
Abstract
Abstract
Background:
The treatment of achalasia is palliative. Pneumatic dilatation (PD) or laparoscopic Heller myotomy (LHM) just eliminates the outflow obstruction allowing easier emptying of the esophagus. The aim of this study was to evaluate the results of a multidisciplinary approach to esophageal achalasia.
Materials and Methods:
A consecutive series of patients with achalasia treated by a multidisciplinary esophageal team consisting of radiologists, gastroenterologists, and surgeons in a quaternary care center between May 2008 and April 2015 were analyzed.
Results:
A total of 147 patients with achalasia underwent LHM and partial fundoplication. Sixty-two patients (42%) had been treated preoperatively with PD and/or botulinum toxin (BT). The preoperative Eckardt score (ES) was 6.4 ± 2. At a median follow-up of 22 months, 128 patients (87%) did well and required no further treatment (ES 0.1). The remaining 19 patients (13%) had recurrence of symptoms and required further treatment: 12 were treated with PD and improved (ES 0.7); 4 were treated with PD and BT and improved (ES 1.3); 3 failed PD. These 3 patients had been treated with multiple sessions of PD and BT before the myotomy. Overall, 144 patients (98%) did well with laparoscopic (87%) or laparoscopic and endoscopic treatment (11%).
Conclusions:
The results of this study show that (a) LHM is an effective treatment modality, (b) PD improved symptoms in the majority of patients with recurrent dysphagia after myotomy and (c) multiple preoperative endoscopic treatments seem to affect outcomes of LHM. Patients with achalasia should be treated in a quaternary care center by a multidisciplinary team.
Introduction
S
Eight years ago we created a Center for Esophageal Diseases, with the goal of combining the experience of experts from different disciplines to treat patients with benign and malignant esophageal disorders. For esophageal achalasia, we specifically decided to use an LHM as primary form of treatment for untreated patients. We also performed an LHM in patients referred to us after failing other treatment modalities such as PD and intrasphincteric injection of botulinum toxin (BT). We hypothesized that, thanks to a multidisciplinary approach, we could improve the swallowing status of these patients, limiting the need for esophagectomy.
Materials and Methods
Patients referred to the Center for Esophageal Diseases for evaluation and treatment of esophageal achalasia between May of 2008 and April 2015 were included. All patients underwent symptomatic evaluation based on the Eckardt score (ES), barium swallow, upper endoscopy, esophageal manometry, and often ambulatory pH monitoring. The LHM was about 7–8 cm long, and extends for 2.0–2.5 cm onto the gastric wall. Intraoperative endoscopy was not routinely performed. A Dor fundoplication was added to the myotomy as previously described. 13
Patients were seen in clinics 2 weeks postoperatively and subsequently contacted by e-mail if they were doing well. They were instructed to contact us as soon as they noted a change in their swallowing ability, without waiting for severe dysphagia to develop. In patients with recurrent symptoms, a complete work-up was done, including a barium swallow, an endoscopy, esophageal manometry, and pH monitoring. The possibility that one or more PDs were necessary after the operation was discussed with all patients.
Results
A total of 147 patients with achalasia underwent LHM and partial fundoplication. There were 79 men and 68 women and the mean age was 48 years. Patients had been symptomatic for an average of 66 months. Before referral, 62 patients (42%) had been treated with PD and/or BT. The preoperative ES was 6.4 ± 2. The barium swallow showed a picture suggestive of achalasia in 126 patients (86%). Upper endoscopy ruled out the presence of a peptic stricture and cancer in all patients. Conventional manometry with water perfused catheters was performed in 58 patients that showed absence of peristalsis and a nonrelaxing LES. High-resolution manometry was performed in 89 patients that showed type I achalasia in 14 (16%) patients, type II in 69 patients (77%), and type III in 6 patients (7%) (Table 1). When heartburn was present, ambulatory pH monitoring confirmed the absence of pathological gastroesophageal reflux. An LHM and a Dor fundoplication were attempted in all patients. In 2 patients, the operation was converted to open surgery because of bleeding (1 patient) or severe intraperitoneal adhesions secondary to prior operations (1 patient). Five patients (3.4%) had an intraoperative mucosal perforation that was repaired laparoscopically without sequelae. Median length of hospital stay was 23 hours.
