
Abstract
Abstract
The fundamental approach to endoscopy is to identify concerning and potentially premalignant lesions in the gastrointestinal tract, sample or resect the area of interest, await histologic results, and subsequently formulate a treatment and/or surveillance strategy. Detecting subtle lesions and deciding whether they are clinically significant are challenges that rely on the endoscopist's observation skills and experience. Enhanced imaging technologies have been developed to aid in lesion identification and classification, enabling better visualization of the lumen from a wide-field view while also enabling real-time near-field, including cellular level, imaging of the tissue. These innovations can potentially help reduce the rate of missed lesions, the need for extensive surveillance biopsies, and the frequency of surveillance. Several of these advanced imaging technologies are discussed in this review.
Introduction
I
Endoscopic imaging modalities can be characterized by their field of view (Table 1). The mainstay of endoscopy is wide-field imaging to quickly scan large surfaces in the
WLE, white-light endoscopy; NBI, narrow-band imaging; HGD, high-grade dysplasia; NPV, negative predictive value; HD-WLE, high-definition white-light endoscopy; FICE, flexible spectral imaging color enhancement; AFI, autofluorescence imaging; CLE, confocal laser endomicroscopy; GI, gastrointestinal; IV, intravenous; VLE, volumetric laser endomicroscopy; OCT, optical coherence tomography; EUS, endoscopic ultrasound; HRME, high-resolution microendoscopy; LED, light-emitting-diode.
