
Abstract
Abstract
Background:
Endoscopic sphincterotomy (ES) is the standard technique for common bile duct (CBD) stone removal. Recently, endoscopic papillary large balloon dilation (EPLBD) has been shown to be a safe and effective technique for the removal of large CBD stone. The aim of this study was to determine the therapeutic outcomes and safety of EPLBD compared with ES for large CBD stone extraction.
Patients and Methods:
One hundred twenty-four patients with large bile duct stones were randomized into two groups, the first group included 61 patients subjected to EPLBD and the second group included 63 patients who underwent ES. We compared the success rate of stone removal, frequency of mechanical lithotripsy requirement, morbidity, and mortality.
Results:
Baseline characteristics were not significantly different. The overall ductal clearance rate was ultimately similar between the EPLBD group (96.7%) and the ES group (93.7%) (P = .53), the one session ductal clearance rate was significantly different (86.9% versus 71.4%; P = .01). Requirement of mechanical lithotripsy was significantly different between the EPLBD and ES group (9.8% versus 17.5%, P = .04). There were no differences in complication rates between the EPLBD and ES group; pancreatitis, 4.9% versus 6.3%; minor hemorrhage, 1.6% versus 6.3%; acute cholangitis, 3.3% versus 1.9%; and recurrent stones, 3.3% versus 3.2%.
Conclusions:
The therapeutic outcomes of EPLBD for removal of large bile duct stones are better than those of ES with comparable complication rate. EPLBD is also recommended for removal of large CBD stone in patients with an underlying coagulopathy or need for anticoagulation following endoscopic retrograde cholangiopancreaticography.
Introduction
E
Combined endoscopic papillary large balloon dilation (EPLBD) with ES was used in clinical practice in 2003 by Ersoz et al., 10 where a large-diameter dilation balloon (12–20 mm) are used to remove large bile duct stone. This combination would theoretically combine the benefits of both techniques while minimizing their complications. 11 It is rapidly and widely being accepted as an efficient and safe technique for the removal of large or difficult bile duct stone.12,13 However, hemorrhage associated with ES and recurrent stone secondary to patulous ampullary opening are problematic late complications that remain to be solved. 14 EPLBD without ES was recently applied as an alternative technique in 2009. 15 Potential advantages of EPLBD alone include some preservation of the sphincteric function with subsequent decrease of stone recurrence and lower risk of hemorrhage. 14 Recently, although many studies have revealed the encouraging safety and efficacy of EPLBD for CBD stone removal, 16 many gastroenterologists are hesitant to accept this technique, and ES is still the standard and most frequently used method for retrieval of choledocholithiasis. Therefore, we performed the present study to compare between EPLBD and ES in the removal of large CBD stone regarding therapeutic outcomes and safety.
Methods
This prospective study was performed on 124 patients with large CBD stone (>1 cm) between August 2014 and August 2016. Our exclusion criteria included the following: age younger than 18 years, patients with contraindication to endoscopic retrograde cholangiopancreaticography (ERCP; history of contrast dye anaphylaxis, severe cardiopulmonary disease, and recent myocardial infarction), acute pancreatitis or cholangitis at the time of the procedure, previous history of ES, concomitant cholangiocarcinona or stricture, or intrahepatic stone.
The number of patients needed was calculated. Considering a power of 80% and reliability of 0.05, we found that 55 patients should be present in each group. The study was started with 296 patients for the possible loss of patients and data during the study. Eligible patients (158 patients) were randomly divided equally into two groups (Group 1: EPLBD; Group 2: ES) according to a computer-generated random numbers. Of 79 patients allocated to intervention in each group, 18 patients were excluded from EPLBD group and 16 patients from ES group, and the remaining 61 and 63 patients in EPLBD and ES group, respectively, were included in the study (Fig. 1).