BT, botulinum toxin; PD, pneumatic dilatation.
At a median follow-up of 22 months, 128 patients (87%) were doing well with an ES of 0.1. The remaining 19 patients had recurrence of symptoms and required additional treatment: (a) 12 patients were treated with PD alone (median 2 PDs/patient) and improved ES of 0.7, a 20 mm balloon was used in 11 patients and a 30 mm balloon in 1 patient; (b) 4 patients were treated with a combination of PD (median 2 PDs/patient) and BT (one session/patient) and improved ES of 1.3; and (c) 3 patients failed PD and BT, and 2 underwent esophagectomy. They are both asymptomatic. One patient refused additional treatment. These 3 patients had been treated preoperatively with multiple sessions of PD and BT (average four PDs/patient and three BT injections/patient) before having the LHM. At the time of the LHM, severe fibrosis was found at the level of the gastroesophageal junction with loss of the normal anatomic planes. In 1 case, the mucosa was perforated and was repaired.
Overall, 144 patients (98%) were doing well after laparoscopic myotomy (87%) or after a combination of laparoscopic and endoscopic treatment (11%) (Table 2).
BT, botulinum toxin; PD, pneumatic dilatation.
Discussion
The results of this study show that (a) in patients who have failed PD and/or BT, an LHM is technically more difficult and the results are less predictable; (b) LHM is an effective treatment modality in most patients with achalasia; and (c) PD improved symptoms in the majority of patients with recurrent dysphagia after myotomy, avoiding the need for esophagectomy.
Heller myotomy after prior endoscopic treatment
Our report confirms the findings of other studies, showing that prior endoscopic treatment makes a Heller myotomy more challenging and less effective.14–20
In 1999, Patti et al. showed that preoperative treatment with BT created in some patients (particularly in those who had a temporary response) a fibrotic reaction at the level of the gastroesophageal junction, with loss of regular anatomic planes. 14 In their experience, the operation was successful in 91% of patients who had not been treated with BT but in only 50% of those who had been treated with BT with a temporary response. 14 The detrimental effect of BT has been documented by other studies.15–19 For instance, Smith et al. compared the outcome of LHM of 154 patients treated preoperatively (100 patients, dilatations only; 22 patients, BT only; 21 patients, both) with that of 55 patients in whom the LHM was the primary form of treatment. 16 When comparing the two groups, the following findings were evident, confirming that preoperative treatment is associated with worse results: (a) intraoperative complications, 9.6% versus 3.6%; (b) postoperative complications, 10.4% versus 5.4%; and (c) failure of the myotomy, 19.5% versus 10.1%. Our 2 patients who required an esophagectomy had multiple sessions of BT and PD before the LHM was attempted. The operation was technically challenging, as a major amount of fibrosis was present with the obliteration of the normal anatomic planes.
Considering that the evidence against the BT is very strong, we and others feel that the continuous use of BT by the gastroenterological community is quite concerning.14–19 In addition, its use is against the guidelines of the American Gastroenterological Association for the treatment of achalasia, published in 2013. 20 These guidelines clearly stressed that “botulinum toxin should not be employed as first line in patients with achalasia who are candidates for either pneumatic dilation or myotomy. It may increase inflammatory reaction in the mucosa and muscle plane resulting in a higher rate of surgical complications and increased difficulty in subsequent surgical myotomy.” 20 It is appalling that many gastroenterologists still use BT in almost every patient, and that this procedure is reimbursed by insurance companies.
LHM is an effective treatment modality in most patients
Our team decided that an LHM was the primary form of treatment in our Center for patients with achalasia, with PD reserved for patients who did not want to have an operation or for those who experienced recurrent symptoms. This decision was based on two main considerations: (a) the senior surgeon involved in the study had performed LHM for many years with good results and (b) review of the literature shows that even when there is a similar level of expertise with both PD and LHM, the surgical approach often gives better results. In 2011, Boeckxstaens et al. published the 2-year results of a prospective and randomized European trial comparing PD with LHM. 21 Good results (ES < 3) were obtained in 86% of patients after PD and in 90% of patients after LHM. A similar outcome was documented at 5-year follow-up, 82% and 84%, respectively. 9 These results, however, were not confirmed by another prospective and randomized trial conducted in Sweden by Persson et al. while comparing LHM and repetitive PD. 8 At 5-year follow-up, failures occurred in 36% of patients after PD but in only 12% of patients after LHM (P = .025). The superiority of LHM has also been confirmed by three large meta-analyses.4–6 For instance, Campos et al. showed good relief of dysphagia after 36 months in 58% of patients after PD but in 89% of patients after LHM. 4 Postoperative reflux occurred in < 9% of patients after LHM.
