
Abstract
Abstract
As the field of minimally invasive surgery rapidly evolves, there is an opportunity to adopt innovative techniques to accommodate a variety of patient populations. In patients with portal hypertension, a major risk factor upon entry into the abdomen is injury to large, engorged paraumbilical vessels in the anterior abdominal wall. Major blood loss often results from just entering the abdomen. Here, we describe a patient with caput medusae secondary to portal hypertension presenting for laparoscopic repair of a ventral hernia. Using ultrasound guidance, initial port placement into the abdomen was performed safely using needle access, Seldinger technique, and serial dilation for VersaStep™ 5 mm port (Medtronic, Minneapolis, MN) insertion. Overall, this innovative technique is a safe and effective method of entry into the abdomen in a patient with portal hypertension.
Introduction
T
Case Report
This is the case of 6-year-old male with a history of living donor kidney transplant in 2012 who subsequently developed a symptomatic supraumbilical incisional hernia. The patient has autosomal recessive polycystic kidney disease, which led to end-stage renal disease, as well as congenital hepatic fibrosis resulting in portal hypertension. He was referred to pediatric surgery because of complaints of increased bulging and pain at the hernia site that gradually worsened over time. On physical examination, the patient had visible caput medusa (Fig. 1) throughout the anterior abdominal wall. Owing to his persistent symptoms, he was scheduled for an elective laparoscopic ventral hernia repair.
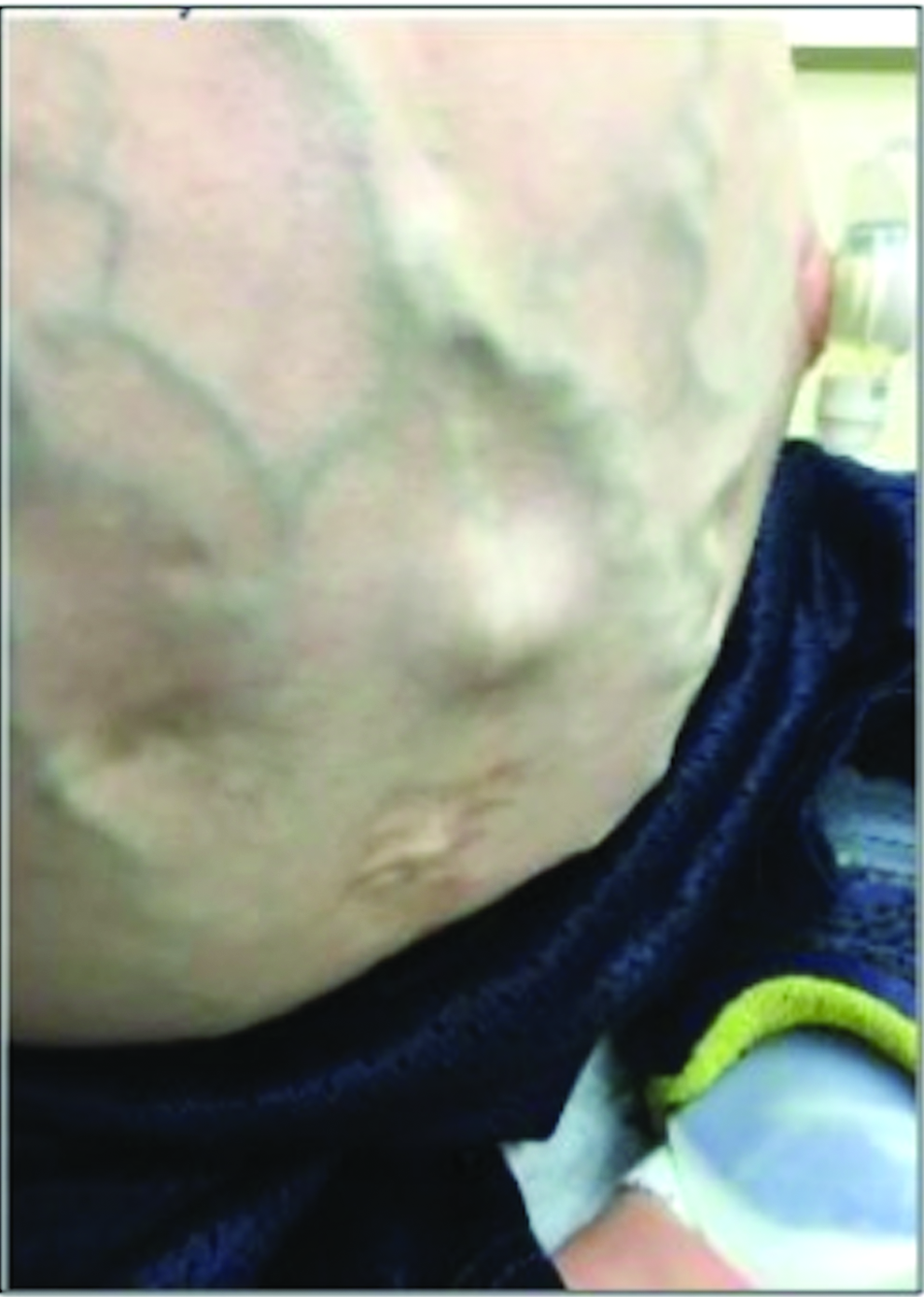
Anterior abdominal wall caput medusa.
