
Abstract
Abstract
Introduction:
Thoracoscopic repair of congenital diaphragmatic hernia (CDH) has been associated with faster recovery, earlier extubation, and decreased morbidity. Nevertheless, thoracoscopic repair is rarely attempted in the post-extracorporeal membrane oxygenation (ECMO) patient. Commonly cited reasons for not attempting thoracoscopy include concerns that the patients' respiratory status is too tenuous to tolerate insufflation pressures or that presumed defect size is so large that it precludes thoracoscopic repair. Our purpose is to review our experience with post-ECMO thoracoscopic CDH repair and evaluate the success of this approach.
Methods:
We performed retrospective analysis of attempted thoracoscopic CDH repairs after ECMO decannulation at our institution from 2001 to 2015. Primary outcome was rate of conversion. Secondary outcomes were intraoperative end-tidal CO2, time to extubation, and rate of recurrence.
Results:
We identified 21 post-ECMO patients in whom thoracoscopic CDH repair was attempted. Thoracoscopic repair was successfully completed in 28%. No patients had reported intolerance to insufflation at 3–7 mmHg. Average end-tidal CO2 at 15 operative minutes was 36.9 mmHg in the thoracoscopic group versus 50.7 mmHg in the open group and at 60 minutes was 34.25 mmHg versus 45.6 mmHg, respectively. One patient in the thoracoscopic group died and 1 experienced a large pneumothorax. In the converted group there was one clinically significant pneumothorax and three pleural effusions. Survivors after thoracoscopy were extubated an average of 5.6 ± 2.6 days after surgery versus 19.4 ± 10 days in the converted group (P < .05). Recurrence rates at last follow-up were equal between the two groups at 20%.
Conclusions:
Thoracoscopic CDH repair is both safe and feasible after ECMO with no increase in operative morbidity or mortality. Insufflation pressures of 3–7 mmHg are well tolerated without undue increase in end-tidal CO2. When compared to conversion cases, thoracoscopic repair is associated with significantly decreased time to extubation with no difference in recurrence.
Introduction
C
Repair of CDH can be performed open or with minimally invasive surgical (MIS) techniques. Thoracoscopy, the most common minimally invasive approach, has been associated with faster recovery, earlier extubation, and decreased morbidity when compared with open procedures.7,8 The major disadvantage is that it is difficult to close large hernias using MIS techniques. In addition, concerns over higher recurrence rates are common, although these results have never been verified with a randomized controlled trial.
The use of thoracoscopic repair in patients with a history of ECMO cannulation is debated. Many experts believe that these patients will not be able to tolerate this procedure for two reasons. The first is that insufflation pressures necessary for thoracoscopic repair will result in excessive hypercapnea and resultant acidosis which the post-ECMO neonate would not tolerate. The second is based on the belief that patients who require ECMO inherently have large defects, which necessitates the need for ECMO cannulation, and that such defects are too large to be repaired thoracoscopically.
Therefore, thoracoscopic repair is rarely attempted in the post-ECMO patient, and reports of this in the medical literature are sparse. The purpose of this study is to review our experience with post-ECMO thoracoscopic CDH repair, describe reasons for conversion to open repair, and evaluate the success of this approach.
Methods
After obtaining IRB approval, we identified all patients at Children's Healthcare of Atlanta (CHOA) who required ECMO before CDH repair between 2001 and 2015. CDH repairs were performed by 8 surgeons at a single site. Selection of procedure approach was at the discretion of the attending surgeon, and 6 of these surgeons attempted thoracoscopic repair at least once. At our institution, we typically do not perform CDH repair until after ECMO decannulation. We performed a retrospective analysis of the post-ECMO patients in whom thoracoscopic repair was attempted, excluding patients in whom thoracoscopic repair was never attempted, including unstable patients, those with Morgagni (anteromedial) type hernias, and those who underwent operation in the NICU. Data regarding operative time from post-ECMO CDH repairs in whom thoracoscopic approach was not attempted were collected for use in comparison to our primary group. We extracted demographic, operative, and outcome data from electronic medical records by reviewing patient histories and physicals, operative notes, and anesthesia records. Our primary outcome was rate of conversion. Secondary outcomes were reasons for conversion, intraoperative end-tidal CO2 at 15 minutes increments during the procedure, time to extubation, and rate of recurrence. We used descriptive statistics and performed a two-sample t-test to compare outcomes between the thoracoscopic group and the converted group.
