
Abstract
Abstract
Purpose:
Portal venous system thrombosis (PVST) is a common and potentially life-threatening complication of splenectomy for portal hypertension due to cirrhosis.
Methods:
A meta-analysis was conducted to study the necessity of pharmacologic prophylaxis of PVST after splenectomy and how to select the feasible treatment method. Articles were searched through the PubMed, EMBASE, Cochrane Library databases, and CNKI.
Results:
Overall, 404 articles were initially identified, and 11 of them were eligible. Among these selected articles, 7 articles were associated with the necessity of anticoagulation for prevention of PVST, while 5 were about the drug selection. We first demonstrated that the incidence of PVST after splenectomy was significantly lower in patients who received the preventive measures than in those who did not (odds ratio [OR]: 0.22, 95% confidence interval [CI]: 0.13–0.39, P < .00001). Then, we compared the new-style treatment with the conventional treatment and found that patients with new therapy method had lower incidence of PVST than those who received conventional treatment (OR: 0.37, 95% CI: 0.27–0.51, P < .00001). Also, some studies (n = 4) reported that early and combination use of anticoagulation drugs can lead to better outcome for patients with splenectomy and devascularization.
Conclusion:
Preventative use of anticoagulant drugs might decrease the incidence of PVST after splenectomy in patients with portal hypertension, new anticoagulant drugs such as low-molecular-weight heparin should be used, and early or combination use of anticoagulation drugs might lead to lower PVST incidence for patients.
Introduction
P
Previous studies demonstrated that the prevention using anticoagulant drugs might decrease the incidence of PVST after splenectomy in patients with portal hypertension. 10 However, the selection of anticoagulation drugs had no universal standard; this lead to the large scope incidence of PVST, and our study aims to conduct the systematic review and meta-analysis for drug selection and hope to find better treatment methods for patients after splenectomy with gastroesophageal devascularization for portal hypertension due to cirrhosis.
Materials and Methods
This work was based on the PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions. 11
Strategy of article collection and selection criteria
We performed the literature search through the PubMed, EMBASE, Cochrane Library databases, and CNKI (the latest date was August 30, 2016). Our search items were according to the previous meta-analysis. 10
Our criteria for selecting the eligible articles were as follows: (1) by the items (rct [ALL Files] or randomized control trial [ALL Files] or randomized controlled trial [ALL Files] or controlled trial [ALL Files] or cohort [ALL Files] or case control [ALL Files]). (2) Any duplicates were excluded; those articles related to animal studies, reviews, comments, editorials, and case reports were excluded. (3) Articles that were not associated with PVST after splenectomy or drug prevention for PVST after splenectomy were excluded. (4) Studies that were associated with all patients selected for receiving the anticoagulant drug treatment after splenectomy were excluded. (5) There was no restriction of publication date, publication language, or publication status.
Data selection
Following data were extracted into tables, including the author, journal, publication year, study design, study population, region where a study was conducted, period of enrollment, type of surgery, and number of patients. We also extracted the methods of drug treatment, number of subgroup patients, and patients who suffered with PVST from each selected article.
Evaluation of study quality
The evaluation of randomized controlled literature was referred to the JADAD score standard table. 12 The scoring method included the following: whether random allocation method was correct; whether randomization was hidden; whether the study of object was by blind method; and whether the situation is out of the experiment and follow-up description was missing. When the score was less than 2, it was assigned as a low quality document, while a score of more than 3 was determined to be a high-quality paper. The evaluation of nonrandomized controlled literature was referred to scoring criteria of methodological index for nonrandomized studies. 13 Studies with score more than 10 were referred as the high-quality articles. Study quality was independently assessed by two authors. When there were any disagreements, the consensus was made by discussing with each other. Both randomized control trials and nonrandomized control studies were selecting the high-quality articles.