PD for the treatment of recurrent dysphagia after LHM
In our study, 128 patients (87%) had an ES of 0.1 after a median follow-up of 22 months. The remaining 19 patients required additional treatment. Before the operation, we discussed with the patients the possibility of having recurrent symptoms. In particular, if they felt that dysphagia was slowly reappearing, we instructed them to contact the Center and to schedule an appointment with either a surgeon or a gastroenterologist without waiting for severe dysphagia to occur. Patients underwent a work-up that included barium swallow, endoscopy, and manometry. The recurrent dysphagia was always treated initially by PD. We did not wait for symptoms to be severe (ES > 3), but we treated patients when we felt that the symptoms were getting progressively worse. This approach was very effective as 98% of patients were doing well with either an LHM alone or a combination of LHM and PD. Other studies have shown that problems usually tend to manifest during the first 12 months after an LHM, and that most are amenable to esophageal dilatation.2,17 For instance, Zaninotto et al. noted recurrence of dysphagia in 39 of 407 patients (9.6%) after LHM and Dor fundoplication. 2 PD was successful in resolving the dysphagia in 30 patients (77%). Overall, considering both the LHM and the postoperative PD, the success rate of treatment was 98%. Sweet et al. also reported the efficacy of dilatation for recurrent dysphagia. In their study, the combined treatment had a success rate of 90%, and no patient required an esophagectomy. 17
In our Center, we did not have experience with POEM, which seems to be effective to treat recurrent dysphagia after LHM.22,23 The use of POEM makes sense, as the LHM is usually performed on the anterior wall of the esophagus, whereas POEM can be performed on the posterior wall of the esophagus. For instance, Onimaru et al. used POEM to treat successfully 10 patients who had recurrent dysphagia after LHM. 22 At 3-month follow-up, the ES decreased from 6.5 ± 1.3 to 1.1 ± 1.3. Longer follow-up will be needed to confirm the validity of these short-term results.
Owing to the success of endoscopic treatment, we did not perform a redo myotomy in patients with recurrent dysphagia. In expert hands, a redo myotomy has a good success rate, particularly in patients in whom the first myotomy was done through a left chest approach, but it is a complex operation that might be complicated by damage of the exposed mucosa with need for an esophagectomy when the first myotomy was done through the abdomen.24,25
As it was the case in our experience, some patients eventually require an esophagectomy. Even though the operation is done for a benign condition, it may be very challenging because of the diameter of the esophagus and of the presence of enlarged feeding vessels in the mediastinum. Devaney et al. from the University of Michigan reported their experience with esophagectomy for esophageal achalasia. 12 Even in very expert hands, the complication rate was very high: anastomotic leak, 10%; recurrent laryngeal nerve injury, 5%; need for thoracotomy to control bleeding, 2%, and chylothorax, 2%. In addition, nearly 50% of patients had postoperative dysphagia and required an anastomotic dilatation. There were two hospital deaths from respiratory insufficiency and death. We used a hybrid Ivor Lewis approach (laparoscopic preparation of the stomach followed by right thoracotomy) for the 2 patients who required an esophagectomy, performing the anastomosis at the apex of the right chest. They are both swallowing without problems. Figure 1 summarizes our treatment algorithm for patients with achalasia.
