
Abstract
Abstract
Background:
Most kidney neoplasms are found incidentally and qualify for nephron-sparing surgery. Laparoscopic approach is beneficial to these patients because of its minimally invasive approach. However, these operations are both difficult and require plenty of experience and extended training. Some stages of the operation are limited by permissible time of transient ischemia. We applied three-dimensional (3D) printing technology to create individual silicone models of kidney to be used for training in laparoscopic procedures before the actual surgeries.
Materials and Methods:
Three patients who qualified for laparoscopic partial nephrectomy were selected. Digital models of their kidneys with tumors were designed based on computed tomography scans, followed by creation of silicone models. These were cast into the forms printed in 3D. The proper surgery was preceded by an operation carried out in a silicone model of laparoscopic simulator in which the tumor was excised and lodged after tumorectomy was filled.
Results:
Average time of the live kidney tumor operation was slightly shorter than that of the silicone model (16 versus 17 minutes). Relatively short period of ischemia did not exceed 9 minutes. One patient underwent surgery without closing the vascular pedicle.
Conclusions:
Experience gained during training with these silicone models improved the actual surgery and can reduce the need for/duration of intraoperative renal ischemia. We believe this training method can be successfully used in other procedures.
Introduction
R
Materials and Methods
Three patients qualified for LPN (Table 1). Digital models of their kidneys with tumors were designed using the 3D Slicer program (Surgical Planning Lab, Boston, MA) based on CT scans. Next, STL files of virtual kidney models were imported to the TinkerCAD software (Autodesk, San Rafael, CA) to design casting molds of kidneys and tumors separately; these were used to prepare ISMs. Forms were prepared with 3D printing technology using the Replicator 2 device (MakerBot Industries, LLC) (Fig. 1). Polylactic acid filament was used for printing, with layer thickness of 0.2 mm. The total time of forms production ranged between 7 and 8 hours; the printout of kidney and tumor forms took 4 hours 15 minutes and 55 minutes, respectively. Commercially available Elite Double 8 (Zhermack SpA, Italy) was used as silicone material; the physical properties of this product corresponded well to the kidney parenchyma. Preparation of the ISM took 1 hour. Tumor was attached to the kidney using silicone adhesive. 8 The model of each kidney with tumor was affixed onto a tripod, simulating the retroperitoneal approach (Fig. 2). Surgeries of ISMs were performed in a laparoscopic simulator using a video channel (Olympus Europa Holding GmbH, Germany). Three ports, including camera, were used. During the first stage, the tumor was resected in the silicone adhesive layer, followed by application of continuous sutures (Fig. 3). The next day, an operator performed surgery on the live kidney according to the scheme applied the previous day.

Forms for casting silicone kidney and silicone tumor printed out applying 3D technology. 3D, three-dimensional.

Silicone kidney—prepared for surgery applying training simulator.
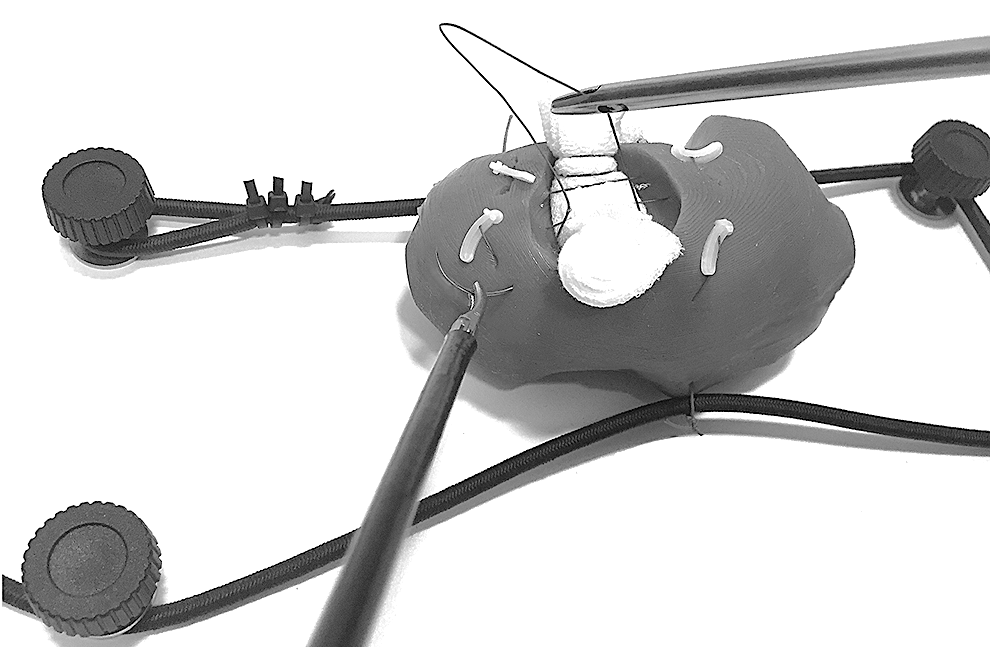
Silicone kidney—resection of tumor with suture on the site of the resection.