Results
We identified 259 patients who underwent CDH repair during the identified time frame. Fifty-five of these required ECMO before repair. In 1 patient, the repair was performed while on ECMO; all others underwent decannulation before repair. Thoracoscopic repair was attempted in 21 and completed in 6. The remaining 15 cases were converted to open procedures for a minimally invasive completion rate of 28.5% (Fig. 1). Operative time was 175 ± 52 minutes in the thoracoscopic group and 142 ± 47 minutes in the converted group (P = .11). This compares to 141 ± 65 minutes in the cohort in whom an open approach was used initially. Paired T-tests demonstrate no significant difference between the three groups in terms of gestational age, age at repair, weight, length of ECMO run, patch use, or operative time (Table 1).
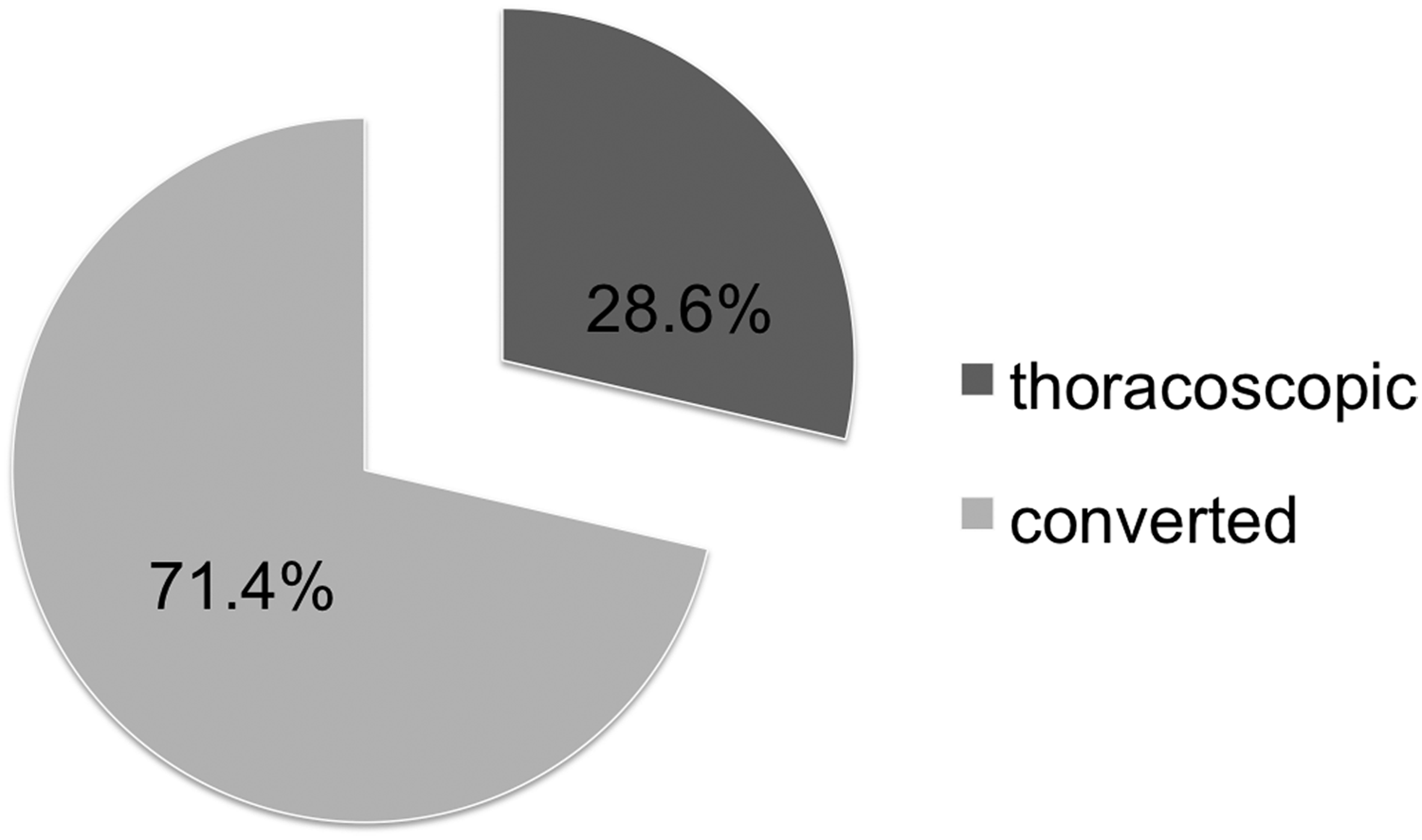
Thoracoscopic congenital diaphragmatic hernia repairs were successfully completed in 6 of 21 attempts after extracorporeal membrane oxygenation decannulation.