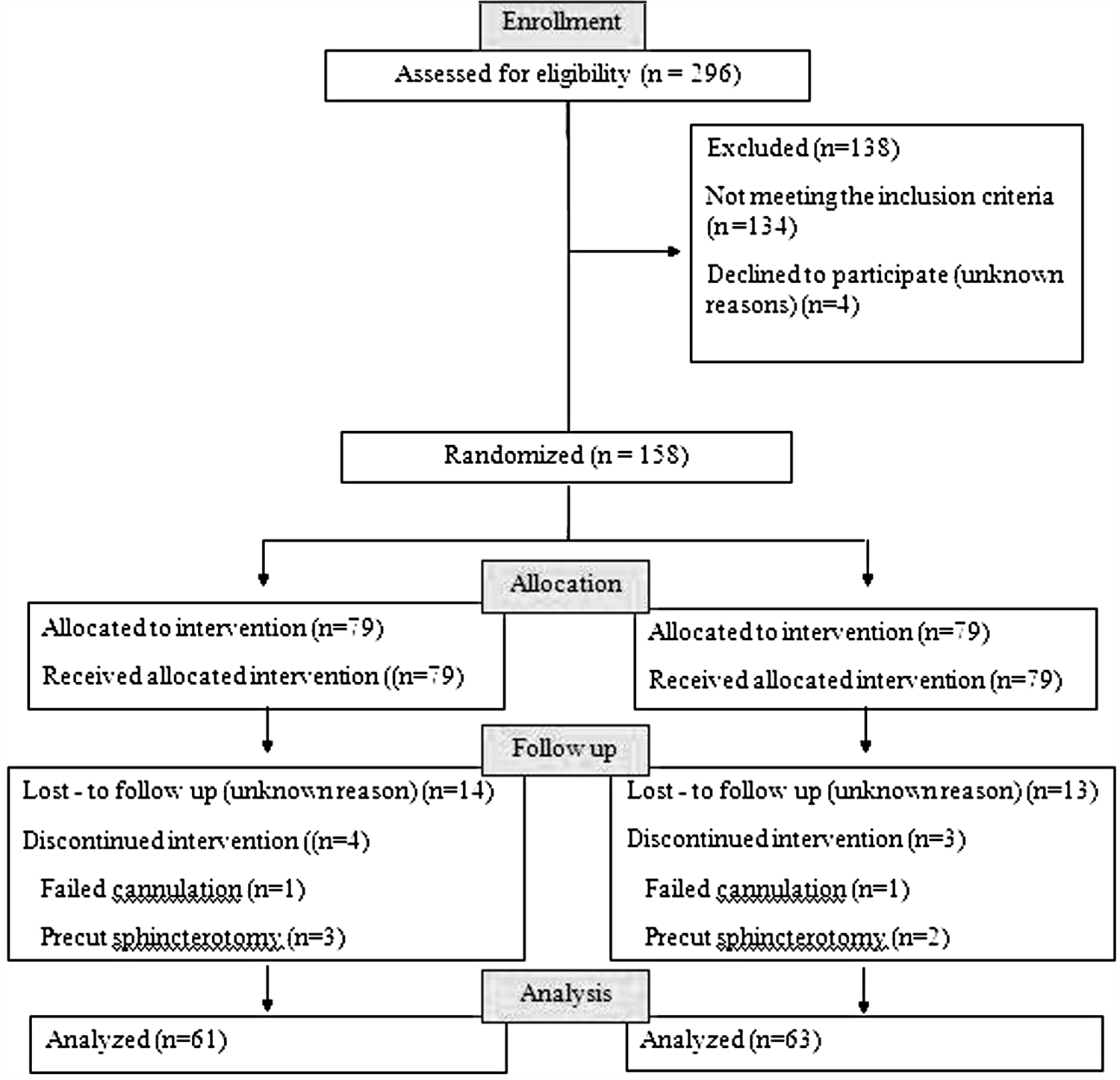
Follow-up chart of patient.
The medical ethical committee of our hospital approved the study protocol and all patients provided written informed consent before entering the study. All patients were subjected to complete assessment, including proper history, clinical examination, laboratory investigations (complete blood count, liver and renal function tests, blood sugar, and serum amylase), and imaging studies (ultrasonography and/or CT, MRCP). All ERCP procedures were performed by experienced endoscopists using the standard duodenoscope (ED-3440T and ED-3485T; Pentax) in the standard manner.
