
Abstract
Abstract
Background:
Laparoscopic resection of gastric subepithelial lesions (SELs) located on the posterior wall of the gastric fundus is technically difficult and time-consuming. To facilitate access, we propose performing the laparoscopic procedure with patients in a right lateral decubitus position, rather than the standard supine position. The aim of our study was to compare operative and clinical outcomes for laparoscopic SEL resection performed in either the right lateral decubitus or the traditional supine position.
Methods:
The analysis was based on the data of 62 patients who underwent laparoscopic resection of SELs of the gastric fundus at Chonnam National University Hospital: 30 patients in the supine position (SUP) group and 32 in the right lateral decubitus position (RLD) group. All surgeries were performed by a single surgeon. Between-group comparisons were evaluated by Student's t, chi-squared, or Fisher's least squared tests, as appropriate for the data set.
Results:
Compared with the SUP group, the RLD had shorter operative time (103 minutes versus 52 minutes, P < .001), less intraoperative blood loss (71 mL versus 31 mL, P < .001), and lower C-reactive protein levels on postoperative days 1 and 2 (P < .005). Time to first flatus and length of hospital stay were comparable between groups.
Conclusion:
Laparoscopic gastric wedge resection for SELs on the gastric fundus in the right lateral decubitus position is feasible and safe, and provides operative advantages over the supine position.
Introduction
G
A tumor on the anterior gastric wall is easy to visualize and to remove laparoscopically. However, performing laparoscopic resection of a tumor on the posterior wall of the fundus or upper body of the stomach is difficult and time-consuming, as surgeons must divide the greater omentum and lift the stomach to expose the posterior gastric wall. 7 Moreover, the target lesion is generally located away from the video and working port. To address this issue, we have developed a novel approach for laparoscopic resection of SELs on the gastric fundus, placing patients in a right lateral decubitus position rather than the standard supine position. We adopted this positioning based on our experience with laparoscopic resection of gastric SEL in more than 30 patients. The aim of our study was to compare operative and clinical outcomes for laparoscopic SEL resection performed either in right lateral decubitus or in the traditional supine position.
Materials and Methods
Patients
This study was approved by the Institutional Review Board of Chonnam National University Hospital, South Korea (CNUH-2015-243). We conducted a retrospective evaluation of the 280 patients who underwent laparoscopic gastrectomy for gastric SELs by a single surgeon at our institution, between January 2009 and December 2014. All patients underwent a preoperative work-up that included esophagogastroduodenoscopy and computed tomography (CT) to specify tumor location. Endoscopic ultrasonogram (EUS) was performed in selected patients for further confirmation of tumor location. In standard manner, operative treatment was indicated for gastric SELs > 2 cm in diameter. However, operative treatment was also provided for gastric SELs <2 cm for patients who wanted operative treatment of the tumor, when an intermediate or high-risk gastrointestinal stromal tumor (GIST) was suspected, based on the results of EUS, or for tumors that increased in size during the follow-up period. Of the 280 prospective patients, 63 had SELs located on the gastric fundus, specifically on the superior portion of the body of the stomach, above the level of the cardiac notch. For the purposes of our analysis, we excluded patients who required a conversion from laparoscopic to open surgery. Our analysis, therefore, included the data of 32 patients who underwent laparoscopic surgery in the right lateral decubitus position (RLD group) and 30 patients who underwent surgery in the supine position (SUP group). We evaluated between-group differences for the following clinicopathological characteristics, identified retrospectively from patients' medical records: age; sex; body mass index (BMI, kg/m2); the American Society of Anesthesiologists (ASA) score; tumor location, divided into anterior wall and posterior gastric wall; tumor size and histological classification; operative results; hospital course; and morbidity and mortality.
Operative technique
SUP group
Under general anesthesia, patients were placed in the reverse Trendelenburg position with legs apart. The initial trocar was inserted at the umbilicus, using the Hasson technique. A pneumoperitoneum was created with carbon dioxide. Two right operator ports (a 5-mm upper and a 12-mm lower port) were inserted into the upper abdomen. The liver was then retracted upward, using a simple suture technique, and the location of the tumor mass was identified by either direct visual inspection or by palpation with the laparoscopic instrument. An omental dissection was performed, and the short gastric vessels were coagulated and cut with a harmonic scalpel (ACE36E; Ethicon Endo-Surgery, Cincinnati, OH) as needed. For tumors that were not palpable with the laparoscopic instrument were small (<1 cm) or had an endophytic growth pattern, preoperative tattooing around the tumor was performed using indigocarmine 0.8% either during the endoscopy or intraoperative esophagogastroduodenoscopy. Once the location of tumor(s) was confirmed, the stomach was mobilized, as required, and dissection of the omentum performed.