High-Definition White Light Endoscopy and High-Magnification Endoscopy
An endoscopic image is generated in several steps, including illumination of the tissue with a light source, capture of the image by digital sensors, and processing of the image for visual display. Technologic advances now allow smaller digital sensors to capture and produce images with a higher pixel density (resolution) than in standard-definition white-light endoscopy (SD-WLE), resulting in sharper and more detailed images. 1 This is known as high-definition white-light endoscopy (HD-WLE), now considered the minimum standard of care (Figs. 1a and 2a). 2
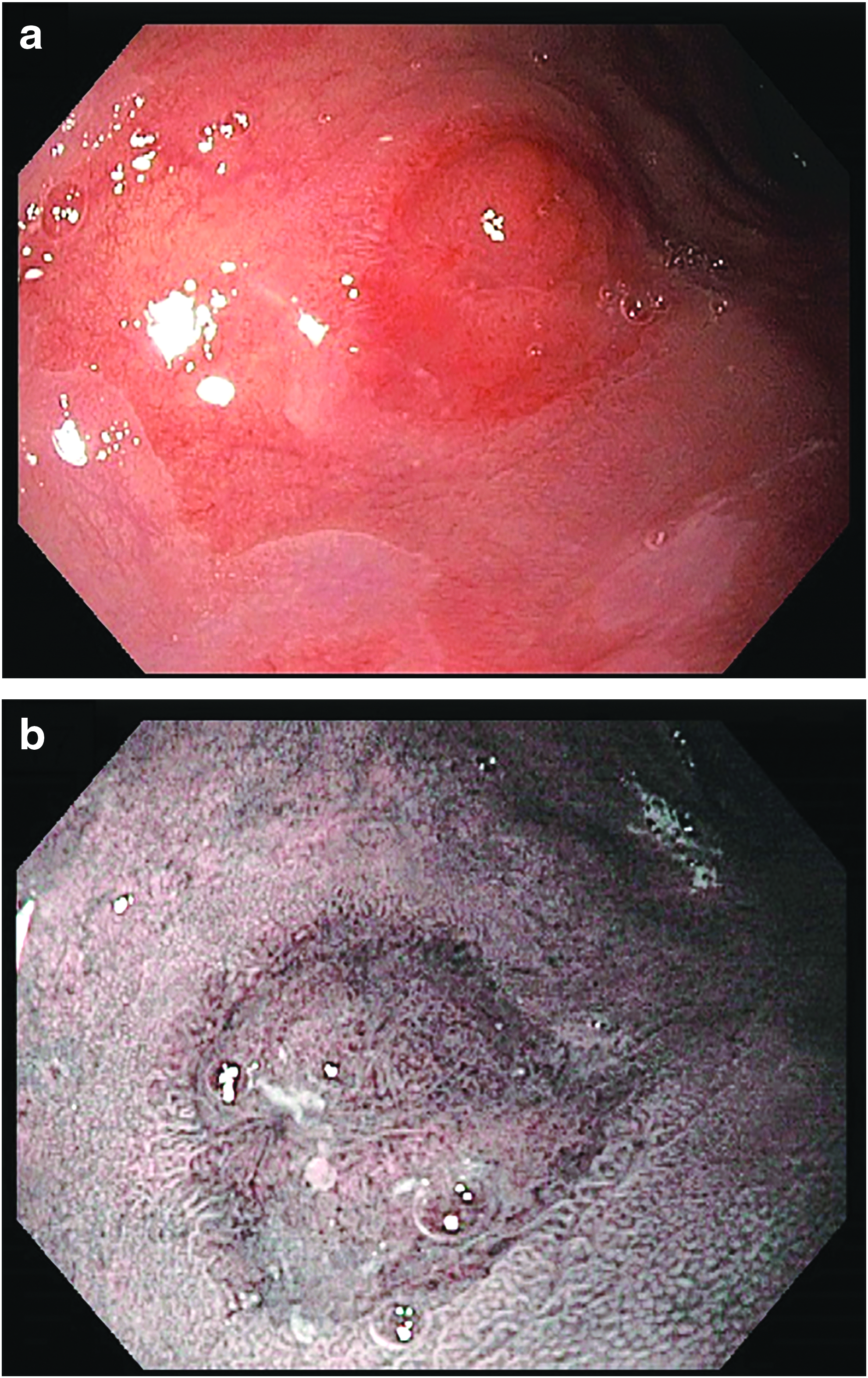
A nodule containing intramucosal adenocarcinoma arising in a background of high-grade dysplasia and Barrett's esophagus seen via high-definition white-light endoscopy
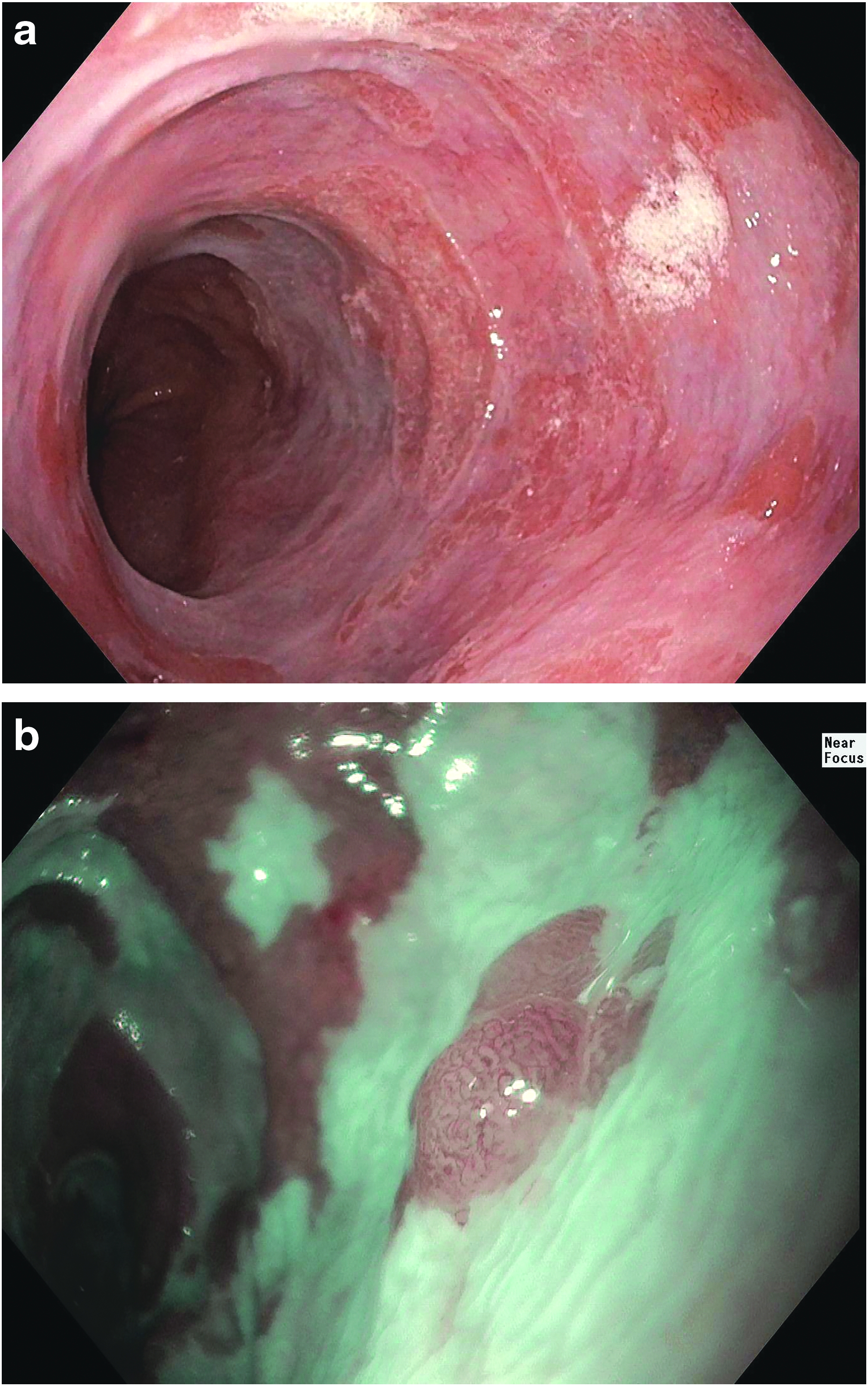
Barrett's esophagus under high-definition white-light endoscopy
In addition to resolution, the other component of high-quality visualization is magnification. Most endoscopes use a lens to magnify an image 30- to 35-fold while maintaining resolution, sometimes with additional digital zoom features. 1 There are also high-magnification endoscopes, which can perform optical, rather than digital, zoom of up to 150-fold while maintaining resolution by using a movable lens in the tip of the endoscope. 1 High-magnification endoscopes are specialized instruments that should not be confused with the standard magnifying features of most endoscopes. However, newer devices made by Olympus (190 series) have a limited form of optical zoom called near-focus mode (Fig. 2b), using a two-stage lens at the tip of the endoscope. This allows visualization of tissue 2–6 mm away from the tip without loss of focus or resolution. 1
In terms of evidence, it is difficult to interpret the impact of HD-WLE compared to SD-WLE, as most studies compared the technologies in combination with another modality, such as narrow-band imaging (NBI), rather than as a head-to-head assessment. However, information extrapolated from these studies and the resulting expert opinions suggest that HD-WLE is superior to SD-WLE.1,2
Optical Chromoendoscopy/Electronic Image Enhancement (Narrow-Band Imaging, Flexible Spectral Imaging Color Enhancement, i-Scan)
Chromoendoscopy refers to wide-field colorimetric techniques to highlight specific features of the tissue being examined during endoscopy. This can come in via electronic chromoendoscopy (as optical or digital chromoendoscopy) or by spraying chemical substances via dye-based chromoendoscopy, described later.
