
Abstract
Abstract
Background:
The management of ectopic pancreas is not well defined. This study aims to determine the prevalence of symptomatic ectopic pancreas and identify those who may benefit from treatment, with a particular focus on robotically assisted surgical management.
Methods:
Our institutional pathology database was queried to identify a cohort of ectopic pancreas specimens. Additional clinical data regarding clinical symptomatology, diagnostic studies, and treatment were obtained through chart review.
Results:
Nineteen cases of ectopic pancreas were found incidentally during surgery for another condition or found incidentally in a pathologic specimen (65.5%). Eleven patients (37.9%) reported prior symptoms, notably abdominal pain and/or gastrointestinal bleeding. The most common locations for ectopic pancreas were the duodenum and small bowel (31% and 27.6%, respectively). Three out of 29 cases (10.3%) had no symptoms, but had evidence of preneoplastic changes on pathology, while one harbored pancreatic cancer. Over the years, treatment of ectopic pancreas has shifted from open to laparoscopic and more recently to robotic surgery.
Conclusions:
Our experience is in line with existing evidence supporting surgical treatment of symptomatic or complicated ectopic pancreas. In the current era, minimally invasive and robotic surgery can be used safely and successfully for treatment of ectopic pancreas.
Introduction
E
Most of what is understood about ectopic pancreas is derived from case reports, the earliest of which was written by Jean Shulz who described pancreatic tissue in the tip a jejunal diverticulum in 1727. 7 Subsequent histologic and necropsy reports starting in the 1800s identified pancreatic tissue within the greater curvature of the stomach at a prevalence of 0.55%–13.2%.5,8 A plethora of case reports later identified ectopic pancreas within the incisura and antrum of the stomach,9,10 the wall of the pylorus, 11 the duodenum, 12 the gallbladder wall, 13 jejunal diverticulum, 14 Meckel's diverticulum,14,15 jejunal mesentery,16,17 and small bowel mesentery.18,19 Gastric ectopic pancreas has even been described postgastric bypass, perhaps secondary to incretin stimulation. 20 As a result, a classification system has been developed to characterize pathologic grades. Originally developed by Heinrech in 1909 and later modified by Gaspar-Fuentes in 1973, the prevailing classification system divides ectopic pancreas into four types based on the integrity of pancreatic acinar cells, islet cells, and ductal anatomy: Type 1—typical pancreatic tissue with acini, islet cells, and ducts similar to normal pancreas; Type 2—pancreatic ducts only; Type 3—acinar tissue only; and Type 4—islet cells only. 21
The importance of identifying and classifying ectopic pancreas is directly related to the potential for the development of neoplasia, pancreatitis, and other morbid sequelae. Pancreatitis is a well-studied entity in which inflammation of the pancreas leads to fluid sequestration, profound hypotension, and significant morbidity even in the wake of improving critical care management of the 21st century.22,23 In fact, several scoring systems have been developed to identify those patients at greatest risk for the development of complications related to acute pancreatitis, 24 the earliest of which includes the Ranson criteria developed at our institution. 25 While ectopic pancreatitis is the most frequent presentation of symptomatic ectopic pancreas, incidental discovery is much more common,26,27 and delayed diagnosis can lead to morbid outcomes. In this report, we provide an extensive and current review of the literature along with our institutional experience with the management of ectopic pancreas, which over the years has evolved from traditional surgery to minimally invasive and now robotic surgical interventions.
Materials and Methods
We retrospectively identified a total of 32 cases of ectopic pancreas between January 1991 and December 2015, three of which were identified in aborted fetuses and excluded for the purposes of this report (Table 1). To identify our cohort, we searched our pathology database for the terms “ectopic pancreas,” “heterotopic pancreas,” or “Meckel's diverticulum.” Additional clinical data regarding clinical symptomatology, diagnostic studies, and treatment were obtained through chart review.
The majority (65.5%) of cases were noted incidentally at surgery for another reason. The most common locations of ectopic pancreas are the duodenum, small bowel, and stomach. Four cases had evidence of preneoplasia or neoplasia.