In the first group with EPLBD, after selective cannulation of the CBD with a 5.5 Fr ERCP catheter (Glo-Tip II ERCP catheter; Wilson-Cook Medical, Winston-Salem, NC; COOK Ireland), cholangiography was performed to confirm the diagnosis of CBD stone. After passage of a 0.035 inch guide-wire (Tracer metro direct wire guide; Wilson-Cook Medical, Winston-Salem, NC; COOK Ireland) through the diagnostic catheter, a hydrostatic balloon for esophageal/pyloric dilation (Hercules 3 stage balloon; inflated balloon diameter 12, 13.5, 15 mm/balloon length 8 cm; Wilson-Cook Medical, Winston-Salem, NC; COOK Ireland) was passed over it and placed accurately, across the duodenal papilla under fluoroscopic and endoscopic guidance. The balloon was then inflated gradually with diluted contrast media by using an inflation device (Quantum biliary inflation device; Wilson-Cook Medical, Winston-Salem, NC; COOK Ireland), and maintained for 30–60 seconds. After the waist on the balloon disappeared, the balloon was deflated and removed. If longitudinally extensive narrowing of the balloon was recognized, the pressure of inflation was not increased further to prevent perforation. The size of balloon dilation was determined according to the size of stones and the CBD diameter, not exceeding the diameter of the distal CBD to minimize the risk of perforation.
In the second group with ES, sphincterotomy was done with D.A.S.H. sphincterotome (D.A.S.H. Dometip double lumen sphincterotome; Wilson-Cook Medical, Winston-Salem, NC; COOK Ireland) as large as possible.
The stones were extracted with an extraction basket (Web extraction basket; Wilson-Cook Medical, Inc., Winston-Salem, NC; COOK Ireland) and/or a retrieval balloon (Howell D.A.S.H. extraction balloon; Wilson-Cook Medical, Inc., Winston-Salem, NC; COOK Ireland) with or without the aid of EML (Sohendra lithotripter; Wilson-Cook Medical, Inc., Winston-Salem, NC; COOK Ireland). Endoscopic retrograde biliary drainage (ERBD) was done at the end of the procedure with incomplete stone removal to prevent cholangitis. A second attempt at stone extraction was performed within 3 days if there was incomplete removal of stones in the first endoscopic session.
The primary endpoint was the successful stone removal rate and the secondary endpoints were the mechanical lithotripsy requirement, morbidity and mortality, ERBD requirement, and the number of ERCP sessions required for complete ductal clearance. After ERCP, all patients were observed for at least 24 hours for detection of early complications. Four hours post-ERCP, serum amylase measurement was done in all cases. Routine abdominal ultrasonography and sometime abdominal CT were done for all patients with suspicious post-ERCP pancreatitis. If complications arose, patients stayed in the hospital until they recovered.
The bile duct and stone diameters were measured by comparing the largest diameter of the stone/bile duct with the diameter of the duodenoscope. The number of ERCP sessions was defined as the total number to achieve complete stone clearance. Procedure time was measured between the time when the endoscope was advanced in the mouth and the time when the endoscope was advanced out from the mouth. Post-ERCP complications were defined according to the 1991 consensus guidelines. 1
The continuous variables are expressed as means ± standard deviations or as medians with ranges. Statistical analysis was performed using the chi-square test for noncontinuous variables and Student's t-test for continuous variables. The analyses were performed using SPSS 12.0 (SPSS, Inc., Chicago, IL). P < .05 was considered statistically significant.
Results
Of the total 124 patients with large bile duct stones, 61 patients were enrolled in the EPLBD group and 63 patients were enrolled in the ES group. The patients' demographic characteristics are not significantly different between both groups (Table 1). The results of EPLBD are shown in Table 2. The mean diameter and duration of balloon dilation were 13.5 mm and 43.5 seconds, respectively.
CBD, common bile duct; EPLBD, endoscopic papillary large balloon dilation; ES, endoscopic sphincterotomy.
The outcomes of endoscopic stone removal after EPLBD and ES are shown in Table 3. The overall stone clearance was similar between both groups (96.7% versus 93.7%; P = .53), while the successful complete clearance in the first endoscopic session was significantly higher in the EPLBD group (86.9%) than in the ES group (71.4%), (P = .01). The requirement of EML was significantly less in the EPLBD (9.8%) than in the ES group (17.5%) (P = .04). Mean duration of the whole procedure was similar between the EPLBD group (43.9 ± 10.6 min) and the ES group (47.2 ± 13.6 min) (P = .78). If incomplete stone clearance was suspected at the final cholangiogram, a 10-Fr plastic stent was placed. The need for biliary stent was 9.8% versus 22.2%, respectively (P = .03). Among those patients not successful (6/124), the failure was due to stone impaction (4 patients), basket impaction (1 patient), and intolerance of patient (1 patient).