Electronic chromoendoscopy consists of a set of proprietary image modification techniques built into the endoscopy system or the processing software. Olympus offers NBI, which uses an optical filter placed in front of the endoscope's light source (usually a white xenon lamp). 3 The NBI filter preferentially illuminates the two absorption peaks of hemoglobin, highlighting blood vessels. This increases contrast between vascular and nonvascular tissues and enables a sharper image (Figs. 1b and 2b). This also helps isolate dysplastic or malignant lesions, which often have a prominent disordered vasculature due to angiogenesis, from non-neoplastic tissue. 3
The other electronic image enhancement techniques use digital processing of images rather than optical filtering. These include i-Scan, a product of Pentax Medical, and flexible spectral imaging color enhancement (FICE), a product of Fujinon. 3 i-Scan and FICE utilize software to analyze the image and enhance certain color wavelengths, thereby highlighting vasculature and increasing surface contrast. 3
To date, NBI has been the mostly commonly studied and utilized modality. Data on FICE and i-Scan are more limited, but the performance characteristics appear to be similar to NBI. 4 The primary benefits of these techniques are their ability to highlight subtle mucosal and vascular patterns at the push of a button. Electronic chromoendoscopy is therefore useful for real-time, in vivo detection of abnormal mucosa and enables trained operators to predict histology with reasonable accuracy. 3
In BE, NBI appears to be useful as a complementary tool for identification of intestinal metaplasia and dysplasia. A 2016 meta-analysis of nine studies reported a sensitivity of 94.2%, specificity of 94.4%, and negative predictive value (NPV) of 97.5% for the detection of dysplasia during surveillance. 5 In addition, fewer biopsies may be required compared to random biopsy protocols for dysplasia detection without sacrificing sensitivity and accuracy, allowing potential cost and time savings. 6
Despite these promising results, optical chromoendoscopy with targeted biopsies remains an adjunctive technique rather than a replacement for HD-WLE and random biopsy protocols for most providers. This is because most of the existing literature has been published by endoscopists with significant expertise in BE and NBI, as well as the fact that a standard classification system of mucosal and vascular patterns has not yet been universally adopted.5,7
For colonoscopy, studies on NBI are more heterogeneous, often comparing NBI to SD-WLE, which is no longer the standard of care. Meta-analyses of randomized controlled trials have not shown improvements in adenoma detection rates or polyp miss rates when comparing WLE to NBI. However, for diminutive colorectal polyps (≤5 mm), NBI was found to have a >90% NPV and high diagnostic accuracy for adenomas, serving as a useful “optical biopsy” tool based on surface characteristics alone.4,5 Polyps of this size are highly unlikely to harbor malignancy, so diagnosis of an adenoma serves primarily to correctly assign the interval to the next surveillance colonoscopy. 5 Given the high degree of diagnostic confidence with NBI, a strategy to resect and discard such tiny adenomas has been endorsed for clinical practice to reduce the need for pathology confirmation, thereby reducing costs. 5
Dye-Based Chromoendoscopy
The alternative to electronic chromoendoscopy is dye-based chromoendoscopy, a wide-field technique in which a topical stain is applied to the mucosa to provide contrast enhancement. 8 A variety of agents have been studied, including indigo carmine, iodine-based solutions, methylene blue, and acetic acid. Each agent has specific staining properties to enhance mucosal detail. For example, methylene blue and iodine are vital stains absorbed by specific tissues. After spraying the stain, the mucosa is washed to determine which areas stain and which do not. Methylene blue preferentially stains intestinal and colonic mucosa without staining squamous epithelium, identifying intestinal metaplasia in the esophagus (Barrett's). Indigo carmine, in contrast, does not stain mucosa, but pools in mucosal grooves and crevices to highlight surface topography. Acetic acid itself is colorless, but can wash off mucus and reacts with the mucosa to enhance surface patterns. 2
While it can significantly improve visualization of the mucosa, dye-based chromoendoscopy has not gained widespread clinical use for several reasons. It is felt to be tedious and time-consuming compared to electronic chromoendoscopy and requires contrast dyes, for which there are concerns about mucosal damage and overall safety.2,7 It requires a certain degree of technical experience to properly spray the dye and interpret the images to differentiate true lesions from normal findings.