Results
Notably, 19 cases of ectopic pancreas were incidental findings noted intraoperatively or found incidentally in a surgical specimen (65.5%). Three out of 29 cases (10.3%) had evidence of preneoplastic changes on pathology (Table 2), while one harbored pancreatic malignancy. Of the three cases with preneoplasia, all were incidentally found lesions located in the duodenum or small bowel. Tumor sizes ranged from 0.5 to 4.8 cm in diameter. Three contained findings consistent with Pancreatic Intraepithelial Neoplasia 1 (PanIN-1) and had no symptoms before discovery. One case was located in the small bowel, contained pancreatic adenocarcinoma involving 3 out of 29 lymph nodes, and presented with a small bowel obstruction. None underwent routine surveillance, and 1 patient with PanIN-1 died due to unrelated causes after a complex abdominal wall hernia repair. Approximately, 11/29 (37.9%) of our known cases reported symptoms, two of which were noted to have classic symptoms of pancreatitis (Table 3). In these two cases, a robotic-assisted surgical approach was taken with complete resolution of symptoms.
Three cases were noted to have evidence of premalignant changes, all of which were asymptomatic and incidentally found. Tumor size ranged from 0.5 to 1.6 cm.
Pan-IN 1, pancreatic intraepithelial neoplasia.
The most commonly reported symptoms, if present, were abdominal pain, pancreatitis, and upper GI bleeding.
GI, gastrointestinal.
Case 1
The first case is a 22-year-old male with a history of upper abdominal pain who presented with 9 days of upper abdominal pain radiating to his back. He endorsed worsening abdominal pain with meals, but denied a significant drinking history or gallstone disease. During an episode of pain 7 months prior, he presented to an emergency room at an outside hospital. His lipase was 393 Units/L (U/L). Computed tomography (CT) scan was unrevealing, and he was later discharged. On admission to our university hospital's emergency department, his lipase was 1455 U/L. An abdominal ultrasound, CT scan of the abdomen and pelvis, and a magnetic resonance cholangiopancreatography failed to identify any gallstones, biliary, or pancreatic pathology. Subsequent esophagogastroduodenoscopy (EGD) and endoscopic ultrasound (EUS) showed a 4 cm submucosal mass in the greater curvature of the stomach, with a questionable ductal structure (Fig. 1). Given his recurrent symptomatology and EGD findings suspicious for ectopic pancreas, the patient was taken to the operating room (OR) for a robotic-assisted laparoscopic wedge gastrectomy. The patient's pain resolved immediately after surgery, and his lipase downtrended to 41 U/L on postoperative day 1. He was discharged on postoperative day 2 without complication. Two weeks after discharge, the patient was seen as an outpatient with minimal incisional pain and resolution of his symptoms. Pathologic report showed Gaspar-Fuentes Type 1 submucosal heterotopic pancreatic tissue measuring 2.5 × 2.0 × 1.5 cm (Fig. 2). The patient was evaluated 18 months after surgery without recurrence of his symptoms.

Esophagogastroduodenoscopy findings of large submucosal mass (thick white arrow). Endoscopic ultrasound with questionable ductal structure within the same submucosal mass (thin white arrow).

Gross pathologic specimen with notable submucosal mass (solid black arrow), along with cross-sectional image of pathologic specimen with tan, submucosal heterotopic pancreatic tissue (dashed black arrow).