Statistical analysis
We used the Revman 5.3 software provided by the Cochrane collaboration for meta-analysis. Count data were measured by relative risk (OR value) and 95% CI; quantitative data were measured by the weighted mean differences or standardized mean differences and 95% CI. No statistical difference was found when 95% CI was 1. While statistical difference was found when 95% CI was >1 or <1, mean P < .05. Before the data was merged, heterogeneity inspection was conducted; the experimental results of the heterogeneity analysis used the chi-square test, if P > .1 or I2 ≤ 50%, mean heterogeneity effect of the merged quantity is small, and the fixed-effects model can be used for meta-analysis, while showing large heterogeneity of combining effect of the amount, should be changed for random-effects model analysis. Funnel plots were used for the assessment of publication bias.
Results
Overall, 404 articles were selected from the PubMed, EMBASE, Cochrane Library databases, and CNKI. Also, by excluding duplicates, animal studies, reviews, comments, editorials, and case reports, there were 102 candidates remaining. Further by removing the articles which were not according to our research direction, 11 articles were included in our meta-analysis (Fig. 1). These included studies were published in full texts between 2000 and 2016; of them, four were randomized clinical trials14–17 and seven were prospective or retrospective cohort studies3,6,7,18–21 (Table 1). These studies were conducted by the investigators from Canada (n = 1), China (n = 8), and Japan (n = 2). All patients of these studies suffered from liver hypertension and liver cirrhosis. The information regarding the eligibility criteria of patients, prevention time, and prevention methods is summarized in Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/lap). Patient's characteristics of included studies and all results for prevention of PVST are summarized in Supplementary Table S2. Among these studies, anticoagulants were used in eight studies, thrombolytics in two studies, and prostaglandin E1 in one study.