RLD group
Under general anesthesia, the patient was placed in the right lateral decubitus position (Fig. 1a). The operator stood on the right side of the patient and the video assistants on the left side. Three abdominal ports were placed along the left subcostal area, and the camera scope port was inserted on the left anterior axillary line using a direct trocar insertion method. 8 Other trocars were inserted carefully on the medial side through the initial port (Fig. 1b).
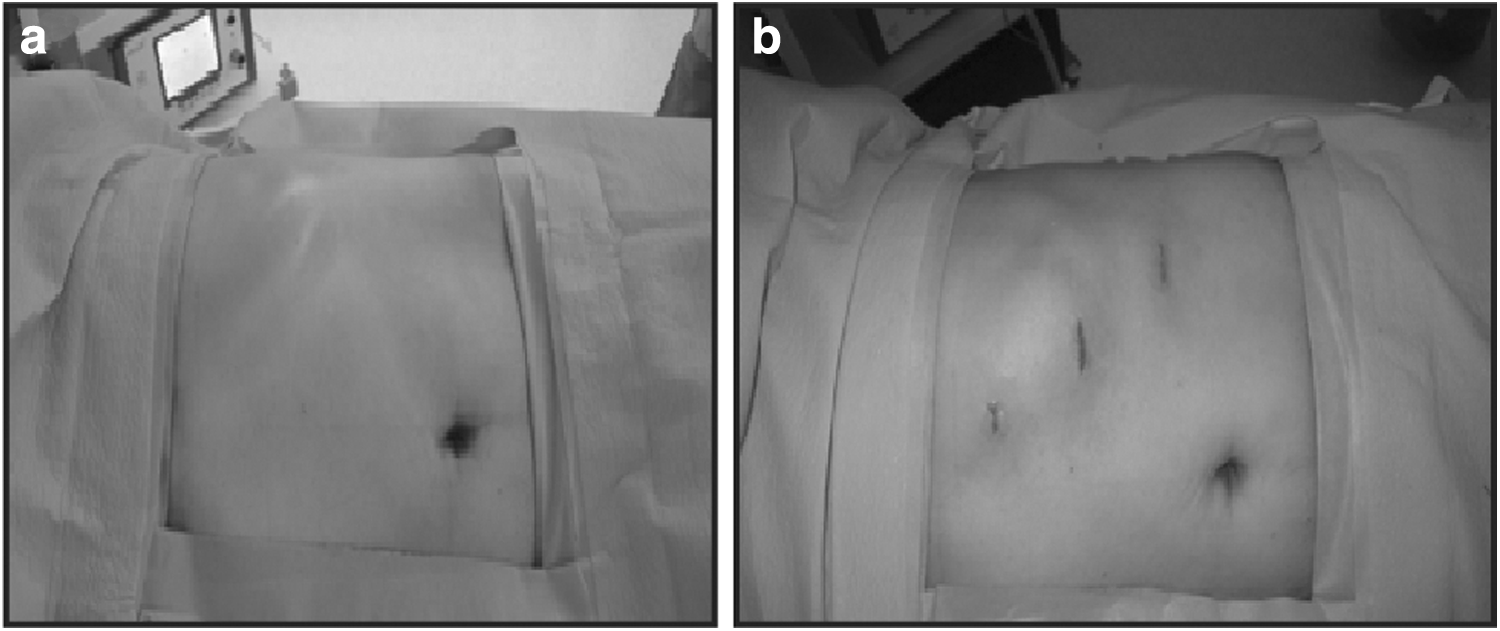
The patient was positioned in right lateral decubitus after being administered anesthesia.