In addition to the aforementioned technical concerns, there is also uncertainty about the accuracy of this technique. For BE, only acetic acid has met the minimum accepted sensitivity and specificity thresholds for incorporation into routine practice. 5 For patients with longstanding IBD, the role of dye-based chromoendoscopy in detecting dysplasia has been studied extensively. Several randomized controlled trials have shown a higher diagnostic yield for dysplasia compared to random biopsy protocols.8–10 However, at that time, HD-WLE, newer magnification technology, and electronic chromoendoscopy were still evolving. A consensus statement on dysplasia surveillance in patients with IBD strongly recommends dye-based chromoendoscopy over SD-WLE. 8 However, there is only a conditional recommendation over HD-WLE based on low-quality evidence from the single study available at the time. 8 Some experts have subsequently cast doubts about the universal implementation of chromoendoscopy in IBD.11,12 A large, 40-year analysis of 1375 patients with ulcerative colitis found that HD-WLE with random biopsies and chromoendoscopy both increased the rate of detecting dysplasia, but there was no improvement in the detection of colorectal cancer. 13 This raised concerns about the overdetection and potentially unnecessary overtreatment of lesions in certain IBD patients. 13 In addition, a large retrospective study of 775 patients over 13 years discovered that real-world adoption of dye-based chromoendoscopy did not result in an increase in dysplasia detection compared to WLE with random biopsies (most of which was SD-WLE). 10 Given these concerns, dye-based chromoendoscopy has not been universally adopted as the surveillance technique in all IBD patients, and further prospective studies are needed. 11
Autofluorescence Imaging
Autofluorescence imaging (AFI) is a wide-field imaging modality that takes advantage of endogenous molecules (fluorophores), which emit fluorescence when excited at specific wavelengths. Different tissues (i.e., neoplastic versus non-neoplastic) will contain different fluorophores, thereby generating an image in which normal mucosa appears green, while dysplastic or neoplastic tissue appears purple after software processing. 14
Unfortunately, the data regarding AFI in the
Confocal Laser Endomicroscopy