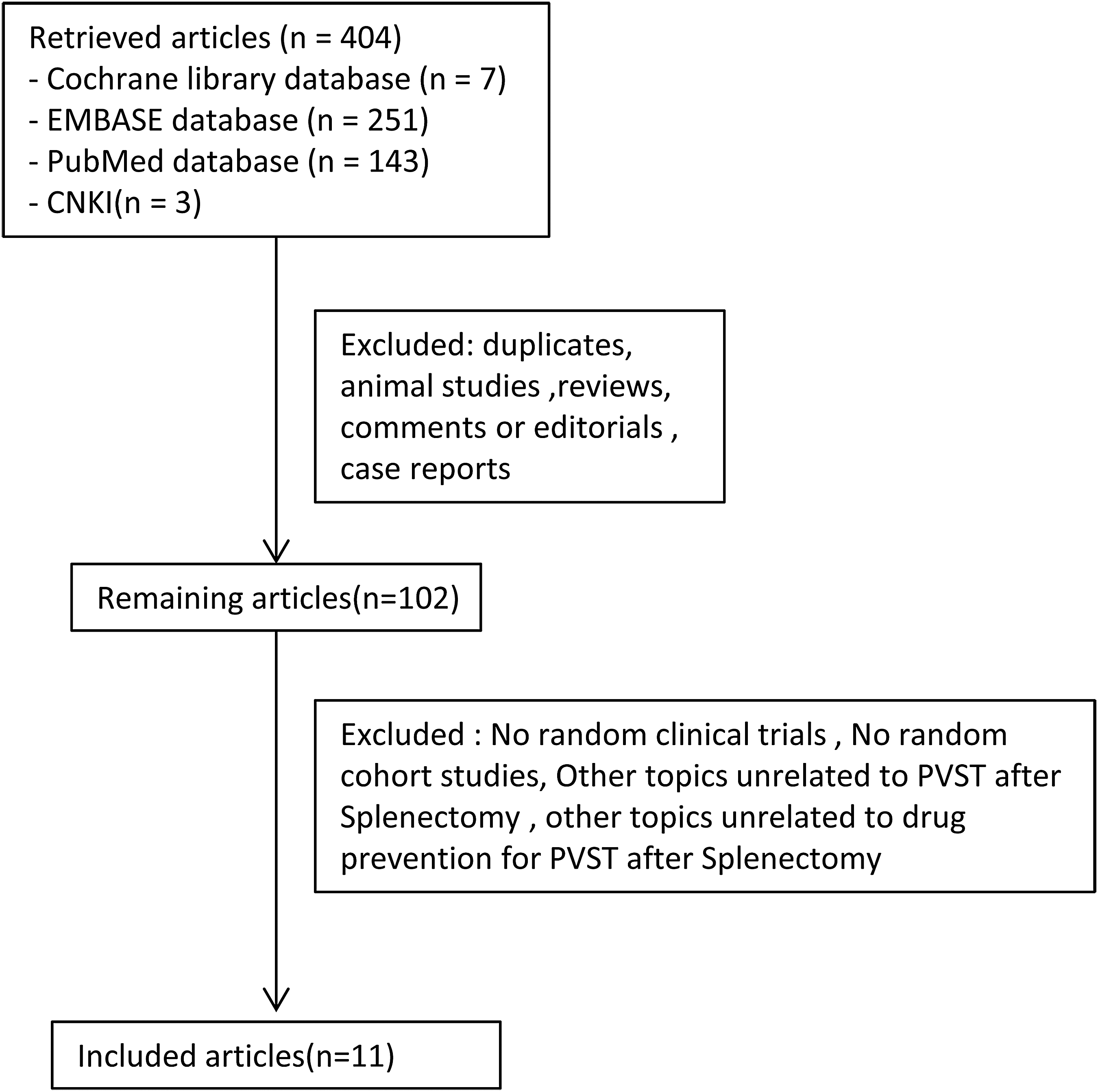
Flowchart of study inclusion.
LC, liver cirrhosis; PH, portal hypertension; RCT, randomized controlled trial.
Study quality
Randomized studies
JADAD score was used for quality assessment of randomized studies. Articles by Wang et al., 14 Ma et al., 15 Xue et al., 16 and Jian and Lin 17 were quantified as the score standard, and all articles were corresponding to RCT criteria (Supplementary Table S3).
Nonrandomized studies
The quality assessment of nonrandomized studies was done by methodological items for nonrandomized studies; the score was graded according to the 12 items. All the seven articles eligible for the criteria are listed in Supplementary Table S4.
Prevention using anticoagulant drugs in the incidence of PVST
Among these 11 selected articles, 7 articles study the clinical efficiency of anticoagulation drugs for the prevention of incidence of PVST after splenectomy between patients who received the anticoagulant drug treatment and those who did not. Heterogeneity among studies was confirmed, and there was no statistical difference (I2 = 46%, P = .10). A fixed-effect model was used, and the pooled OR was 0.22 (95% CI: 0.13–0.39, P < .00001; Fig. 2), suggesting a significantly lower incidence of PVST after splenectomy in patients who received the preventive measures. Funnel plots reveal that there exists some publication bias among these articles (Fig. 3). We believe the reason for such situation may be according to the small sample size in some of the articles, such as Wang et al. 14
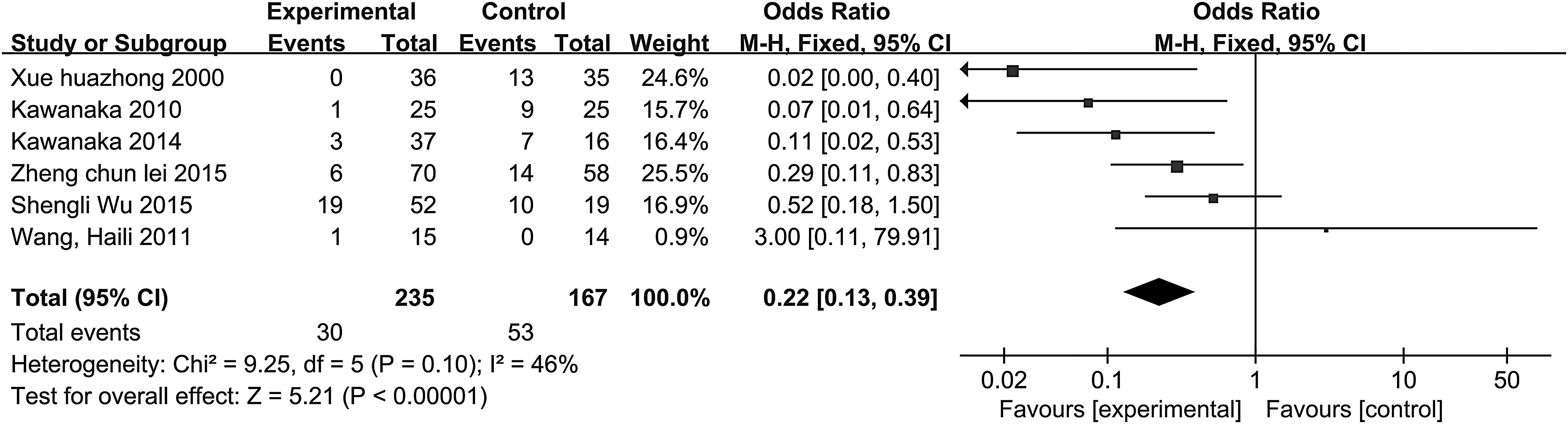
Forest plots showing the results of meta-analysis comparing the incidence of PVST after splenectomy between patients who received the anticoagulant drugs and those who did not. PVST, portal venous system thrombosis.