Case 2
The second case is a 35-year-old male with a history of upper abdominal pain who was transferred to our hospital for management of intermittent epigastric pain and possible gastric neoplasm. Seven months before admission, the patient began to experience postprandial epigastric pain radiating to his back. He endorsed mild alcohol use. At that time, he underwent an EGD that showed a small ulcer in the antrum and mild chronic gastritis. He was started on a proton pump inhibitor and counseled to avoid nonsteroidal anti-inflammatory drugs. Five months before admission, the patient underwent repeat EGD and magnetic resonance imaging for recurrence of his abdominal pain, which showed an antral ulcer with mild nonspecific chronic gastropathy and pancreas divisum. A CT scan was performed, which showed a 6.0 × 4.5 cm peripherally enhancing fluid collection abutting the gastric antrum and first portion of the duodenum and a serum lipase level of 302 U/L (Fig. 3). Given his chronic and recurrent abdominal pain, possibly due to the fluid collection of uncertain etiology, the patient was transferred to our hospital for further management. With a preoperative diagnosis of gastric outlet obstruction due to the inflammatory mass, the patient was taken to the OR for a robotic-assisted laparoscopic partial gastrectomy with Billroth II reconstruction. Gross evaluation of the specimen revealed a central umbilication in the mucosa overlying a tan yellow tubular 1.0 × 0.5 cm structure (Fig. 4). The pathology showed Gaspar-Fuentes Type 1 ectopic pancreatic tissue in the gastric wall with surrounding scar-like fibrosis, chronic inflammatory infiltrate, a cystically dilated duct, and an overlying ulcerated epithelium. After a postoperative course notable for ileus, the patient was discharged. Follow-up at 2 weeks and 24 months after surgery revealed that the patient had been without recurrence of symptoms and free of abdominal pain.
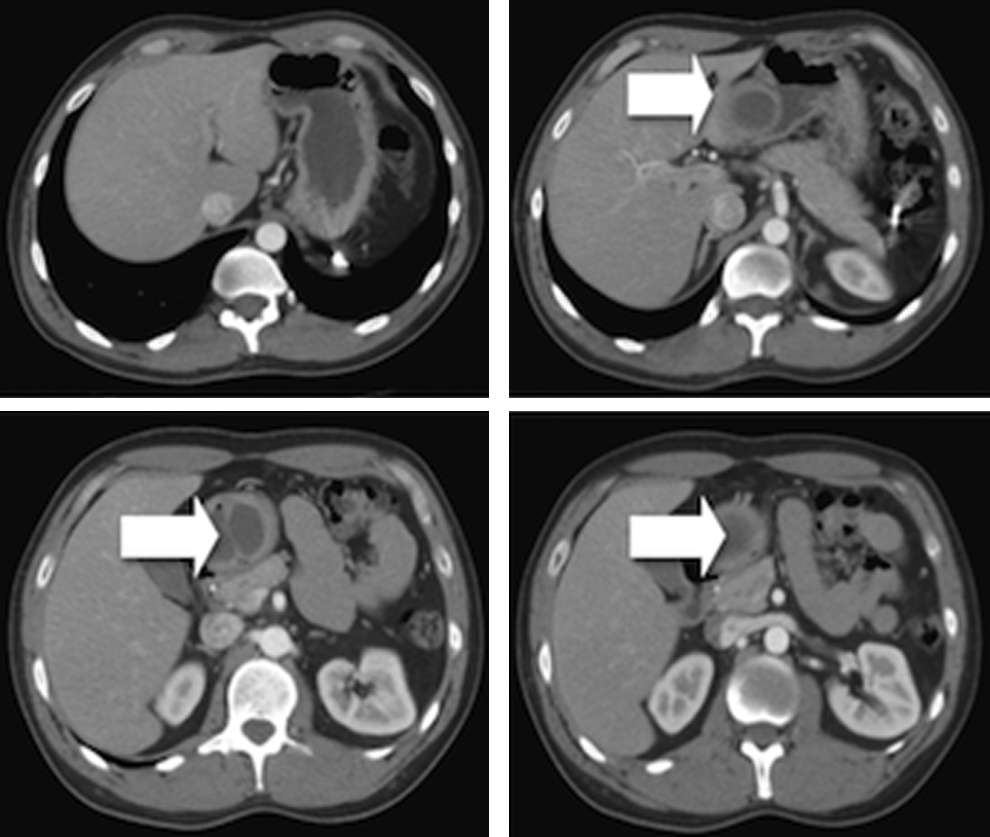
Sequential images from computed tomography scan of the abdomen and pelvis with gastric outlet obstruction secondary to submucosal mass (thick white arrows).
