
Abstract
Abstract
Endoscopic mucosal resection (EMR) is an increasingly popular minimally invasive technique that is used for the management of superficial lesions in the upper and lower gastrointestinal tract. The goal of this article is to describe the indications and technique of EMR, with a focus on the endoscopic management of Barrett's esophagus (BE). The two major EMR techniques—cap EMR and band EMR—will be presented, along with a discussion of their efficacy as well as their integration into the broader treatment paradigm of endoscopic eradication therapy for BE.
Introduction
E
Indications
The basic premise of EMR is to remove the diseased mucosal layer by resection to the level of the submucosa. 1 EMR is indicated for the management of pre-malignant or malignant lesions that are confined to the mucosal layer, without involvement of the deeper submucosal or muscular layers and without evidence of venous or lymphatic involvement.2,3 There is no absolute limit with regards to maximal lateral size, only with regards to depth. However, lesions involving greater than 2/3 to 3/4 of the esophageal circumference are generally avoided due to their potential for stricture formation, although this is not an absolute contraindication.
Role of EMR in BE
In the esophagus, EMR is used with curative intent for the treatment of dysplastic BE and superficial well- and moderately differentiated carcinoma (i.e., intramucosal adenocarcinoma). When cancer is limited to the mucosa, the risk of metastasis is as low as 0%, increasing to 3% if the cancer invades the lamina propria, 12% if there is invasion of the muscularis mucosa, and 26% if there is invasion of the submucosa.1,3 EMR is, thus, limited to resection of mucosal lesions without involvement of the submucosa.
Multiple societal guidelines support the role of EMR in the management of BE. The American Society for Gastrointestinal Endoscopy (ASGE) recommends endoscopic resection of nodular dysplastic BE to determine the stage of dysplasia before considering other ablative therapy. 4 The American Gastroenterological Association (AGA) recommends EMR for patients with dysplastic BE associated with a visible mucosal irregularity to determine the T stage of the neoplasia. 5 The American College of Gastroenterology (ACG) recommends EMR as the initial diagnostic and therapeutic maneuver for patients with nodular BE. 6
Multimodality endoscopic eradication therapy for BE
Multimodality endoscopic eradication therapy (EET) involves the use of EMR to remove visible mucosal irregularities such as nodules or early esophageal carcinoma, followed by an ablative technique such as radiofrequency ablation (RFA) to eradicate any remaining BE (Fig. 1). 7 EMR yields large tissue specimens, up to 2 cm in size, for pathologic examination and cancer staging; studies demonstrate greater inter-observer agreement between pathologists with regards to dysplasia staging with EMR as compared with traditional biopsy specimens. 8 Histologic assessment of the EMR specimen also guides subsequent therapy via the T-staging information provided.

Multimodality EET for the treatment of BE.
The goals of EET are not only to achieve complete eradication of dysplasia (CE-D) but also to achieve complete eradication of intestinal metaplasia (CE-IM) to prevent neoplastic progression. Evidence for the efficacy of multimodality EET has emerged rapidly.9–12 RFA has been shown to lead to durable reversion of metaplastic mucosa to normal appearing neo-squamous epithelium in a high proportion of patients at any stage of BE. 10 EET with combination of EMR and RFA is now the treatment of choice in patients with BE with high-grade dysplasia (HGD) and/or intramucosal adenocarcinoma. 7 EET is also increasingly considered in patients with BE with established low-grade dysplasia (LGD), although its role in patients with non-dysplastic Barrett's esophagus (NDBE) remains controversial. 13
Technique
The two generally accepted EMR techniques are the cap and band techniques.
Cap EMR
Cap EMR is fundamentally based on the principles of snare polypectomy (Fig. 2).1,14
1. A transparent plastic cap is attached to the tip of the forward-viewing endoscope. There are two types of plastic caps. One is an obliquely cut large-capacity cap with an outer diameter of 16.5 mm, allowing for the removal of large samples up to 20–25 mm in size. The other is a straight-cut medium-size cap with an outer diameter of 13.5 mm, which can be used for the removal of smaller or residual lesions.