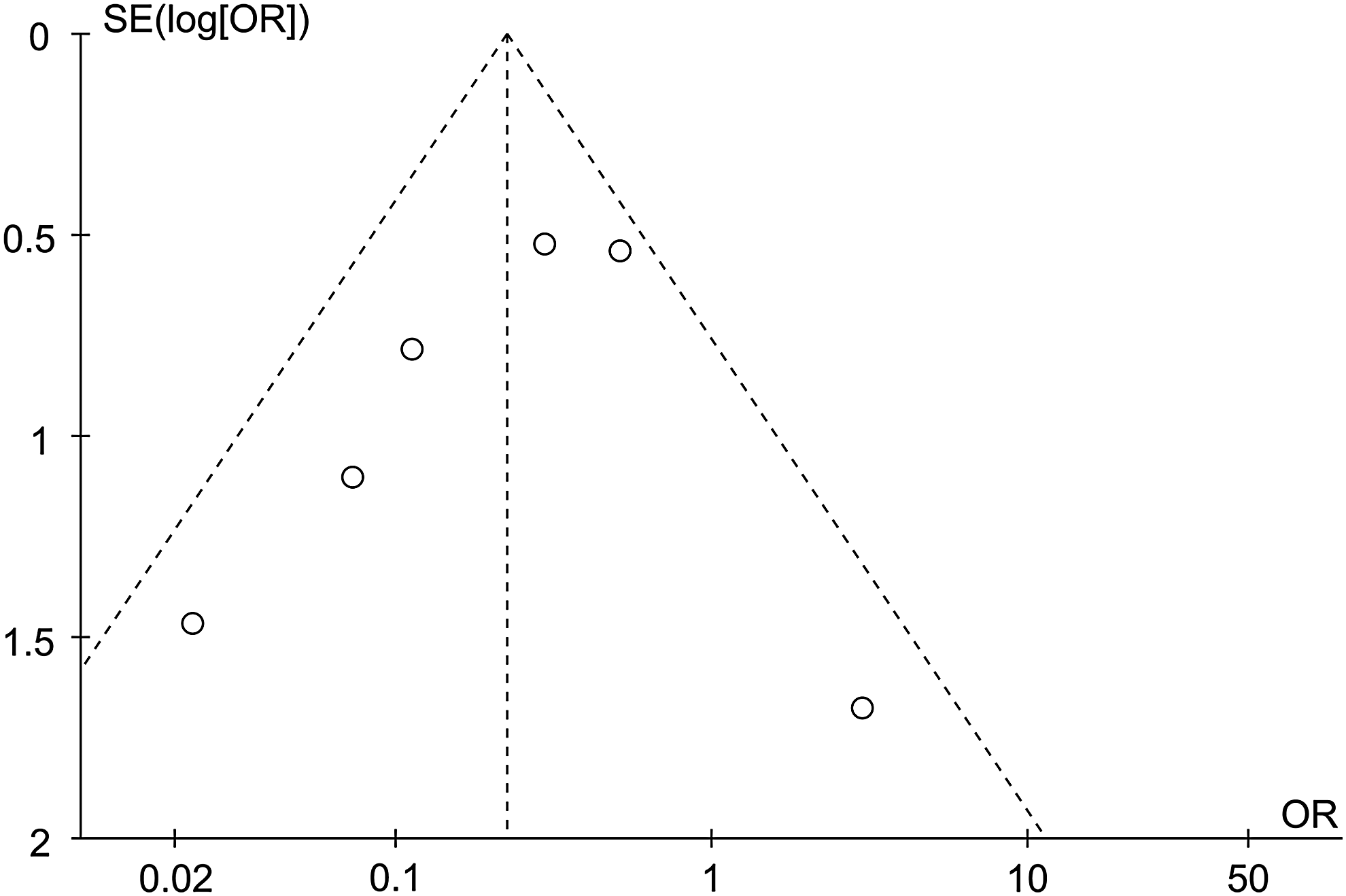
Funnel plot to explore the publication bias in the meta-analyses comparing the incidence of PVST after splenectomy between patients who received the anticoagulant drugs and those who did not. PVST, portal venous system thrombosis.
