimally invasive esophagectomy with gastric pull-up has gained popularity in children and is considered a safe alternative to open procedure. 6
Shalaby et al. report a stricture rate of 15% and a leak rate of 11%, 7 whereas Parilli et al. report no strictures, but a leak rate of 40%. 8 The largest pediatric series published to date of 16 patients by Ng et al. shows a stricture rate of 12.5% and a leak rate of 6%. 3 In our series, we have no documented leaks. However, we notice a 42% stricture rate among the minimally invasive approach patients. This result is comparable to reported series. All of them were treated successfully with balloon dilation.
Although the preferred gastric conduit in adults is still debated in the literature, many have demonstrated excellent outcomes with tubularized gastric conduits without pyloroplasty. 9 A meta-analysis of these studies by Akkerman et al. 9 showed that tubularization results in significantly decreased DGE (relative risk 0.34; 95% confidence interval (95% CI) 0.12–0.97). Pyloroplasty did not improve DGE in tubularized or in whole stomach (relative risk 0.91; 95% CI 0.57–1.43). Most of the pediatric published series report on using the whole stomach with or without pyloroplasty.3,7,8,10
Unlike adults, the literature on tubularized gastric conduit in pediatric population is limited. To our knowledge, Kane and his associates are the only other group to report using tubularized conduit in the pediatric population. 11 We favor the tubularized conduit because we feel that it enhances gastric emptying. Of the 7 patients with this method of replacement, only 1 patient had a pyloroplasty. The average time to achieve full oral feeds in this group was 16 days, with the 1 patient with pyloroplasty achieving oral independency at 27 days. Of the 3 patients with a whole stomach conduit, only one is currently able to tolerate full oral feeds. It is possible that these 2 patients who have nontubularized conduits and pyloroplasty have concurrent medical problems that influence their ability to tolerate oral intakes. The patients with tubularized conduit without pyloroplasty fared as well or better than published reports regarding the time it took to achieve oral independency.
Although our analysis is one of the largest series utilizing the tubularized gastric conduits, it has several limitations because of the retrospective nature of the study and a small number of patients. Furthermore, the study is composed of a heterogenous group of patients. This heterogeneity may lead to different responses to surgery and, therefore, may not provide consistent outcomes.
Conclusions
Minimally invasive esophagectomy with gastric conduit is safe and provides a good alternative approach in pediatric population who require an esophageal replacement. A tubularized conduit seems to enhance gastric emptying and potentially avoid the need for a pyloroplasty. However, a randomized study is needed to validate that tubularization is superior to a pull-up using the entire stomach.
Footnotes
Acknowledgments
The authors thank the Department of Pediatric Surgery at Children's Hospital Los Angeles and the Department of Pediatric Surgery at Miller Children's Hospital, Long Beach Memorial Medical Center.
Disclosure Statement
No competing financial interests exist.