In all 15 of the converted cases, the reason for conversion was attributed to the size of the defect. None required conversion to an open procedure due to intolerance of insufflation pressures. Ten of the 15 patients tolerated insufflation pressures of 3–7 mmHg without clinical compromise. Four of 15 had no comment in the operative note about tolerance to insufflation pressures. One patient did not tolerate when the insufflation pressures were raised to 8 mmHg as a strategy to reduce the hernia. The reason for conversion in this case was nevertheless attributed to the defect size.
Average end-tidal CO2 at 15 operative minutes was 36.9 mmHg in the thoracoscopic group versus 50.7 mmHg in the open group. At 60 minutes end-tidal CO2 was 34.3 mmHg versus 45.6 mmHg, respectively. End-tidal CO2 averaged between 35 and 51 mmHg in thoracoscopic cases with no significant increases during insufflation (Fig. 2).

Post-extracorporeal membrane oxygenation patients did not experience dangerous increases in end-tidal CO2 during attempted thoracoscopic congenital diaphragmatic hernia repair.
Clinically significant pneumothorax and/or pleural effusion was defined as 1, which required chest tube placement. One patient in the thoracoscopic group had a significant pneumothorax. The converted group had one clinically significant pneumothorax and three pleural effusions, and the open group had six clinically significant pleural effusions and two pneumothoraces. One patient in the thoracoscopic group expired on postoperative day 3 due to sepsis. In the open group, there were 7 early deaths within the first 2 weeks postoperatively and 9 total deaths before discharge. Survivors in the thoracoscopic group were extubated 5.6 ± 3 days after surgery. The converted group had a time to extubation of 18.4 ± 10 days. Average time to extubation in the open group was 21.5 ± 15 days after surgery (Fig. 3). One-way analysis of variance (ANOVA) demonstrated a clinically significant difference between the MIS converted and primarily open groups at the P < .05 level [F(2, 25) = 3.35 P = .05]. Survivors in the thoracoscopic group were discharged 36.4 ± 6 days after surgery, the converted group had a time to discharge of 75.0 ± 29 days, and the open group had a time to discharge of 65.0 ± 46 days (Fig. 4). One-way ANOVA analysis did not demonstrate a clinically significant difference between the MIS, converted, and primarily open groups at the P < .05 level [F(2, 41) = 1.84; P = .17].