New therapy versus conventional therapy in the incidence of PVST
Another five articles aim to research efficiency of different anticoagulation drugs for prevention of incidence of PVST after splenectomy. Our study defined those who were using single low-molecular dextran or aspirin, or irregularly using anticoagulation drugs were categorized as using conventional therapy, while those who were regularly using low-molecular-weight heparin (LMWH) and additional drugs aspirin or warfarin, or using prostaglandin E1, antithrombin III were categorized as using a new therapy. Then, we analyzed the data from these five articles and found that heterogeneity among studies was not significant (I2 = 0%, P = .84). A fixed-effect model was used for analysis, and the pooled OR was 0.37 (95% CI: 0.27–0.51, P < .00001) (Fig. 4), suggesting a significantly lower incidence of PVST after splenectomy in patients who received the new therapy. Funnel plots analysis was conducted and the results demonstrated that all these studies were within 95% CI; such consequence suggested that there was no proof for the existence of publication bias (Fig. 5).
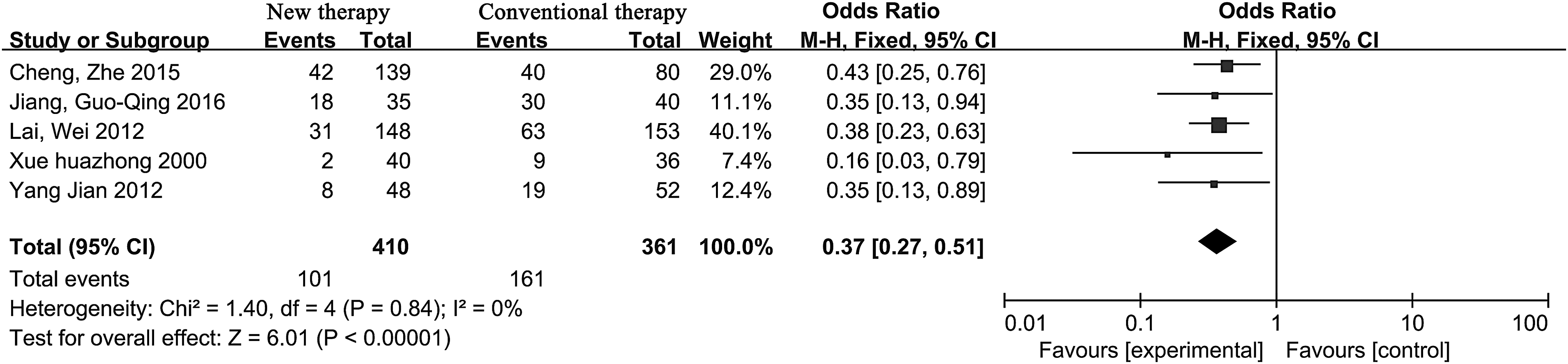
Forest plots showing the results of meta-analysis comparing the incidence of PVST after splenectomy between patients who received the new therapy method and those who received the conventional therapy; the new therapy included the regular usage of LMWH and additional drugs aspirin or warfarin, or using prostaglandin E1and antithrombin III, and the conventional therapy included the usage of aspirin and low-molecular dextran or irregular usage of anticoagulant drugs. LMWH, low-molecular-weight heparin; PVST, portal venous system thrombosis.