Resection of gastric epithelial lesions
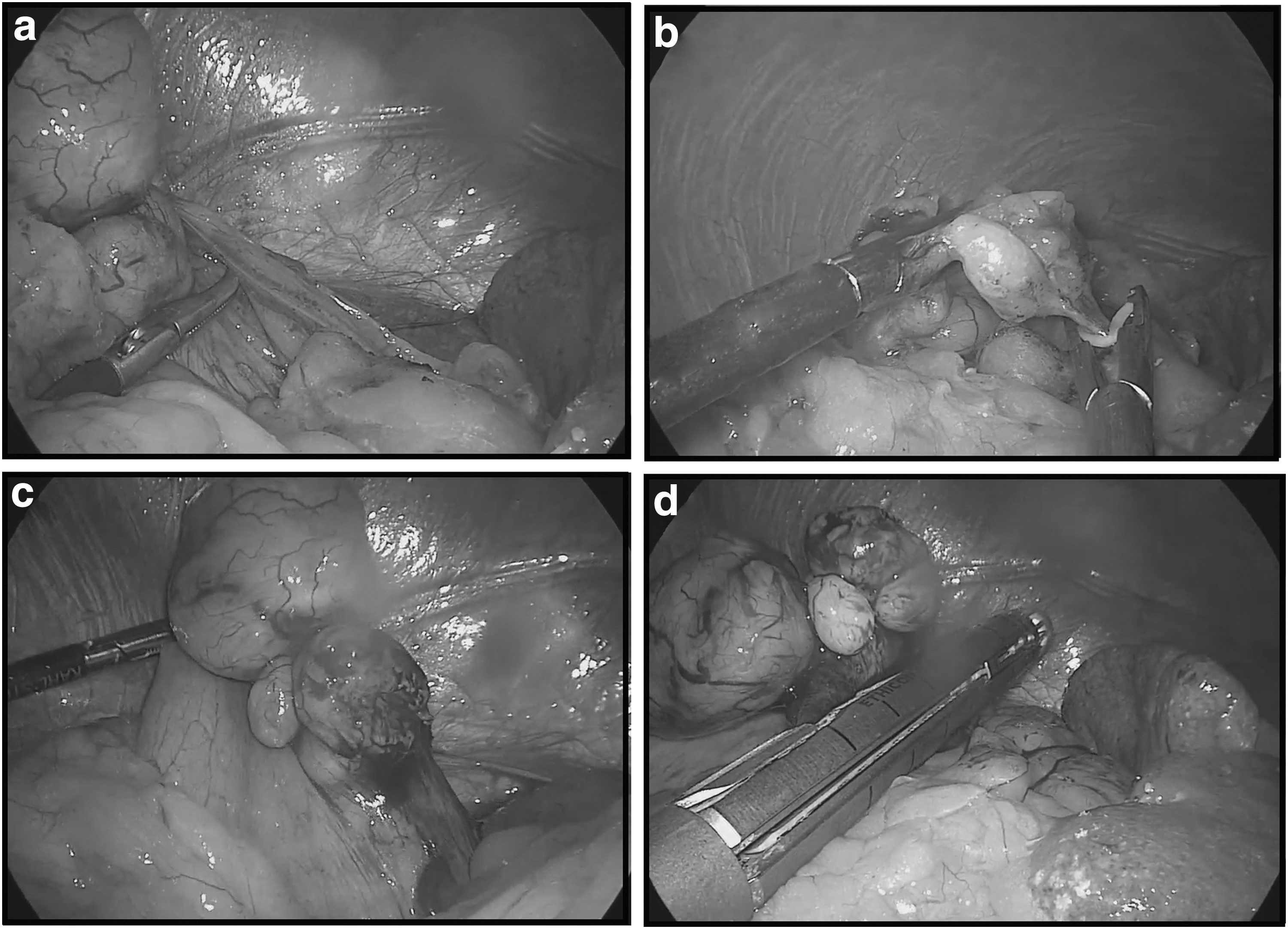
When the tumor was located in the great curvature, extending to the posterior side of the fundus, we ligated a branch of the short gastric arteries to lift the posterior wall of the gastric fundus (Fig. 2a, b). The tumor was grasped and pulled upward using atraumatic forceps (Fig. 2c), and a 60-mm endoscopic linear stapler (PSE60A; Ethicon Endo-Surgery) was subsequently used to resect the tumor. Bleeding from the stapling line was controlled using Bovie or Lembert sutures, depending on the surgeon's preference (Fig. 2d). The tumor was removed through the 12-mm working port using an endo-bag. Each trocar site was closed layer by layer. For all cases performed in the RLD group, fixation of the liver was not necessary. Lymph node dissection was not routinely performed as part of this procedure as lymphatic spread of submucosal tumors is rare. However, if enlarged lymph nodes were identified, those were dissected.