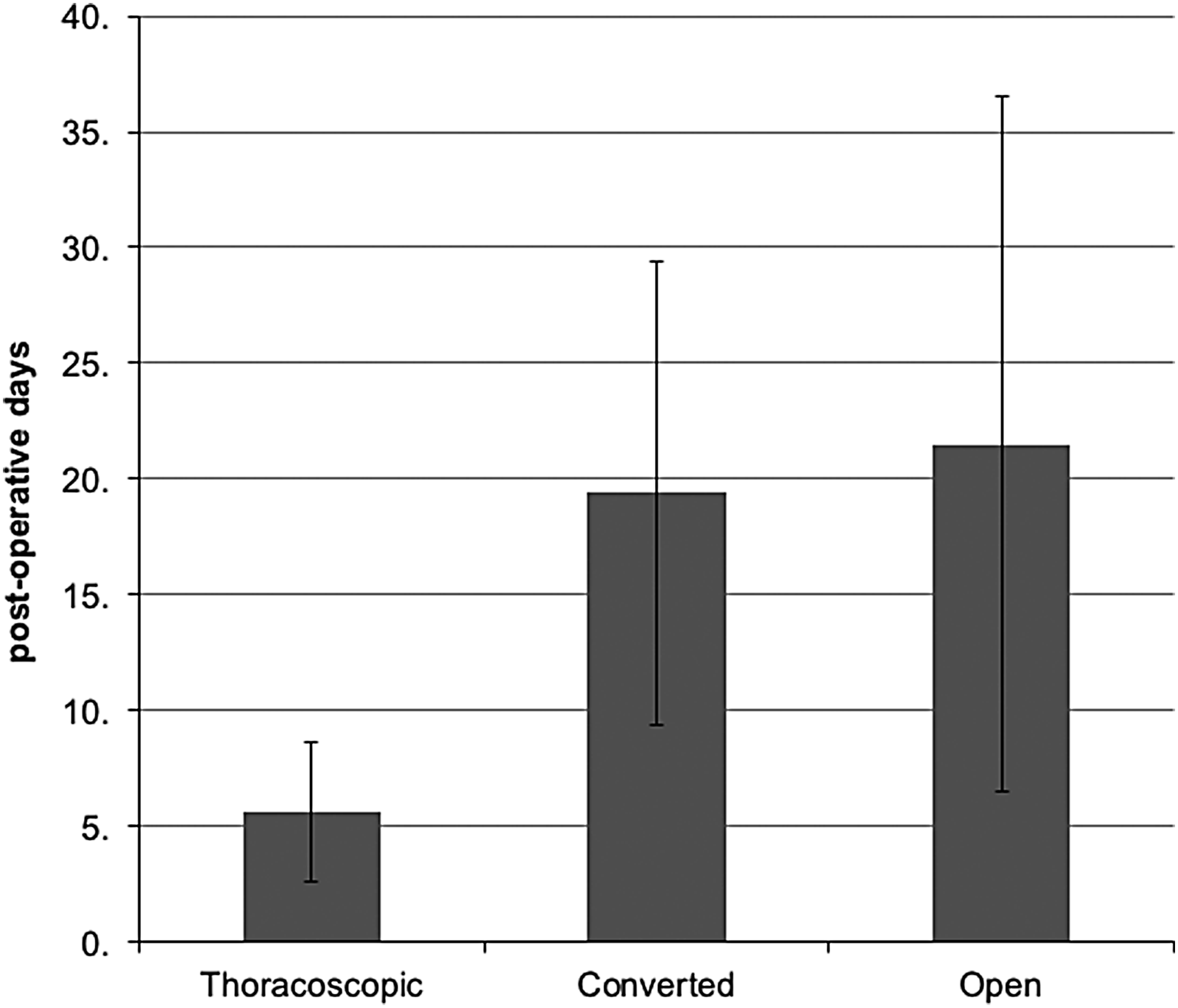
Time to extubation is shorter after thoracoscopic congenital diaphragmatic hernia repair than after open conversion in the postextracorporeal membrane oxygenation population.
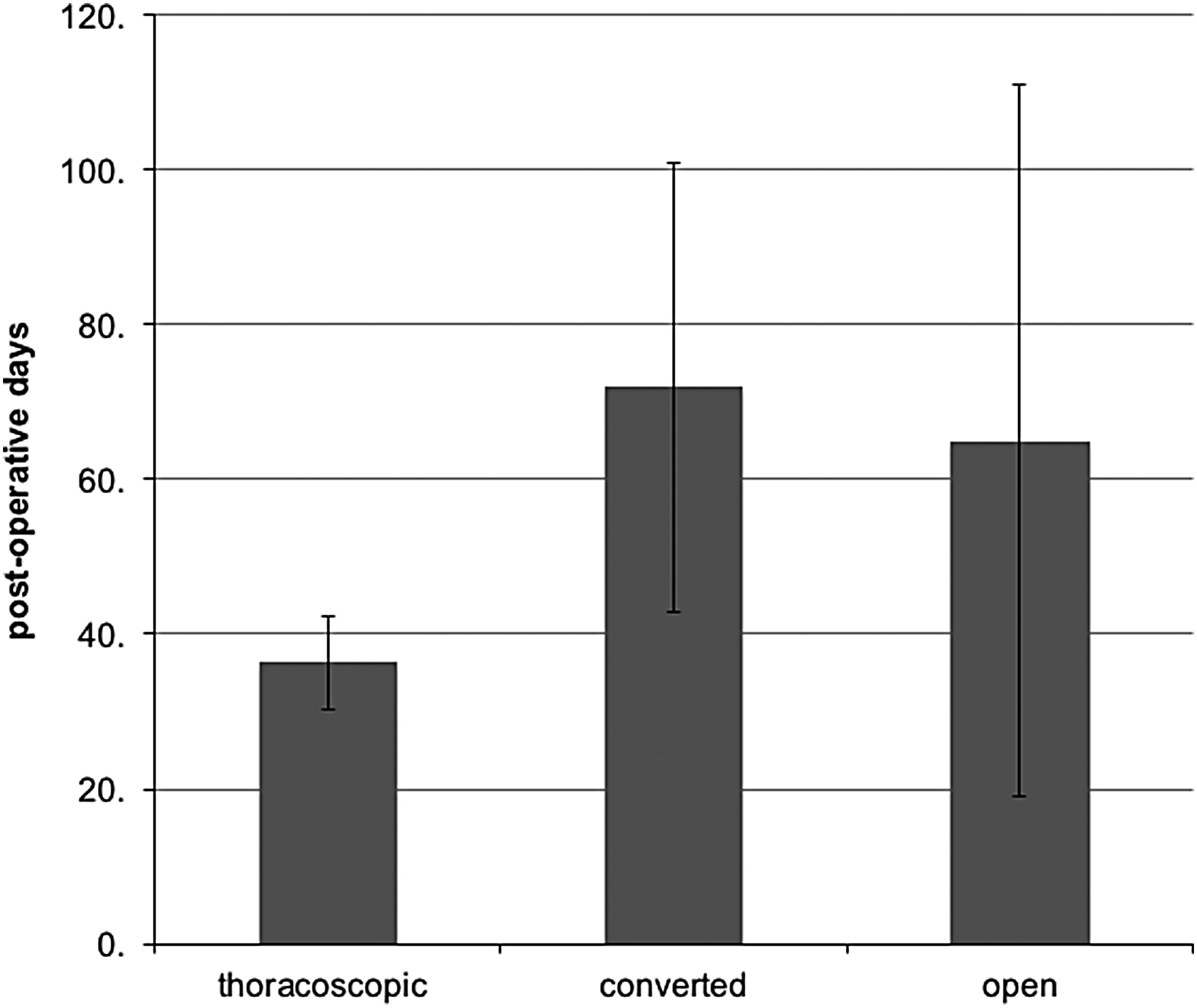
Time to discharge is shorter after thoracoscopic congenital diaphragmatic hernia repair than after open conversion in the postextracorporeal membrane oxygenation population.
A two-sample t-test showed a significant difference between the thoracoscopic group and the converted group (P < .01) and between the thoracoscopic group and the open group (P < .01), but not between the converted and open groups (P = .40).
Median time of follow-up was 2.1 years (range 1 month to 14 years). During this time, 1 out of 5 survivors in the thoracoscopic group and 3 out of 15 patients in the converted group had a recurrence, a 20% recurrence rate in each group. The rate of recurrence after primary open repair for post-ECMO patients was 24%.
Discussion
Numerous studies suggest that ECMO use improves survival in critically ill CDH patients with single-center series reporting survival rates of 33%–86% in the post-ECMO population.9–16 Although the thoracoscopic approach to CDH repair even in the non-ECMO population remains controversial, in some circles the potential benefits are well described. Studies have demonstrated a statistically significant improvement in time to extubation, return to full enteral feeds, and shorter postoperative hospital stays.7,8 These patients have lower narcotic and sedation requirements, less severe complications, and lower total adjusted hospital charges. 7 In the long term, they avoid the potential risk of scoliosis or chest wall deformities previously described after thoracotomy as well as the well-documented risk of adhesions following laparotomy.17,18
Recent literature has been indeterminate regarding timing of repair in infants with CDH requiring ECMO. Although some have observed increased survival, fewer circuit complications, and fewer intubated days than those repaired while on ECMO, data from the CDH study group and other single-center studies have shown increased mortality in the cohort repaired on ECMO along with higher incidence of bleeding and longer total ECMO time.9,11,19–24 Therefore, we choose to wait until decannulation to perform CDH repair.