Results
Training took 17 minutes on average (15–19 minutes). On average, removal of live tumor and hemostasis took 16 minutes. In 1 case, ischemia was not induced; in the remaining 2 cases, the renal pedicles were closed briefly for 7 and 9 minutes, respectively. Hemostasis was achieved with the application of monopolar coagulation, Tachosil (Takeda GmbH, Austria) surgical roller and Vicryl 1-0 suture. Our patients lost 280 mL of blood on average. The total time for each procedure ranged between 80 and 105 minutes. Patients were discharged well from the hospital on the third postoperative day. Pathological evaluation of all cases revealed RCC Furman Grade 1 with negative surgical margins.
Discussion
PN is the current standard method of treatment of T1a kidney tumors. The laparoscopic technique is beneficial because of its minimally invasive methodology. Many studies have shown that LPN is associated with shorter hospitalization, convalescence, and reduced use of narcotics. 9 However, LPN requires great experience and involves a higher risk of intraoperative bleeding and longer duration of induced renal ischemia. To expedite the surgical procedure, reduce complications, and shorten the duration of ischemia, advanced methods including 3D virtual imaging, intrasurgical ultrasonography, and advanced real time intrasurgical navigation systems have been applied. 10 However, laparoscopic skills acquired from training with animal models or simulators depart from reality. Reports on printing individual kidney models based on patients' CT scans have recently been published. 11 These enable better recognition of the kidney and tumor anatomy and better surgical planning. However, the solid materials used in 3D printing limit further use of the models printed out. Thanks to 3D printing, we created multiple-use forms to prepare silicone kidney models, which can be used in simulations of surgical procedures. Properties of the commercially available Elite Double 8 were found to be very similar to those of a live kidney. Proper flexibility and mechanical resistance enable cutting of the model and suturing without the risk of spontaneous damage. During training, special attention was paid to the location of the tumor, availability of laparoscopic instruments, depth and shape of the site of the removed tumor, and the optimal techniques of tumor resection and suturing. During the actual surgery, identical topography of the kidneys and tumors was encountered; this enabled us to safely perform the same procedure conducted the day before. The experience gained from training with the ISM accelerated the actual surgery; in 1 patient, the essential stages of the procedure were performed without the need of renal ischemia; in the remaining 2 patients ischemia did not exceed 9 minutes.
In our opinion, creating individual kidney models brings new possibilities to laparoscopic education. This is especially essential in centers that rarely perform LPN. Surgical training before the actual procedure may shorten the duration of ischemia, which remains a debated issue between open and LPN. The technique may also be successfully used in other procedures. Thanks to its printed form, ISMs can be duplicated. This allows the same surgical training to be performed as many times by as many operators at various centers as possible. Interesting clinical cases can be archived this way and used to provide training for new residents or testing of subsequent surgical techniques or instruments. The low cost of creating the models (∼100 Euros), short production time, and the use of low-cost 3D printers are also worth emphasizing.
Footnotes
Acknowledgment
We specially thank the President of the Polish Association of Urology.
Disclosure Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethics board approval number is KB-0012/140/04/16. The authors declare that no competing financial interests exist. Informed consent was obtained from all individual participants included in the study. This article has not been published and is not under consideration by another journal.