Postoperative course
Patients were allowed to start a soft diet on the morning of postoperative day (POD) 1. Postoperative pain was managed using intravenous, patient-controlled, analgesia for 2–3 days postsurgery. Intravenous fluid was administered in restricted amounts until POD 1. Patients were discharged from the hospital on POD 4, if they had no fever, tenderness, leukocytosis, or other complications.
Statistical analyses
Quantitative data are expressed as a mean ± standard deviation. Between-group differences were evaluated using Student's t or Mann–Whitney U tests for continuous data and chi-squared and Fisher's exact tests for categorical data, as appropriate for the data distribution. Continuous data from the different groups were compared using the nonparametric Mann–Whitney test. A P value <.05 was considered to be statistically significant. All analyses were performed using SPSS (version 18.0; SPSS, Inc., Chicago, IL).
Results
Patient and tumor characteristics
Patients' clinicopathalogical features for both the SUP and RLD group are summarized in Table 1. The distribution of pathological diagnoses was as follows: 51 cases of GIST (2 high risk, 9 intermediate risk, 19 low risk, and 21 very low-risk tumors; based on Fletcher's criteria) 9 ; 7 cases of leiomyomas; and 4 cases of other types of tumors (2 schwannomas, 1 granular cell tumor, and 1 hamartoma). The distribution of age, sex, BMI, ASA score, tumor size, and histological tumor classification were comparable for the two groups. The prevalence of SELs on the posterior wall of the fundus was higher in the RLD group, than in the SUP group.
ASA, American Society of Anesthesiologists; AW, anterior wall; BMI, body mass index; GIST, gastrointestinal stromal tumor; PW, posterior gastric wall; RLD, right lateral decubitus position; SUP, supine position.
Surgical outcome
The surgical outcomes for both groups are summarized in Table 2. The mean operating time for the RLD group was significantly shorter than for the SUP group with the intraoperative blood loss being significantly lower for the RLD group as well. There were no significant between-group differences in gas passage, and the mean hospital stay was comparable for both groups. The median level of C-reactive protein (CRP) was significantly lower for the RLD group than for the SUP group, particularly on POD 1 and 2 (Table 3). The rate of morbidity, reported in Table 4, was also comparable between groups, with no incidence of surgery-related mortality.
RLD, right lateral decubitus position; SUP, supine position.
CRP, C-reactive protein; RLD, right lateral decubitus position; SUP, supine position.
RLD, right lateral decubitus position; SUP, supine position.
Discussion
Laparoscopic local resection of gastric SELs, in the absence of lymph node metastases, has been widely accepted as a safe and feasible approach.10,11 Recently, various laparoscopic approaches for gastric SELs have been described based on tumor location.12,13 Laparoscopic wedge resection by endo-GIA™ is the most common technique used for gastric SEL resection due to its simplicity.7,14 However, wedge resection for SELs that are located on the posterior wall of the gastric fundus is technically difficult with various approaches having been described for laparoscopy resection of posterior wall gastric SELs. In 1997, Ibrahim et al. described a transgastric resection, with the tumor resected by endo-GIA performed through an anterior gastrotomy. 15 Ibrahim et al. concluded that a transgastric resection was simple to perform, provided excellent for hemostasis, and allowed excision of a smaller margin of normal tissue. However, both the intragastric and transgastric approaches require surgeons to perform additional complex steps compared with an extraluminal resection. Furthermore, an intragastric resection should be considered only for the treatment of small lesions due to the difficulty in controlling bleeding when resecting large lesions. Moreover, a transgastric resection requires additional laparoscopic stapler to repair the gastrotomy site as the omentum must be divided and the omental bursa entered to ultimately perform a resection that is similar to the extraluminal technique.