EPLBD, endoscopic papillary large balloon dilation; ERBD, endoscopic retrograde biliary drainage; ERCP, endoscopic retrograde cholangiopancreaticography; ES, endoscopic sphincterotomy.
There were no significant differences in the complications between the EPLBD and ES group; pancreatitis, 4.9% versus 6.3% (P = .38); hemorrhage, 1.6% versus 6.3% (P = .15); acute cholangitis, 3.3% versus 1.9% (P = .69); basket impaction 1.6% versus 0% (P = .16); and recurrent CBD stone 3.3% versus 3.2% (P = .99) (Table 4). There was no perforation or mortality in either group. All cases of post-ERCP pancreatitis in the EPLBD and ES groups were mild, which improved with medical treatment. Hemorrhage was mild and controlled with injection or spraying of diluted epinephrine solution or balloon compression.
CBD, common bile duct; EPLBD, endoscopic papillary large balloon dilation; ES, endoscopic sphincterotomy.
Discussion
Ampullary widening is the most decisive part for a successful endoscopic removal of CBD stones. 11 ES is the most commonly used method since the first description in 1974. 17 However, ES carries substantial procedure-related risks, such as hemorrhage and perforation, and perhaps an increased incidence of ascending cholangitis and de novo formation of bile-duct stones, especially in younger patients. 18 As an alternative to ES, EPBD was introduced in 1982 by Staritz et al. 4 EPBD has been reported to be safe and effective for the management of CBD stone and advantageously preserves the sphincter of Oddi function and reduce complications, such as hemorrhage and perforation, compared with ES. 6 However, the results of studies of the usefulness of EPBD are conflicting up to date. EPBD is not generally recommended for the treatment of choledocholithiasis because the procedure has been associated with a high risk of pancreatitis to the extent of an increased mortality rate which was reported in a preliminary report of a randomized controlled trial. 19 In contrast, other studies reported no differences in the risk of pancreatitis between ES and EPBD, thus leaving some possibility to offer EPBD for the treatment of bile duct stone. 20 Another limitation of EPBD was related to the size of the balloon. It is difficult to extract large or multiple stones from the bile duct by 8–10 mm balloon dilator that is generally used in EPBD, and often requires mechanical lithotripsy and more endoscopic sessions to achieve bile duct clearance. 15
EPLBD combined with limited ES was first reported in 2003 by Ersoz et al. 10 In the previous technique, a large diameter balloon catheter, which usually had been used for dilating esophageal or pyloric strictures, had been used for dilating the papillae for patients with intractable bile duct stones. Since that time, several studies have been demonstrating the therapeutic outcomes and safety of this technique for larger stone extraction.21–24 The risk of pancreatitis is presumably protected because the obstruction of the pancreatic orifice is alleviated by antecedent ES. However, concerns over hemorrhage and loss of sphincter functions still remain. 14 Wider opening of the ampullary orifice with loss of ampullary sphincter function is likely to increase recurrence of bile duct stones secondary to reflux of duodenal contents into the bile duct. 14 There are no methods to achieve enlargement of ampulla that minimize the risk of early complications and preserve sphincter function. One retrospective study suggested that EPLBD without ES, which showed the possibility to preserve sphincter function, was safe and effective in patients with large bile duct stone. 25
In our study, the comparison of the result between both groups in the overall rate of complete stone clearance showed that the two procedures were similar (96.7% versus 93.7%; P = .53). Our result was consistent with many recent previous studies.11,14,26,27 However, it has been reported that EPLBD may reveal better results in the removal of large-sized stone. 10 The initial success rate for the removal of CBD stone was significantly higher in the EPLBD group (86.9%) than in the ES group (71.4%) (P = .01), and these data were similar to previously published results.25,28,29 In contrast, many studies revealed that EPLBD did not show any advantages over ES in the successful clearance of bile duct stones in one session.14,26,27 In patients whose CBD stones could not be completely removed in the first ERCP session, the cause was mainly impacted stone. The mean number of required endoscopic sessions for complete stone clearance was less frequent in the EPLBD group (1.03 ± 0.36) than in the ES group (1.13 ± 0.45), but the difference was not statistically significant (P = .66).