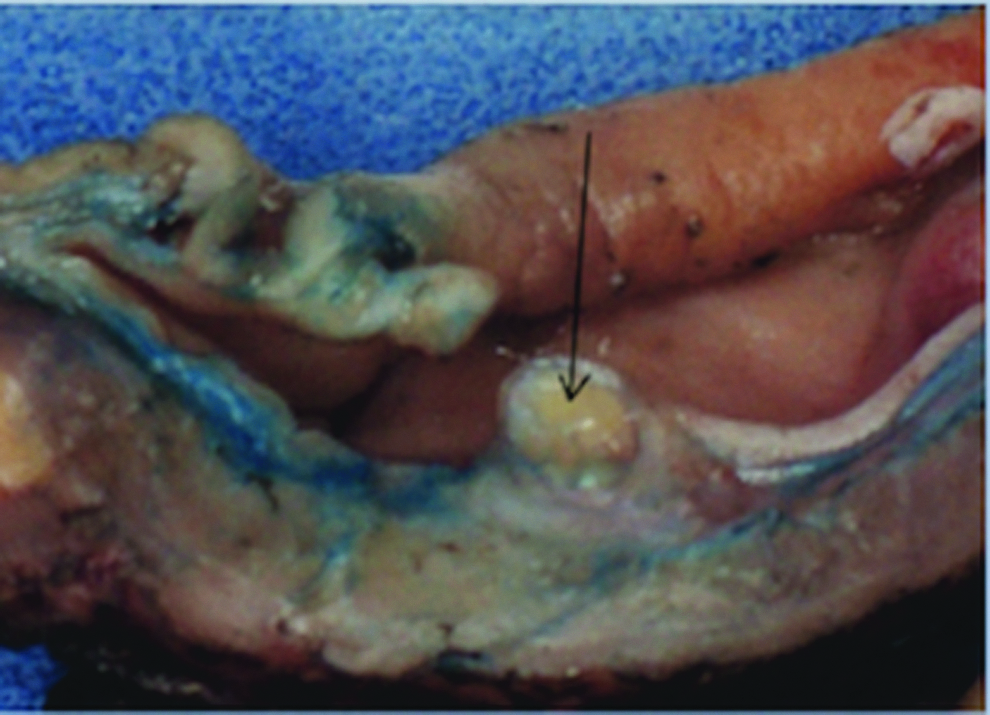
Gross pathologic specimen of tan, tubular structure causing gastric outlet obstruction at level of antrum and pylorus (thin black arrow).
Discussion
Ectopic pancreatitis is an unconventional cause of chronic abdominal pain, but its prevalence may be underestimated. Approximately 10% of 136 million emergency department visits per year are due to abdominal pain, yet 25% of these visits, or 3.4 million patients, never have a clear cause of their abdominal pain identified.28,29 Furthermore, lipasemia is evident in ∼12.5% of patients admitted to the hospital with “nonpancreatic abdominal pain.” 30 Given the reportedly increasing prevalence of ectopic pancreas and the identification of subepithelial masses in 1% of all esophagogastroduodenoscopies,27,26 lipasemia accompanied by abdominal pain and normal pancreatic imaging may be indicative of ectopic pancreatitis. In our report, we describe two cases of ectopic pancreatitis in which patients with chronic abdominal pain and lipasemia were evaluated in emergency departments multiple times over the course of 7 months without a clear diagnosis.