In contrast to the wide-field imaging modalities discussed so far, recent technical advances have made endomicroscopy possible. This refers to a set of emerging near-field technologies that allow for real-time, in vivo cellular and even subcellular assessment of tissue by trained operators. Confocal laser endomicroscopy (CLE) is one such modality that produces very high-magnification and high-resolution images of the superficial mucosal layer (Fig. 3). CLE is most commonly performed via a probe inserted through the standard working channel of the endoscope (pCLE) or a miniprobe through an endoscopic ultrasound needle (nCLE). 15 Endoscope-based CLE (eCLE) integrates the technology into the tip of an endoscope, but is no longer commercially available. 15 CLE takes advantage of the differential fluorescence and reflectance properties of tissue. It requires the use of a contrast agent, and although several topical agents have been studied, intravenous fluorescein has become the preferred option.2,15 Fluorescent light reflected from argon blue laser illumination is captured and processed to produce an over 1000 × magnified image, on the scale of a standard microscope. The pCLE image has a 240 μm by 240 μm field of view with a 55–65 μm depth and 12 frames per second image acquisition speed allowing for video quality imaging. 15
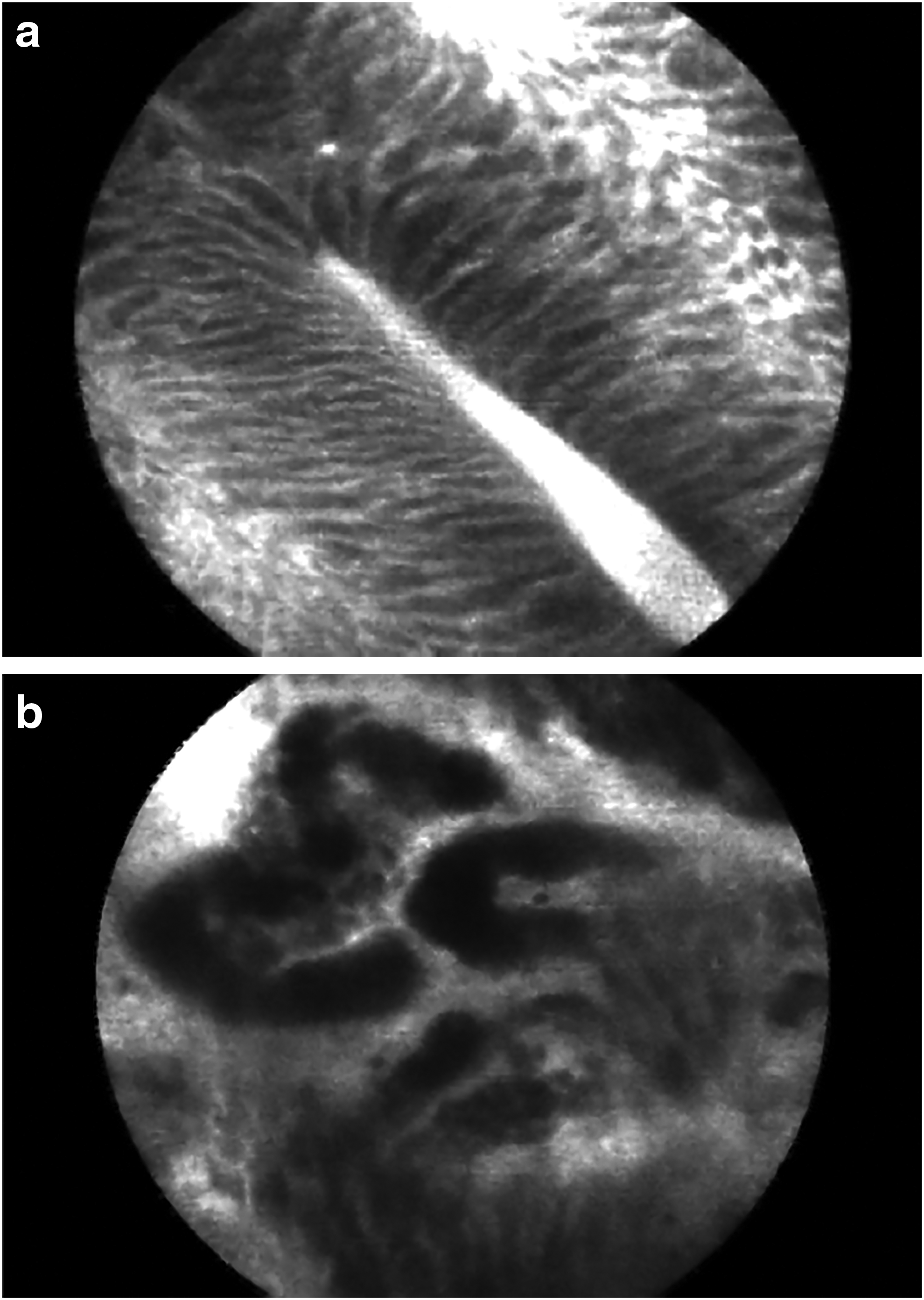
Confocal laser endomicroscopy image of Barrett's esophagus without dysplasia, characterized by uniform, organized villiform architecture
When combined with HD-WLE and targeted biopsies, eCLE was shown to reduce the number of required biopsies by 80% without a sacrifice in sensitivity for high-risk lesions, with high diagnostic yield and accuracy when compared to HD-WLE and random biopsies. 16 For pCLE, a meta-analysis reported a sensitivity of 90.3% and NPV of 95.1% in detecting dysplasia or esophageal adenocarcinoma for pCLE-targeted biopsies compared to a random biopsy protocol. 5
CLE also appears to be useful in other applications. For the evaluation of biliary strictures, studies have demonstrated that pCLE has an 80%–90% NPV for malignancy during endoscopic retrograde cholangiopancreatography, which is quite useful since inadequate tissue sampling remains a concern for endoscopists. 17 pCLE has also been proposed as a new method to verify mucosal healing in IBD. 17 nCLE, which uses a miniprobe that can be passed through a 19-gauge endoscopic ultrasound aspiration needle, may be helpful for differentiating between mucinous and nonmucinous pancreatic cysts. 15 Animal studies, human pilot studies, and early case series indicate that nCLE can also facilitate real-time characterization of solid tumors and lymph nodes.15,18–20 pCLE has also been used to characterize peritoneal nodules in laparoscopy and to evaluate bowel perfusion in animal models.21,22
