
Abstract
Abstract
Background:
The aim of this study was to explore the significance of upper mediastinal lymph node dissection performed by video-assisted thoracic surgery in the treatment of middle thoracic esophageal carcinoma.
Materials and Methods:
The clinical and pathological data from 128 patients with middle thoracic esophageal carcinoma who underwent surgery from January 2013 to December 2015 using a right chest-abdomen-neck approach combined with thoracoscopy and laparoscopy in the Jieyang People's Hospital of Huangdong province were analyzed retrospectively.
Results:
The lymph node metastasis rates of the thoracic left para-recurrent laryngeal nerve (1, 2, and 4L zones) and right para-recurrent laryngeal nerve (1R zone) were 30.47% and 28.12% in 128 cases, respectively. The metastasis rates of the 2R, 4R, and 5 zones were 4.69%, 3.91%, and 5.47%, respectively.
Conclusions:
The upper mediastinal region was the most common location for lymph node metastasis from middle thoracic esophageal carcinoma, and upper mediastinal lymph node dissection performed by video-assisted thoracic surgery was safe and complete. It also reduced the risk of para-recurrent laryngeal nerve injury, residual tumor, and the postoperative recurrence rate.
Introduction
L
It is unclear if minimally invasive esophagectomy is an oncologically safe technique. 5 How to perform local esophagectomy and complete excision of regional lymph nodes with VATS are currently important research topics. Moreover, esophagectomy with VATS requires a high degree of proficiency.6,7 Whether VATS can successfully achieve complete dissection and resection, while avoiding injury to the surrounding organs and tissues, especially for the left and right para-recurrent laryngeal nerve lymph nodes, is still not resolved.
The field range of the entire operative team is better than the common direct vision. With improvements in the application of thoracoscopes with high definition and improved operative technique, an ultrasound knife can be used to separate tissues and reduce bleeding during the surgery, making operative vision more distinct and improving surgical safety, and this may even increase the success rate of radical surgery. VATS improves the safety and success of surgery, and therefore, thoracoscopic esophagectomy can be performed with minimal invasiveness, while systemically dissecting all of the lymph nodes.8,9 This study aimed to explore the safety and standardization of upper mediastinal lymph node dissection with VATS for the treatment of middle thoracic esophageal squamous carcinoma.
Materials and Methods
General data
From January 2013 to December 2015, the records of 128 patients who underwent thoracic middle esophagectomy through a right chest-abdomen-neck approach combined with thoracoscopy and laparoscopy in the Jieyang People's Hospital of Huangdong province were retrospectively reviewed. The included patients had not received neoadjuvant radiochemical therapy and were not diagnosed with distant metastasis before the surgery. There were 106 men and 22 women, and the preoperative clinical features of the patients are shown in Table 1.
Postoperative pathological classification was made using standard tumor-node-metastasis (TNM) classification (UICC7 version), and there were 12, 27, and 89 cases that were postoperative surgical-pathologic TNM (p-TNM) stage I, II, and III, respectively. The pathological degree of differentiation included 8 cases of G1, 25 cases of G2, and 95 cases of G3. All patients underwent esophagectomy and systematic lymph node dissection, including 896 lymph nodes from the upper mediastinum, with an average of 5.54 ± 2.92 lymph nodes per patient. In 63 cases, 249 lymph node metastases were found, with an average of 3.65 ± 1.82 lymph nodes per patient, and the upper mediastinal lymph node metastatic rate and ratio of metastatic nodes were 49.22% and 27.79%, respectively. This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of People's Hospital of Jieyang. Written informed consent was obtained from all participants.
Division of lymph node area
Mediastinal lymph nodes were zoned according to their anatomical sites, and the upper mediastinum contains 1–6 zones of lymph nodes, while the lower mediastinum contains 7–10 zones of lymph nodes.
Surgical method
Double-lumen intubation combined with epidural anesthesia was used in this study. Left lung ventilation was performed during the process of thoracoscopy and it was then replaced by double-lung ventilation during laparoscopy and the neck operation. The surgical operation had three steps:
(1) The thoracoscopy required patients to be in the left lateral position at 90° and a 12-mm incision was made in the ninth intercostal space of the right scapular line tenth interspace to place the thoracoscope, followed by a 12-mm incision and 5-mm incision from the seventh intercostal space of the middle axillary line and scapular line to place the ultrasound knife and grasping forceps, respectively, to separate the esophagus. Next, a 10-mm incision of the fourth intercostal space of the anterior axillary line was placed for the penta-prongs retractor to move the lung and esophageal tissues. We incised the pleura mediastinalis along with the esophagus to detect and separate the tissues so as to confirm whether or not the esophageal carcinoma showed obvious invasion; subsequently, thoracic esophagectomy plus para-esophagus and mediastinal lymph nodes dissection were conducted. The esophagus was separated up to the neck and down to the esophageal hiatus. Figure 1 showed the intraoperative cleaning of Upper Mediastinal lymph nodes. (2) The laparoscopic operation required the patient be in a horizontal position. The angle between the head and feet was maintained at 30° after completion of neck and abdominal disinfection. A 1-mm incision under the navel was made to place the pneumascos needle to establish the artificial pneumoperitoneum, and then, the 12 mm diameter trocar and laparoscope were placed, followed by placing four different trocars (5, 5, 5 mm, and 12 cm) in the incisions in the midclavicular line and anterior axillary line of the left and right costal lower border, respectively, under the direct vision of the microscope. The surgeon stood to the left of the patient to observe the adhesive and metastatic conditions. We dissociated the greater curvature of the stomach along with the outside of the great gastric curvature vessels and ligated the left gastric vein and artery, and the ultrasound knife was used to remove the lymph nodes from the left gastric vein and artery, common hepatic artery, left spleen artery, and stomachus cardiacus, and then continued to dissect lymph nodes upper to the esophageal hiatus and down to the thoracic esophagus. (3) To perform the esophagogastrostomy, a 5-cm incision was made in the anterior border of the left sternocleidomastoid; then, we dissociated the cervical esophagus along with the inside of the neck vascular sheathing. A 5-cm incision was made under the xiphoid to pull out the stomach to make a gastric tube and inosculate the fundus of the stomach and cervical esophagus with a circular stapler.