Since 1% of all EGDs result in the identification of a subepithelial mass,27,26 an examination of the diagnostic criteria and surveillance of ectopic pancreas are warranted. A defining characteristic, although not 100% specific, is a submucosal mass with central umbilication. When biopsied, histological examination confirms fragments of pancreatic tissue. EUS has also been used to identify ectopic pancreatitis, which helps differentiate ectopic pancreas from other mesenchymal tumors of the stomach such as gastrointestinal (GI) stromal tumors.31,32 Characteristics include indistinct borders, heterogenous echogenicity, the presence of an anechoic area, and location within two or more layers of the bowel wall. Through reliable diagnostic and imaging criteria on EUS noted by Park et al., ectopic pancreas can often be diagnosed radiographically without having to risk the complication of pancreatitis after biopsy.31,33
Asymptomatic ectopic pancreas is likely a benign anomaly and may be best left alone. It has been noted that asymptomatic lesions up to 2 cm in diameter may be monitored clinically without endoscopic surveillance. 33 Current recommendations do not support routine biopsy or follow-up screening for incidental ectopic pancreas tissue as the rate of malignant transformation is noted to be exceedingly low.26,35 Nearly all cases of malignant transformation in ectopic pancreatic tissue are case reports. Yet, the prevalence of preneoplasia in our cohort of incidentally obtained ectopic pancreas specimens was 13.8%. Three out of the four cases of neoplasia were asymptomatic, incidentally discovered PanIN-1 lesions, and did not undergo radiological or endoscopic surveillance. The remaining case presented with a small bowel obstruction secondary to a perforated small bowel tumor, discovered to be pancreatic adenocarcinoma, presumably secondary to transformation of ectopic pancreas tissue. In addition to our experience with pancreatic adenocarcinoma developing from ectopic pancreas, Fukumori et al. describe a case where surveillance of a gastric subepithelial lesion ultimately resulted in elevation of cancer antigen 19–9 and a diagnosis of ectopic pancreatic cancer. 36 In the rare case that ectopic pancreas is biopsied and shown to contain preneoplasia, consideration should be made for surgical resection. Furthermore, based on our knowledge that native pancreatic cancer metastasizes by lymph nodes and our ectopic pancreatic adenocarcinoma involved 3 out of 29 regional nodes, consideration should be given to lymphadenectomy as well. In our cohort, pancreatic intraepithelial neoplasia was noted in tumors 0.5, 1.3, and 1.6 cm in diameter. Further prospective evaluation should be performed correlating the incidence of neoplasia to the size of ectopic pancreatic tissue to create formal surveillance guidelines.
It has been proposed that treatment is necessary for symptomatic ectopic pancreas lesions and lesions greater than 3 cm. 37 Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) are an effective treatment for submucosally located symptomatic ectopic pancreatitis, with an R0 resection rate approaching 82%–90%.38–40 Since the most common location for ectopic pancreas is in the submucosal layer of the GI tract, this approach may be effective for ∼54% of cases. 38 However, with this approach, perforation occurs in 5.4%–15% of patients, bleeding in 2.7%, and pneumoperitoneum in 8.1%.40,41 Additional consequences of ectopic pancreas that may not be best addressed with EMR and EMD include recurrent pancreatitis, gastric outlet obstruction, 42 pseudocyst formation,43,44 malignant degeneration,45,46 and GI bleeding.47,48
Based on our institutional experiences and an extensive review of the literature, we propose that asymptomatic lesions larger than 3 cm, symptomatic ectopic pancreas, biopsied lesions with evidence of premalignancy, or lesions located in the muscularis propria, subserosa, or serosal layers of the GI tract, which may occur in up to 33% of cases, 49 should be managed with minimally invasive surgical resection, as EMR and ESD are unlikely to safely and adequately resect ectopic pancreatitis in the deeper layers of the GI tract. 50 In addition, complications of ectopic pancreatitis, such as gastric outlet obstruction, pseudocyst formation, malignant degeneration, GI bleeding, and perforation should be managed with a definitive surgical resection. In past case reports, open subtotal gastrectomy with Billroth II reconstruction and exploratory laparoscopy with segmental excision have been performed for gastric outlet obstruction secondary to ectopic pancreas.34,51 We employed robotic-assisted gastric resections with immediate and complete symptomatic relief of ectopic pancreatitis. To our knowledge, our reports are the first to show a robotic-assisted gastrectomy as a reasonable approach to the management of symptomatic ectopic pancreatitis.
Footnotes
Disclosure Statement
No competing financial interests exist.