Funnel plot to explore the publication bias in the meta-analyses comparing the incidence of PVST after splenectomy between patients who received the new therapy method and those who received the conventional method. PVST, portal venous system thrombosis.
Subgroup analysis according to the method or time of drugs used for the prevention of PVST
In the subgroup analysis of our study comparing regular usage of LMWH and warfarin or aspirin with irregular usage, the pooled OR was 0.38 (95% CI: 0.23–0.63, P = .0002; Supplementary Fig. S1), suggesting that the regular usage of LMWH and warfarin or aspirin can decrease the incidence of PVST after splenectomy.
In the subgroup analysis of our study comparing the combination of LMWH and low-molecular dextran with LMWH alone, the pooled OR was 0.11 (95% CI: 0.01–1.02, P = .05; Supplementary Fig. S2), suggesting that a combination of LMWH and low-molecular dextran may come to better result; further studies are needed to verify by large sample.
In the subgroup analysis of our study comparing early usage of anticoagulation drugs with later usage, the pooled OR was 0.43 (95% CI: 0.13–1.42, P = 0.17) (Supplementary Fig. S3), suggesting that no statistical difference in the time of prevention; further studies are needed to verify such result.
Discussion
Our systematic review and meta-analysis primarily aimed to compare the incidence of PVST between patients who received the anticoagulant drug treatment for the prevention of PVST after splenectomy and those who did not, and between people who received new anticoagulation method for the prevention of PVST after splenectomy and those who received relative conventional method. Our study found that such drugs of anticoagulants, prostaglandin E1, and thrombolytics could significantly decrease the incidence of PVST after splenectomy. Also, we found that people who received new anticoagulation therapy can have a better consequence. According to the analysis of existing literatures, we found that LMWH, prostaglandin E1, and antithrombin III were considered new anticoagulation drugs, whereas aspirin and low-molecular dextran were conventional drugs. In our review, we found that regular usage of LMWH within the first 5 days after surgery, followed by oral warfarin or aspirin for 1 month was considered efficient for the prevention of PVST.6,7,18,19 Such a method for prevention of PVST was considering the function of these anticoagulation drugs; thus, LMWH can give the best anticoagulant effect in short period, while for a long time of anticoagulation, warfarin and aspirin may have the satisfied result and decrease the risk of bleeding. Also, Jiang et al. 21 found that warfarin can lead to better consequence than aspirin.
Kawanaka et al. 20 found that antithrombin III can lead to satisfied efficiency for the prevention of PVST after splenectomy, and this phenomenon was confirmed by his further research. 3 Kawanaka believed that the decreased antithrombin III (ATIII) activity and large splenic vein diameter (SVD) are the risk factors for portal vein thrombosis after splenectomy in liver cirrhosis with portal hypertension. In his study, he found that when ATIII activity was ≥70% and SVD was <10 mm, treatment was not required for prevention of PVST, whereas when ATIII activity was <70% or SVD was ≥10 mm, the ATIII monotherapy was necessary; however, ATIII combined therapy followed by danaparoid sodium and warfarin was needed when SVD was ≥15 mm or huge hepatofugal collateral vessels was ≥10 mm. Kawanaka et al. gave a new method for prevention of PVST, thus the use of anticoagulation drugs is based on the index of risk factors of PVST after splenectomy. Such treatments can lead to the best result and decrease the side effects of the drugs used.
The major limitation of our study was the small number of studies included in our meta-analysis, which greatly limited the reliability of the findings from the meta-analyses regarding the efficacy of preventive measures and the rational using of anticoagulant drugs after splenectomy. Further studies are needed to confirm the best way to use all kinds of anticoagulant drugs for prevention of PVST after splenectomy for patients with liver cirrhosis and portal hypertension.
Footnotes
Acknowledgment
All the authors contributed equally to this article.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.