2. The mucosal surface surrounding the margins of the lesion can be marked by the tip of a snare wire by using electrocautery. Markings are placed about 2 mm away from the actual margins of the lesion. This step is especially important when the margins of the lesion are difficult to recognize or become distorted after submucosal injection.
3. A methylene blue-tinged normal saline solution (with 1:10,000 epinephrine, if desired) is injected into the submucosa with an endoscopic injection needle. Puncturing of the mucosa at an oblique angle is crucial to avoid transmural penetration of the needle. The total volume of injected solution may vary; however, it is important to lift the entire lesion. Injecting the distal margin first allows the lesion to be lifted toward rather than away from the endoscope. Lifting or bulging of the mucosa occurs when the solution is correctly injected into the submucosal layer. Inability of the mucosal layer to lift with the development of a bleb lateral to the lesion suggests possible submucosal involvement (“non-lifting sign”) and should prompt reconsideration and/or termination of the procedure.
4. A specifically designed small-diameter snare is “pre-looped” into the rim of the cap. To pre-loop the snare, moderate suction is applied to the adjacent normal mucosa to seal the outlet of the cap, and the snare wire is passed through the endoscopic channel and opened. The opened snare wire is fixed along the rim of the cap such that the outer sheath of the snare sticks up to the rim of the cap.
5. The pre-looped snare is maintained as the endoscope is brought near the target mucosa. The target mucosa, including the lesion, is fully suctioned inside the cap; alternatively, using a dual-channel endoscope, forceps can be used to pull the target mucosa into the suction cap. The snare wire is closed around the lesion, giving it a polypoid appearance.
6. The pseudopolyp of snared mucosa is cut by using blended-current electrocautery. “Resected specimens can be removed sequentially or stored in the stomach and collected en masse via a Roth net at the completion of the procedure.” (identical instructions as step 5 in band EMR section).