Historically, it was believed that ECMO patients would not tolerate thoracoscopic repair. Several published protocols included “no ECMO requirement” as a criterion for attempting MIS repair.7,25,26 Two reasons for this are commonly cited: first is that patients who require ECMO are more likely to have large defects making MIS repair difficult, and second is the belief that these patients' tenuous respiratory status places them at high risk for decompensation under necessary insufflation pressures.
Before this study, there have been 5 published cases of thoracoscopic CDH repair after ECMO across three institutions, 2 patients in a thoracoscopic repair series by Kim et al. had previously required ECMO, and 1 of these cases was completed thoracoscopically. Cho et al. reported that 2 out of 10 successful thoracoscopic repairs were in post-ECMO patients, and McHoney et al. included 2 post-ECMO patients in 13 patients with attempted thoracoscopic repair, although they did not specify whether these were among the 5 cases converted to open repair. 20 Out of 21 attempted thoracoscopic repairs after ECMO at our institution, 6 were completed thoracoscopically making this the largest series of successful MIS post-ECMO repairs to date. While a stated conversion rate of 72% is concerning, our surgical approach involves a brief thoracoscopic assessment of the size and suitability of the diaphragmatic rim. Such assessment of the feasibility of MIS approach can be quickly performed, and then, the surgeon can immediately decide whether to proceed with MIS approach or convert to open procedure.
Every conversion in our study was attributed to large defect size. Although this correlates with the general consensus that patients requiring ECMO are more likely to have large defects, it dispels the claim that this trend precludes MIS repair in all such patients.
Although need for patch repair is classically associated with converted cases compared to successful MIS repairs, we were able to complete a patch repair thoracoscopically in 5 patients in this cohort. 20 The patch repairs in these patients were typically performed with primary closure of the diaphragm medially and use of mesh for the posterolateral aspect of the diaphragm. They all consisted of a biological patch underlay on the abdominal side of the diaphragm and Gore-Tex on the chest side of the repair. This patch combination has been the primary practice at the institution for both open and MIS cases. The Gore-Tex provides strength, and the SIS adds an overlapping layer with potential to increase ingrowth and further solidify the repair.
Others claim that post-ECMO patients will not tolerate the physiologic changes associated with thoracoscopic repair. The minimally invasive approach has been associated with more intraoperative hypercapnea and acidosis than an open approach, most likely due to the combined effects of limited chest wall expansion and absorption of CO2 used for insufflation.7,23,25 One study, however, demonstrated that while EtCO2 was significantly elevated during thoracoscopy, this shift was not reflected in serum pH or arterial CO2 levels and the authors argued that EtCO2 overestimates PaCO2 in these patients. 20 Another cohort study demonstrated that despite increased acidosis and higher peak inspiratory pressures (PIP) intraoperatively, patients undergoing thoracoscopic repair had lower PIP on postoperative day 1, shorter ventilator time, and lower requirement of supplemental oxygen postoperatively. 7 In our patients, there was no recorded intolerance of insufflation pressures from 3 to 7 mmHg, with intraoperative EtCO2 ranging from normal to mildly elevated. There were no significant increases in EtCO2 during insufflation and no conversions reported due to cardiorespiratory instability. This challenges the claim that hypercapnea and intolerance of insufflation pressures contribute significantly to inability of post-ECMO patients to undergo thoracoscopic repair.
Cases completed thoracoscopically were longer than converted cases averaging 175 minutes versus 142 minutes, respectively. This is consistent with reports in the general CDH population, in which MIS repairs average between 120 and 198 minutes and the average length of open repairs ranges from 90 to 143 minutes.8,17,18,20,23,24,27,28 In addition, it is well established that operative time for MIS procedures decreases with institutional experience. 8
It should be noted that the observational nature of this study introduces the risk of selection bias. The decision to attempt MIS repair was at the clinical discretion of the attending surgeon, and as such, there was significant heterogeneity between individuals in the rate of thoracoscopic attempts and successful thoracoscopic repairs. While MIS repairs were attempted throughout the time period of the study, the global trend of increasing MIS procedures was reflected in a slight trend toward attempting MIS repair in later years in the post-ECMO cohort. Therefore, it is possible that improved neonatal care during this time confounded the effect of the procedure itself to improve outcomes. However, the similarity in outcomes between the converted and open groups suggests that the difference may be related more to the procedure type or to the patient characteristics than to the time period in which it was performed. There did not appear to be neither a correlation between surgeon experience and the decision to attempt thoracoscopic repair, nor strong evidence that surgeon experience was a driving factor in likelihood of successful MIS repair. As noted in Table 1, there were no age or weight parameters suggestive of the likelihood of successful thoracoscopic repair. Therefore, further study with a larger cohort is warranted to elucidate which post-ECMO CDH patients are the best candidates for MIS repair.