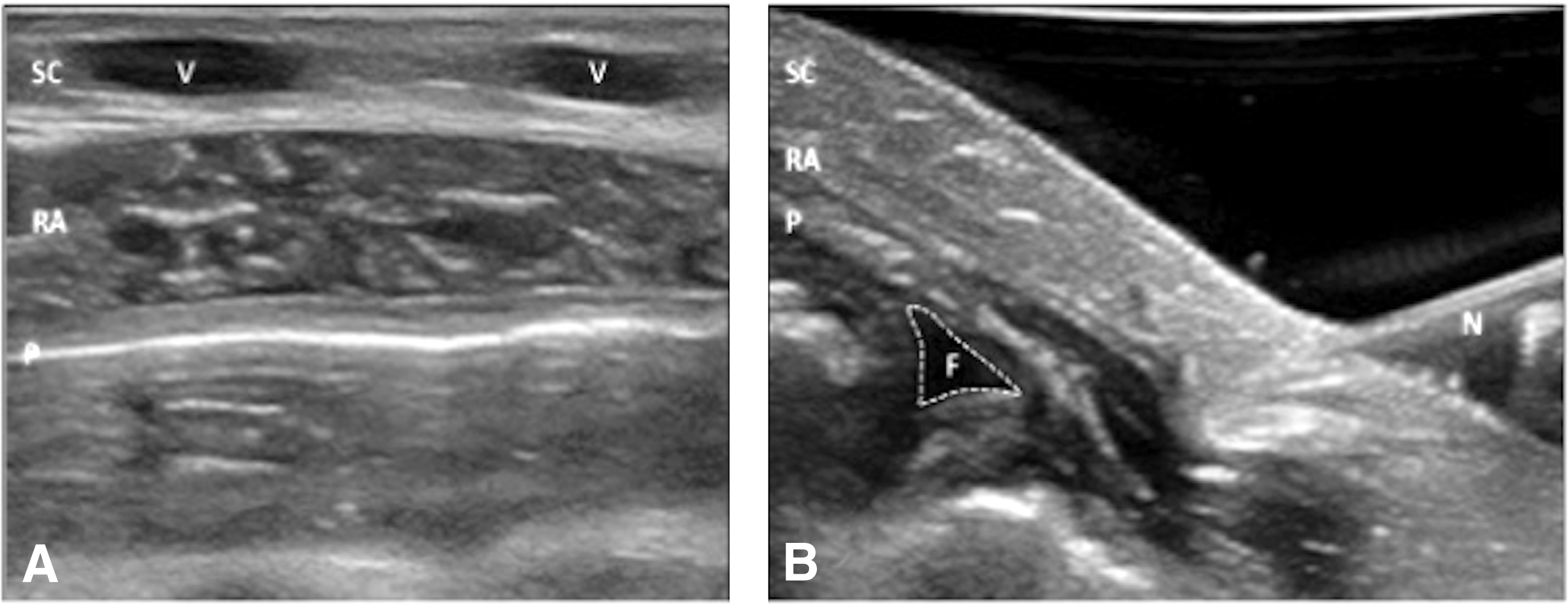
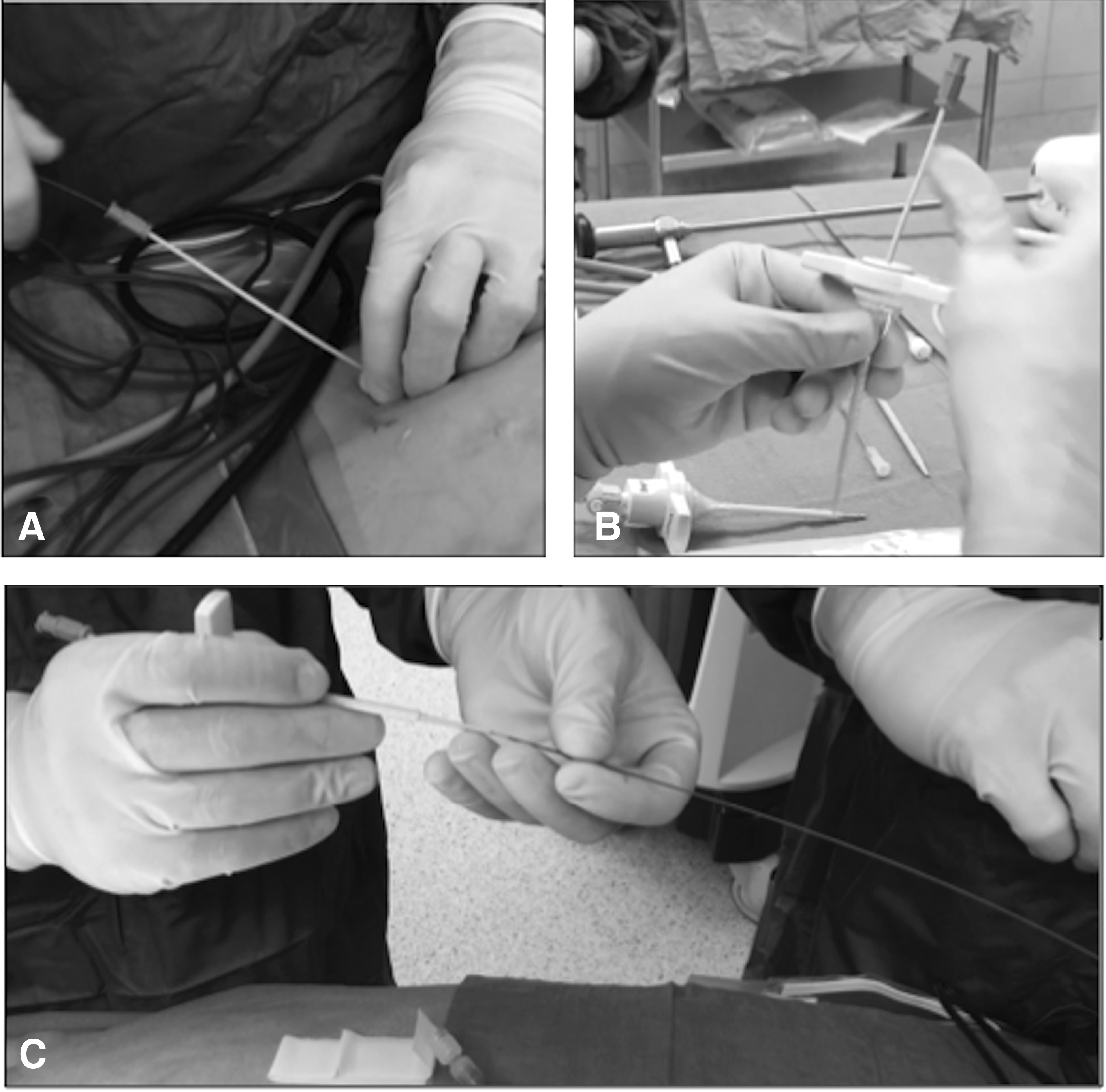
The patient was brought into the operating room and placed in the supine position. After intubation, the patient's abdomen was prepped and draped in the usual sterile manner. Ultrasound was then used to evaluate the anterior abdomen wall and locate abdominal wall vessels (Fig. 2A). Using ultrasound guidance, a 21 g micropuncture needle (Cook Medical, Inc., Bloomington, IN) was inserted just past the peritoneum in the right lower quadrant avoiding vessels and underlying bowel. In addition, using intraperitoneal fluid pockets as targets provides safe entry during needle insertion (Fig. 2B). Using the Seldinger technique, a 0.018 Cope wire (Cook Medical, Inc.) was placed through the needle, followed by a 3–4F dilator (Cook Medical, Inc.). Using the dilator, the 0.018 wire was exchanged for a stiff 0.035 Amplatz Super Stiff wire (Boston Scientific Corp., Natick, MA), which was used for serial dilations up to a 16F dilator. A VersaStep radially expandible sleeve or Veress sheath (Medtronic, Minneapolis, MN) was positioned over a 7F dilator (Fig. 3A) and placed into the abdomen, over the wire (Fig. 3B). After removal of the wire and dilator, a 5 mm Mini Step cannula and dilator (Medtronic) were safely placed without difficulty (Fig. 3C). The abdomen was insufflated and ultrasound was used again for placement of an additional 5 mm port. The area of the hernia was examined with ultrasound and vessel location was determined. A primary repair was performed with 0-Vicryl using a Carter-Thomason (CooperSurgical, Inc., Trumbull, CT) under laparoscopic and ultrasound guidance (Fig. 4A) with good result (Fig. 4B). The patient did well postoperatively and was discharged without complications.