7. If additional resection is necessary, steps 3–6 should be repeated. Repeated saline injection is necessary to reduce the risk of muscle involvement during the procedure, as the injected solution may disappear within a few minutes of the injection.
8. On completion, the resection site should be closely inspected to exclude any residual mucosa, visible vessels that may require hemostasis, muscle involvement, or perforation.
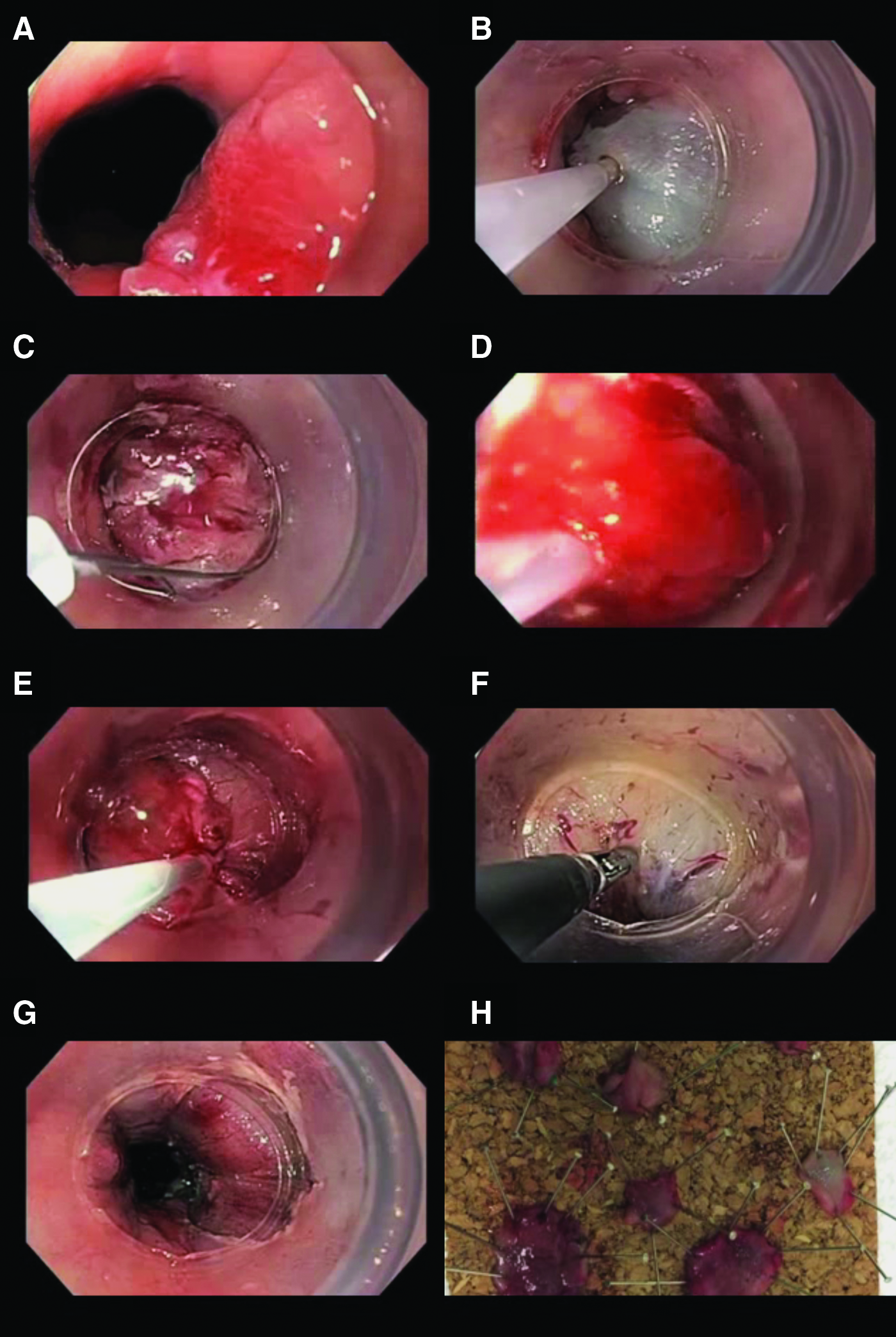
Steps in cap EMR.
Band EMR
Band EMR is fundamentally based on the principles of endoscopic band ligation, and it is also referred to as multiband mucosectomy (Fig. 3).2,15,16
1. As with cap EMR, the mucosal surface surrounding the margins of the lesion is marked by the tip of a snare wire by using electrocautery. Markings, when necessary, are placed 2–5 mm away from the actual margins of the lesion. The initial marking of the lesion may become important if the endoscopic view during resection becomes impaired by bleeding post-resection.
2. The endoscope is removed, and the ligator device is assembled. The wires that deploy the bands are positioned in line with the working channel to keep them out of the endoscopic view. The endoscope with the device attached is then re-introduced.
3. The delineated lesion is identified, and the mucosa is sucked into the cap. When the cap is completely filled with mucosa (known as complete “red-out”), a rubber band is deployed and a pseudopolyp of captured mucosa is created. The band is designed to not be strong enough to hold the muscularis propria, making routine submucosal injection/lifting unnecessary before resection.
4. A hexagonal snare is placed on the pseudopolyp and closed below the band. The pseudopolyp is then cut by using blended-current electrocautery.
5. In the same fashion, additional resection is performed by repeating steps 3 and 4. Resections are performed either in a distal to proximal fashion or starting at the most suspicious portion of the delineated area. An overlap of 10%–25% between adjacent resections ensures that no residual “tissue bridges” are left behind. Resected specimens can be removed sequentially or stored in the stomach and collected en masse via a Roth net at the completion of the procedure.
6. On completion, the EMR site should be closely inspected to exclude any residual mucosa, visible vessels that may require hemostasis, muscle involvement, or perforation.