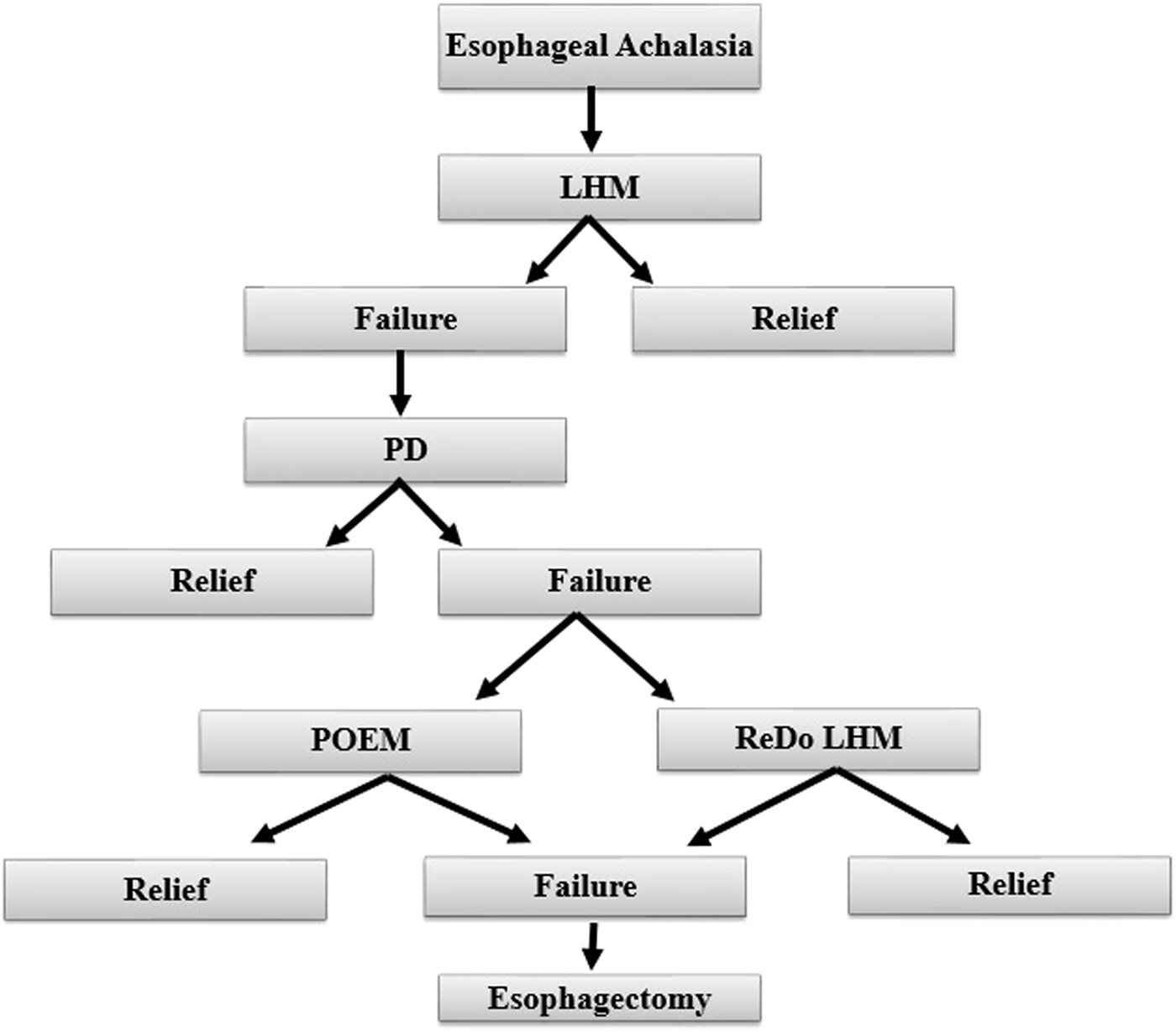
Treatment algorithm for esophageal achalasia. LHM, laparoscopic Heller myotomy; PD, pneumatic dilatation; POEM, peroral endoscopic myotomy.
Our study has some limitations. First, it is a retrospective study from a single institution. Second, it includes a limited number of patients. Third, the length of follow-up is about 2 years, and a longer follow-up will be necessary to determine whether these results will last over time. Finally, POEM was not part of the treatment algorithm.
Even with these limitations, we feel that our study supports the concept of treating patients with achalasia in Centers where the surgeon is part of a team of physicians who share experience and expertise in the treatment of this disease.
Footnotes
Disclosure Statement
No competing financial interests exist.