During laparoscopic surgery, exposure of the operative target organ is essential. In conventional laparoscopic surgery for lesions of the gastric fundus, the left lobe of the liver obscures the intraperitoneal laparoscopic field for left upper abdomen. Therefore, surgeons generally use various techniques for retraction of the falciform ligament and left lobe of the liver.16–18 However, performing these procedures is relatively time-consuming. Based on our experience, we proposed that closing the gap between the port and the target location on the gastric fundus would facilitate the operative procedure. This closing of the gap between the laparoscopic port and the gastric fundus was accomplished by moving the location of the video scope trocar from its usual position in the right subcostal area to the left subcostal area, with the patient in a right lateral decubitus position. 19 This change in patient positioning and trocar location provides a direct view of the gastric fundus, as well as reducing the distance between the videoscope and the working port. After a first successful laparoscopic gastric wedge resection in the right lateral decubitus position in 2010, we have now adopted this approach as our primary choice for laparoscopic wedge resection for SELs on the gastric fundus at our institution, having now performed more than 30 surgeries with patients in a right lateral decubitus position to date. In our review of the literature, we have identified only a few reports on laparoscopic gastrectomy for SELs on the gastric fundus, identifying the technical issues associated with resection performed on the posterior gastric wall. To our knowledge, we are the first to propose using a right lateral decubitus position to facilitate the procedure.
In our study group, the prevalence of tumors located on the posterior gastric wall was significantly higher in the RLD group than in the SUP group. Yet, operative outcomes favored the RLD group, a possible indication of the improved technical ease of performing these difficult SEL resections with patients in a right lateral decubitus position. Mean operative time was, in fact, significantly shorter for the RLD group, which likely correlates to the superior surgical view provided as the liver slides to a ventral position under the influence of gravity, avoiding the need for retraction of the falciform ligament and left lobe of the liver. For the supine position, if the SELs are located on the posterior wall of the gastric fundus, the greater omentum needs to be dissected and the assistant needs to lift the stomach ventrally to create an approach. In contrast, when patients are in a right lateral decubitus position, the laparoscopic instrument can be used to pull the gastric fundus to the caudal side to approach the gastric posterior wall. Moreover, when ligation of the short gastric artery is required, the right lateral decubitus position shortens the distance between the visual and working port, reducing the technical difficulty of clipping and ligating the artery and, therefore, shortening operative time, in addition to providing a better exposure of the posterior wall SELs. In fact, the operative time was significantly lower in the RLD group than in the SUP group (58.8 ± 33.0 minutes and 103.0 ± 51.8 minutes, respectively; P < .001). Certainly, operative time can also be shortened by surgeon's accumulated experience with the technique. To control for experience-specific effect on our outcomes, the surgeon had completed > 60 cases to ensure mastery of the technique before the start of the study.
Moreover, total blood loss was significantly lower in the RLD group than in the SUP group, which, again, may be because of an improved surgical view with patients in a right lateral decubitus position, which eliminated the requirement of omental dissection. Patient positioning did not influence any other surgical and clinical outcomes, with time to first flatus and length of hospital stay being comparable for the two groups. However, it is important to note that in our usual protocol, patients are discharged on POD 4, allowing sufficient time to effectively control pain postlaparoscopy, which typically peak, and 2–3 days after the procedure. 20 The median CRP level on POD 1 and 2 was significantly lower in the RLD group than in the SUP group, which might reflect the shorter operative time and avoidance of unnecessary tissue dissection and vessel ligation. Importantly, the complication rate was comparable between groups, with only one case of splenocolic ligament injury and abdominal wall muscle bleeding in the RLD group, which was directly caused by the insertion of the trocar laterally rather than on the anterior axillary line.
In conclusion, laparoscopic wedge resection for SELs on the gastric fundus with patients in a right lateral decubitus position is feasible and safe. This patient positioning provides several advantages, including shorter operative time and smaller volume of blood loss. Further studies are needed to fully prove the advantage of using a right lateral decubitus position for the resection of SELs on the posterior wall of the gastric fundus.
Footnotes
Acknowledgment
This study was supported by a grant (CRI 15016-1) by the Chonnam National University Hospital Biomedical Research Institute.
Disclosure Statement
None of the authors has any conflicts of interest or financial ties to disclose.