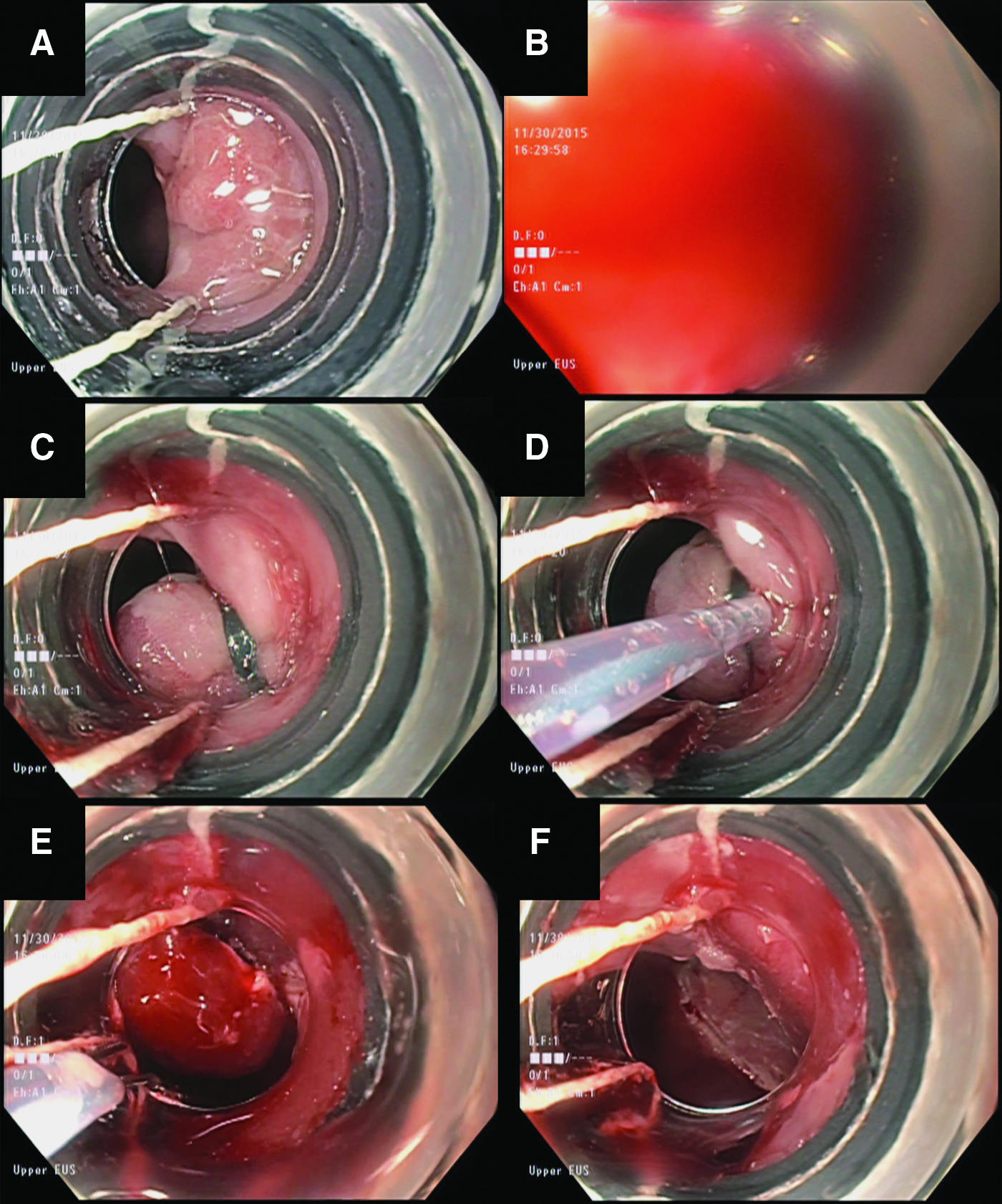
Steps in band EMR.