A principal limitation of CLE is that with its small field of view, it is prone to sampling error and relies on precise placement of the probe or device on the targeted mucosa.2,15 Therefore, CLE usually requires a preceding wide-field examination to identify areas for closer inspection. When abnormal histology is identified by CLE, there is also the challenge of subsequently locating and correctly sampling the site of interest. Further improvements underway in CLE-based practice include tying it to a wide-field imaging technique to rapidly identify candidate lesions before performing closer histologic inspection.2,23 This may be achieved through molecular endoscopy, using agents that specifically bind abnormal tissues and highlight them (i.e., through fluorescence or reflectance) for closer inspection. 23 A variety of injectable or topical agents, including enzyme-activated probes, antibodies, peptides, and lectins, have been demonstrated in preclinical and clinical studies to target specific molecules in colonic adenomas, colorectal cancer, Crohn's disease, Clostridium difficile, Barrett's neoplasia, esophageal squamous cell cancer, and gastric cancer. 23
Optical Coherence Tomography/Volumetric Laser Endomicroscopy
Optical coherence tomography (OCT) is a technique that measures the tissue reflectivity of infrared light to develop high-resolution cross-sectional images of surface and subsurface structures of the
The second-generation OCT system, volumetric laser endomicroscopy (VLE; NinePoint Medical, Inc.) is available for use in BE. It consists of an OCT system in a 6-cm-long balloon mounted to an endoscopic probe, which is inserted through a standard working channel. An infrared light inside the inflated balloon spirals along the probe to scan the mucosa circumferentially in about 90 seconds. The light is reflected back to the probe to generate an image. This results in 1200 high-resolution, 360° cross-sectional images of the mucosa and submucosa of the esophagus, which can be reviewed in transverse and longitudinal views using the VLE software, akin to scrolling a computerized tomography scan (Fig. 4). The length of the probe and circumferential image provides a “full-field” view, as opposed to the near-field view of CLE. VLE also has an advantage, in that it shows subsurface architecture up to ∼3 mm deep rather than just the more superficial layers seen by CLE.24,25 Any abnormalities seen on VLE can be targeted for further endoscopic inspection, biopsy, or resection. The latest improvements in this device will incorporate laser marking of abnormal areas with the VLE probe to make it easier to subsequently biopsy or resect (Fig. 4).2,20
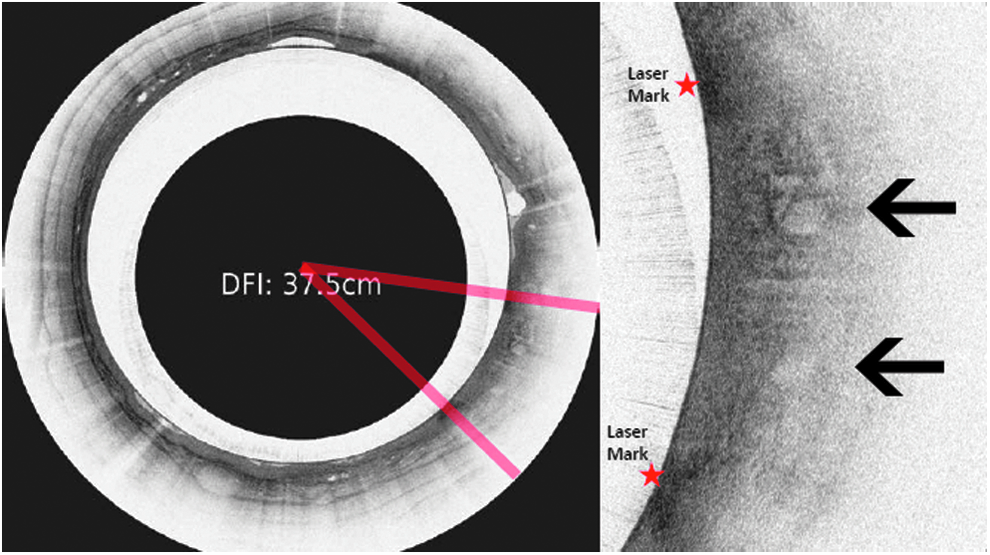
A volumetric laser endomicroscopy scan of Barrett's esophagus (cross-sectional view) with two areas concerning for high-grade dysplasia (black arrows). Images courtesy of NinePoint Medical.