The use of EML was frequently lower in EPLBD group (9.8%) than in the ES group (17.5%) (P = .04), and this result was similar to previously published result.21,26,30,31 Therefore, it was thought that large balloon dilation can dilate the orifice of the papilla more than conventional ES and offer a more adequate orifice for removal of large stones. 11 However some studies did not show any significant difference in EML between both groups.11,14,32 The requirement for EML might depend on stone size, the extent of ES, the shape of stones, and the bile duct. 21 Therefore, EML could still be applied when large balloon dilation by itself could not stretch the distal bile duct wall enough to be effective for removal of large stones. 27
In our study, ERCP duration tended to be shorter in the EPLBD group compared with ES group, however, the result revealed no significant difference. In contrast, two recent meta-analyses revealed that EPLBD was performed with longer durations; however, the meta-analyses revealed no significant difference in ERCP duration.11,26 ES required more ERBD compared with EPLBD (9.8% versus 22.2%) (P = .03), which would probably add up to extra therapeutic cost. In contrast, Oh and Kim 14 reported similar rate of ERBD between EPLBD and ES.
Regarding complications, our study suggested that EPLBD did not increase the frequency of overall early complications or any single one. This was consistent with many recent studies.11,14,26 In contrast, it was reported that EPLBD may cause very serious bleeding 33 and perforation. 34 In our study, the risk of bleeding associated with EPLBD was negligible. Only minor bleeding developed in 1.6% of patients in the EPLBD group and was controlled easily with a diluted epinephrine solution injection or spray or balloon compression. EPLBD might have advantages in patients with coagulopathy over ES. Also, retroperitoneal perforation was negligible in this study as no patients developed perforation in both groups. The size of the balloon is the major determinant for the success of EPLBD. As the ampullary enlargement by balloon dilation becomes wider, stone removal can be facilitated. However, oversized balloons increase the risk of perforation or vessel injury. 14 In the present study, we used balloons between 12 and 15 mm in diameter, not exceeding the size of the CBD stone and the diameter of the distal part of the CBD. This large ballooning was safely performed because the CBD was already dilated over the size of the balloon. It is very important to avoid excessive inflation, especially in case of bile duct strictures, to prevent the risk of perforation or bleeding. The incidence of cholangitis in EPLBD group was slightly higher but not statistically significant compared with ES group (3.3% versus 1.9%; P = .69). This may be explained by the associated risk of ampullary edema which may be increased by EPLBD.
Oh and Kim, 14 hypothesized that EPLBD may preserve sphincter function and decrease subsequent risk of CBD stone recurrence by reducing ascending infection of bile. However, duodeno-biliary reflux associated with a large sphincterotomy is not the only cause. Stone recurrence is more likely to be caused by several factors working together, including the contamination of bile by enteric bacteria, but also a reduced biliary outflow through a small sphincterotomy or a stricture of the sphincterotomy site, and a dilated CBD with a consequent bile stasis and sludge creation. The incidence of recurrent CBD stones was similar in both groups (3.3% versus 3.2%; P = .99). Although some previous studies reported that papillary function seemed to recover much faster and CBD stone recurrence was decreased after EPLBD, sphincter function might be slowly and partially recovered after EPLBD because extensive dilation of the sphincter may lead to the tearing of the sphincteric muscles.35,36 Assessment of sphincter function and long-term follow-up after EPLBD should be necessary. One of the limitations of our study was the small sample size. A large-scale, multicenter study will be needed to confirm the therapeutic outcomes of EPLBD.
In conclusion, EPLBD is an effective and safe method for the removal of large CBD stones with similar success rate and complication rate compared with standard ES. EPLBD should be considered as an alternative to ES for patients in whom ES could not be routinely performed. EPLBD is also recommended for removal of large CBD stones in patients with an underlying coagulopathy or need for anticoagulation after ERCP.
Footnotes
Disclosure Statement
No competing financial interests exist.