Clinical Outcomes
Evidence for the efficacy of EMR has rapidly emerged over the past two decades. Before the advent of RFA, EMR was used either alone or in conjunction with other ablative techniques such as photodynamic therapy (PDT). 17 EMR is now an integral component of multimodality EET, in conjunction with an ablative technique such as RFA.
Multiple groups have described the clinical success of EMR for BE. Ell et al. reported a prospective study of 64 patients who underwent cap EMR, of whom 61 had early carcinoma and 3 had HGD. 18 In their study population, 35 patients were considered “low-risk,” with lesion size ≤20 mm in diameter, and HGD or well to moderately differentiated adenocarcinoma without submucosal invasion. The remaining 29 patients were considered “high-risk,” with lesion size >20 mm in diameter, poorly differentiated adenocarcinoma, or with submucosal invasion. Complete remission was achieved in 97% of low-risk patients but in only 59% of high-risk patients. At mean 12-month follow-up, recurrent or metachronous carcinomas were found among 17% of low-risk patients and among 14% of high-risk patients, without statistical significance. Alvarez Herrero et al. prospectively studied 170 band EMR patients who underwent combined 243 band EMR procedures, of which 113 were performed for focal lesions, 117 were performed as part of a stepwise radical endoscopic resection (SRER) protocol in which EMR was used for resection of all abnormal tissue without the use of ablation, and 13 were performed as escape treatment after RFA. 15 Complete endoscopic resection was achieved in 91% of focal lesions, 86% of patients who underwent SRER, and 100% for escape treatment after RFA. These results led to multimodality EET to become the standard of care rather than SRER.
Favorable long-term EMR outcomes have also been demonstrated by multiple groups. Ell et al. reported long-term follow-up in 100 consecutive patients with dysplastic BE and low-risk adenocarcinoma. 19 Complete local remission was achieved in 99% after a mean of 1.9 months and a maximum of three EMRs. During a mean follow-up of 36.7 months, recurrent or metachronous carcinomas were found in 11% of patients, all of whom were successfully treated with repeat EMR. The 5-year survival rate was calculated to be 98%, with two patients dying from other causes. Similarly, Larghi et al. reported 26 consecutive patients with BE and either HGD or intramucosal adenocarcinoma who underwent SRER by using cap EMR. 20 At median 28-month follow-up, 87.5% of patients achieved endoscopic and histological eradication of BE. Two patients were found to have Barrett's epithelium beneath the neosquamous epithelium, and one patient had recurrent intramucosal adenocarcinoma that was successfully treated with repeat EMR. These results suggested favorable outcomes for EMR in patients with BE and low-risk adenocarcinoma.
Pech et al. evaluated the risk factors for recurrence in 349 patients with BE with HGD or intramucosal adenocarcinoma, of whom 279 underwent EMR, 55 underwent PDT, 13 underwent combined EMR and PDT, and 2 underwent argon plasma coagulation (APC). 21 A complete response was achieved in 96.6% of patients. At a mean follow-up of 63.6 months, 21.5% of patients developed metachronous lesions with a 5-year survival rate of 84%. No deaths were due to adenocarcinoma. Ultimately 3.7% of patients required surgery after failure of endoscopic therapy. Risk factors associated with recurrence included piecemeal resection, long-segment BE, no ablative therapy, treatment lasting >10 months before complete remission, and multifocal neoplasia. Given that residual or recurrent BE is at risk of neoplastic progression, and that long-term studies of the durability of EMR for maintaining re-epithelialization with neosquamous mucosa are presently lacking, guidelines advocate ongoing surveillance.4–6
Various groups have compared EMR techniques. May et al. reported a prospective study of 100 consecutive resections in 72 patients with early esophageal carcinoma, randomized to receive cap versus band EMR. 14 No significant differences were observed with respect to the maximum diameter and areas of the resected specimens, and no severe adverse events were seen with either technique. Further endoscopic therapy after initial resection was necessary in 57% of patients, typically due to lateral margins that could not be evaluated due to coagulation artifact or that were positive for malignancy. Pouw et al. compared cap versus band EMR with respect to procedure time and cost in a randomized trial of 84 patients undergoing piecemeal EMR for BE with HGD or intramucosal adenocarcinoma. 16 Band EMR resulted in decreased procedure time (34 minutes versus 50 minutes, P = .02) and costs (240 Euros versus 322 Euros, P < .01) than cap EMR. Band EMR also resulted in smaller individual resection specimens than cap EMR (18 × 13 mm versus 20 × 15 mm, P < .01), although there were no significant differences in depth of resection or adverse events.