Early studies of the first-generation OCT and more recently VLE have developed two scoring systems to correlate the imaging features with dysplasia, with sensitivities of each exceeding 80%.24,25 There is also evidence suggesting that VLE can be a valuable tool in preablation assessment of the esophagus by identifying lesions that need endoscopic mucosal resection as well as in predicting patients who may have prolonged or failed ablation. In addition, it may be used in postablation surveillance to detect residual or recurrent BE.2,25 Due to its depth of penetration, VLE can detect subsquamous intestinal metaplasia, also known as “buried glands,” after ablation, something only detectable at present with random biopsies. 2 However, further research with respect to outcomes, surveillance strategies, and correlation of in vivo VLE images with ex vivo pathology findings is needed.2,24,25 Additional studies of colonic and pancreaticobiliary applications are also underway. 25
Emerging Techniques
High-resolution microendoscopy (HRME) is a near-field technology, which produces subcellular images at a 1000-fold magnification. It requires a fluorescent agent sprayed on the mucosa before a fiber optic probe illuminates the tissue. The resulting fluorescence can be captured and converted to a real-time image. 26 This is similar to CLE, except that the fluorescent agent here can be applied topically and HRME uses a light-emitting diode rather than laser for illumination. HRME is still relatively early in its development, but a recent study demonstrated 94% accuracy, 95% specificity, and 87% positive predictive value in differentiating neoplastic from non-neoplastic colorectal polyps compared to HD-WLE (65%, 39%, and 55%, respectively). 26 Additional studies indicate that it is also reliable as an optical biopsy technique for esophageal squamous cell carcinoma and early gastric malignancies, while being relatively easy to learn and low cost. 27
Another emerging technology is endocytoscopy (EC), in which the mucosal layer is sprayed with a mucolytic and then a staining agent. Light reflected from the tissue is then magnified with a high-power objective lens to produce a histologic image of the most superficial layers of cells. EC has been studied in premalignant and malignant lesions in the esophagus, stomach, and the colon. Initial studies reported sensitivities ranging from 81% to 90% for diagnosing squamous esophageal neoplasia, 56%–86% for gastric neoplasia, and 79%–100% for colonic neoplasia.28–32 EC will need to be compared with other technologies, such as CLE, VLE, and HRME, in terms of accuracy and cost-effectiveness, and its precise role in the endoscopic assessment of these conditions remains to be determined. 33
Conclusion
There have been substantial improvements in imaging technologies over the past two decades as a result of innovations in digital sensors, visual displays, endoscope optics, and software processing. The “holy grail” of endoscopic imaging is a system that can combine a wide-field inspection of the GI tract (as with HD-WLE and NBI) with immediate near-field high-magnification inspection. Such a system will likely combine multiple imaging modalities and may utilize molecular endoscopy and advanced image processing software. An ideal wide-field modality would reliably identify red-flag areas for further investigation, such as using a safe and easy to use molecular probe and imaging enhancements. Real-time endomicroscopic inspection, ideally with subsurface imaging capabilities, could then be performed of these focal regions. The theoretic benefits of this approach include improved sensitivity for dysplastic lesions, a reduction in the number of required biopsies and pathology specimens, more appropriate selection of resection or ablation techniques in real time, and a reduction in the need for random biopsies and in the frequency of surveillance endoscopy. 2
In summary, although the above imaging technologies are conceptually appealing, clinical studies have failed to consistently demonstrate clear superiority of these modalities over a meticulous HD-WLE examination coupled with targeted and random biopsy protocols. 2 At present, these advanced imaging technologies complement a careful HD-WLE examination. Further studies of the utility and practicality of these devices in a community setting would be helpful, as the current studies have been performed at expert centers. Future innovation in this area will be driven by the need for improved outcome data, increased ease of use, and proven cost-effectiveness of these techniques. At present, however, these technologies should not be used as a substitute for a meticulous endoscopic inspection technique.
Footnotes
Disclosure Statement
No competing financial interests exist.