The main benefit of thoracoscopic repair appears to be the significant decrease in time to extubation. This benefit ultimately allows patients to have a shorter hospital stay. Previous studies have demonstrated shortened ventilator time and length of stay after MIS CDH repair when compared with open repairs. 7 Our study corroborates this in the post-ECMO subset of patients with a significantly faster time to extubation and time to discharge in the thoracoscopic group. The data from our open group (average 19.4 days) are consistent with the data from the Congenital Diaphragmatic Hernia Registry (CDHR) average extubation time of 16.5 days. As the primary reason for conversion in our group was large defect size, this raises the question of whether the improved outcomes in the MIS group may be attributed solely to favorable defect rather than surgical approach. In evaluation of the CDHR post-ECMO population, 5% of these patients had defect size A as categorized by the Congenital Diaphragmatic Hernia Study Group (CDHSG) staging system. Even in these patients, average time to extubation was 12.3 ± 12 days; our mean of 5.6 days after MIS repair suggests that minimally invasive approach itself offers additional benefit.
One patient in our minimally invasive group died of sepsis, amounting to a 5% early mortality rate among those with attempted thoracoscopic repair and a 17% rate among those with successful thoracoscopic repair. Among those post-ECMO patients in whom thoracoscopic repair was not attempted, there was an early mortality rate (within 2 weeks of surgery) of 14.0%, and 9 patients (26.5%) died before discharge. Although statistical generalizations are difficult in such a small cohort, this is comparable to the one death experienced in the MIS group. The cause (sepsis) is a risk inherent to all critically ill infants. In addition, it should be noted that this death along with half of the deaths in the open group occurred within the first 4 years of data collection, indicating that improved neonatal care may play a role in decreasing the risk of death postoperatively in this fragile population.
Recurrence rates after thoracoscopic CDH repair are reported between 9% and 40% overall.9,29–32 Most comparative studies report relatively higher rates of recurrence with MIS repairs versus open repairs; high case volume and improved experience, however, narrow the gap between the two.7,17,20,21,26–28 There was no difference in recurrence rates between the thoracoscopic repairs and the converted repairs in our cohort, with 20% of each group experiencing a recurrence in comparison to 24% of the open group. In addition, patients undergoing thoracoscopic repair avoid the morbidity of scoliosis associated with thoracotomy and adhesive obstruction complications from laparotomy. 31
Our outcomes suggest that there is no evidence of harm and there can be a significant benefit from attempted thoracoscopy in post-ECMO CDH patients. As this study consisted of a small sample size at a single institution, multicenter studies should be pursued to further delineate the success of this technique in the post-ECMO population. It is also important to further evaluate the difference in operative time observed between the two procedures. In addition, we offer a note of caution regarding the high conversion rate, which may be alleviated in the future with better identification of MIS candidates and center experience. A higher powered study may be able to observe the effect of the learning curve inherent to all minimally invasive procedures, with operative time decreasing with experience, as well as identify factors associated with successful completion of MIS CDH repairs in the post-ECMO population.
Conclusions
Thoracoscopic CDH repair is both safe and feasible after ECMO with no increase in operative morbidity or mortality. Insufflation pressures of 3–7 mmHg are well tolerated in post-ECMO CDH patients without undo increase in end-tidal CO2. When compared to conversion cases, thoracoscopic repair has a significant benefit in time to extubation and time to discharge. Our outcomes suggest that there is no evidence of harm, and there can be a significant benefit from attempted thoracoscopy in post-ECMO CDH patients. As this study consisted of a small sample size at a single institution, multicenter studies should be pursued to further delineate the success of this technique in the post-ECMO population.
Footnotes
Disclosure Statement
No competing financial interests exist.