EMR versus endoscopic submucosal dissection
Due to the size of the endoscopic cap, snare, and ligation device, EMR usually cannot remove lesions that are larger than 2 cm in one piece, an inherent limitation that can prevent accurate pathologic staging in larger lesions and can increase the risk of local recurrence. A related endoscopic resection technique, endoscopic submucosal dissection (ESD), uses specialized electrosurgical knives to cut the margins of the mucosal lesion, followed by submucosal dissection beneath the isolated mucosa.1,2 Developed in Asia for the resection of early gastric cancer, ESD allows for en bloc resection of large mucosal lesions that cannot be removed in such fashion by EMR, regardless of size.
Although potential advantages of ESD include better histologic analysis and decreased recurrence rates, ESD is more technically demanding and time consuming. 2 A study of 36 patients with BE with HGD or early adenocarcinoma who underwent ESD showed en bloc, R0, and curative resection rates of 100%, 81%, and 69%, respectively. 22 However, a meta-analysis that included 10 band EMR studies and six ESD studies showed that band EMR is not inferior to ESD when comparing outcomes related to recurrence and complications, results that favor band EMR given that it is considerably less time consuming. 23
Recently, Terheggen et al. reported a randomized trial comparing ESD versus cap EMR in patients with BE with HGD or early adenocarcinoma, with regards to histologically complete (R0) resection, CE-D, recurrence, and adverse events. 24 They found that R0 resection was achieved more frequently with ESD than with cap EMR (10/17 versus 2/17, P = .01). However, there was no difference in CE-D or recurrence. ESD was found to be significantly more time consuming, and it was associated with more complications (two cases of perforation). These results suggest that despite apparent technical advantages with ESD, this has not been translated into any clinical advantages in the endoscopic management of BE.
EMR as part of multimodality EET
Aside from short-segment BE or a solitary dysplastic lesion that can be completely treated with EMR alone, EMR is often used as part of multimodality EET in conjunction with an ablative technique such as RFA, in which EMR is used for focal lesions and RFA is used for flat dysplasia or residual NDBE. 7 Eradication of all BE by multimodality EET reduces the risk of subsequent HGD or esophageal adenocarcinoma.
Van Vilsteren et al. reported a multicenter randomized trial comparing SRER versus multimodality EET for the management of BE with HGD. 25 They studied 47 patients with short-segment BE (≤5 cm in length), of whom 25 were randomized to SRER and 22 were randomized to EMR + RFA. CE-D and CE-IM rates were similar between SRER and EMR+RFA (100% versus 96% for CE-D, 92% versus 96% for CE-IM). However, the rate of esophageal stenosis was significantly higher with SRER than with EMR + RFA (88% versus 14%), resulting in more therapeutic sessions (six sessions versus three sessions in the EMR + RFA group) due to the need for esophageal dilation.
Recently, Phoa et al. reported the results from the Euro II prospective multicenter study, which included 132 patients from 13 European centers. 26 Patients underwent EMR of visible nodules, followed by serial RFA every 3 months until all areas of BE were ablated or a maximum of five RFA sessions. Any residual BE was treated with a single additional session of EMR or up to two APC sessions. Based on an intention-to-treat analysis, CE-D was achieved in 92% and CE-IM was achieved in 87%. After a median 27-month follow-up, the recurrence rate of neoplasia and intestinal metaplasia was 4% and 8%, respectively.