Discussion
One of the major complications in laparoscopic surgery is injury at the time of entry into the abdomen. 13 Regardless of the entry technique, the overall vessel injury rate is low, with most injuries occurring to minor vessels at an incidence of 0.7%–2.5%.14–16 Despite being considered minor vessels, injury to epigastric vessels and collaterals can cause significant patient morbidity.17–19 This is especially relevant in patients presenting with portal hypertension and caput medusa. Control of bleeding in this case is often very difficult with various techniques described.8,20,21 In the event that the injury is not identified at the time of operation, the patient may develop abdominal wall hematomas, infections, or intraabdominal bleeding. Owing to these risk factors, ensuring proper precautions during this crucial step in the operation can prevent avoidable complications.
The use of ultrasound can help to observe structures in the soft tissue otherwise invisible to the naked eye. This is of particular importance in the setting of caput medusae, by which avoiding large vessels in the anterior abdominal wall can ultimately prevent significant complications while entering the abdomen for access.
Conclusion
Use of ultrasound-guided access into the peritoneum for laparoscopic surgery is a safe and effective approach in a patient presenting with portal hypertension. This technique demonstrates an effective tool in the surgical armamentarium for entering the abdomen in patients with caput medusae.
Footnotes
Disclosure Statement
No competing financial interests exist.