EMR versus surgery
For the management of BE with HGD or intramucosal adenocarcinoma, esophagectomy traditionally has been the gold standard to which other therapies are compared. However, with increasing data, EMR and multimodality EET are now considered first-line therapy for the management of these indications. 7 Benefits of EET include decreased procedure-related morbidity and mortality, although with higher recurrence rates that can often be endoscopically managed.
Prasad et al. compared the long-term outcomes of 178 patients with intramucosal adenocarcinoma, of whom 132 were treated with EMR/PDT and 46 were treated surgically. 27 Survival was comparable, and treatment modality was not a significant predictor of survival. Recurrent carcinoma was found in 12% of endoscopically treated patients, all of whom were successfully retreated. Pech et al. studied a total of 114 patients with intramucosal adenocarcinoma, of whom 76 were treated with EMR/APC and 38 were treated surgically. 28 Complete remission was seen in all surgically treated patients and in 98.7% who were treated endoscopically. However, there was a 32% major complication rate in the surgical group compared with none in the endoscopic group. During a median 4.1 years of follow-up, one patient in the endoscopically treated group had local recurrence and four had metachronous neoplasia, with an overall recurrence rate of 6.6%, all of whom were successfully retreated.
Finally, Pacifico et al. studied 88 patients with intramucosal adenocarcinoma, of whom 24 were treated with EMR/PDT and 64 were treated surgically. 29 The surgical group was found to have a higher complication rate compared with those treated endoscopically (31% versus 4%), with one death in the surgical group due to complications. However, all patients in the surgical group remained cancer free over a mean 19-month follow-up, whereas only 83% in the endoscopically treated group remained cancer free over a mean 12-month follow-up.
Adverse events
Major adverse events from EMR are rare and include bleeding, perforation, and stricture formation. 4 Immediate bleeding from EMR can occur in up to 10% of patients, and it is primarily dependent on the EMR technique. Bleeding can be managed endoscopically by using conventional techniques such as bipolar cautery, hemostatic forceps, or hemoclips. Delayed bleeding is rare.
Esophageal perforation is reported in less than 3%–7% of patients at high-volume centers. 4 When identified expediently, perforations can often be closed endoscopically by using a variety of instruments, including standard hemoclips, over-the-scope clips, esophageal stents, and suturing.
Stricture formation is the most commonly reported adverse event of EMR. The rates of stricture formation vary depending on the circumference and length of mucosa removed by EMR, but they can occur in up to 17%–88% of patients.15,25,30 EMR should, therefore, be limited to lesions involving less than 2/3 to 3/4 of the esophageal circumference.1,2 Strictures can be managed endoscopically with esophageal dilation.
Summary
EMR is an important therapeutic technique in the management of pre-malignant and early-stage malignant lesions of the gastrointestinal tract. In the management of BE (Fig. 4), EMR has a valuable role in staging and provides a potentially curative resection of visible dysplastic lesions and intramucosal adenocarcinoma. EMR has become an essential component of multimodality EET for the endoscopic management of BE, for which the ultimate goal is total eradication of all Barrett's epithelium.
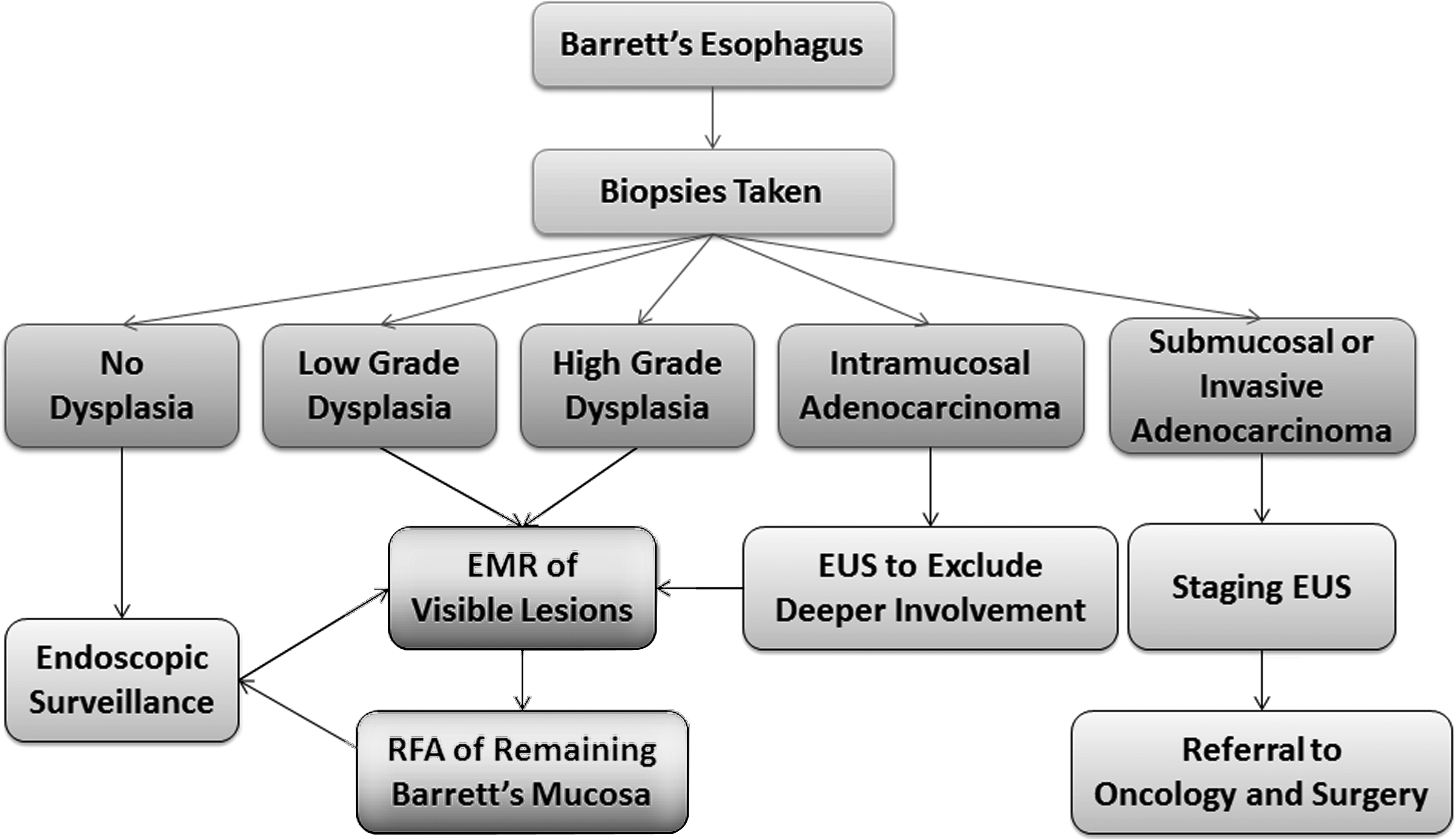
Current algorithm for the endoscopic management of BE.
The two established EMR techniques are cap EMR and band EMR. In general, cap EMR produces larger specimens than band EMR; however, it has a greater risk of muscle injury and, therefore, requires submucosal injection before resection. Band EMR is associated with decreased procedural time and costs than cap EMR; however, it results in smaller individual resection specimens, although without any reported difference in clinical outcomes. Given its excellent outcomes and limited adverse events, the use of EMR in conjunction with ablative techniques such as RFA has established multimodality EET as the first-line therapy for dysplastic BE and early-stage esophageal adenocarcinoma.
Footnotes
Disclosure Statement
No competing financial interests exist.