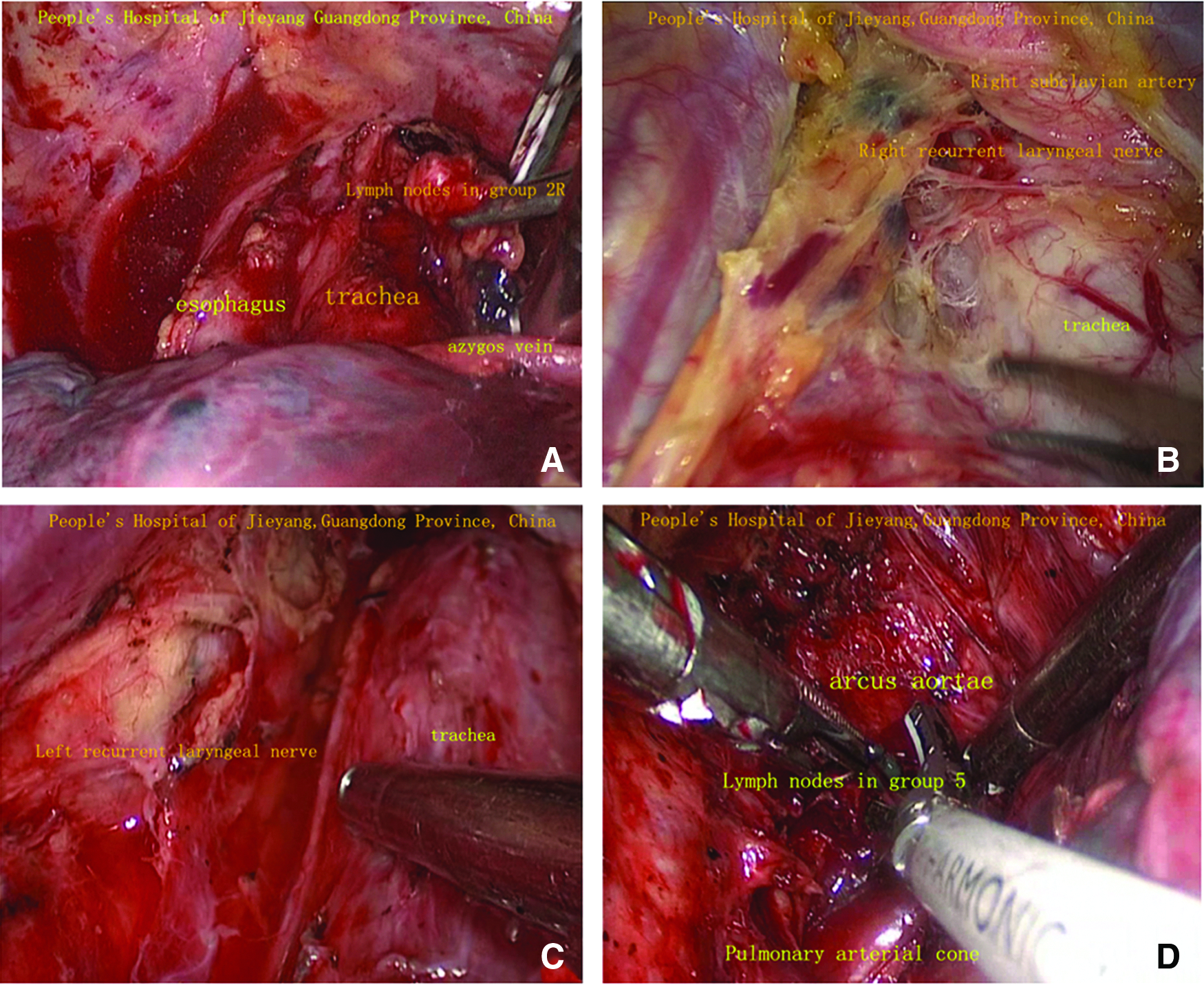
Intraoperative photographs depicting the anatomy and thoracoscopic dissection of the upper mediastinum.
Results
Clinical data
A total of 3074 lymph nodes were dissected in this study, and 791 metastatic lymph nodes were found. From the upper mediastinum, 896 lymph nodes were obtained and 63 cases had 249 metastatic lymph nodes; the upper mediastinal lymph node metastatic rate and ratio of metastatic nodes were 49.22% and 27.79%, respectively. In addition, 974 lymph nodes were from the lower mediastinum, including 288 metastatic lymph nodes from 61 cases, and the lower mediastinal lymph node metastatic rate and ratio of metastatic nodes were 47.66% and 29.57%, respectively. Furthermore, 1204 celiac lymph nodes were removed, including 254 metastatic lymph nodes from 59 cases, and the celiac lymph node metastatic rate and ratio of metastatic nodes were 46.09% and 21.10%, respectively.
Upper mediastinal lymph nodes metastasis
The lymph node metastasis rates in Group 5 zone, Group 2R zone, and Group 4R zone were 5.47%, 4.69%, and 3.91%, respectively. The metastasis rates in the thoracic left recurrent laryngeal nerve lymph node (1, 2, and 4L zones) and right para-recurrent laryngeal nerve lymph node (1R zone) were 30.47% and 28.12%, respectively, and the lymph node metastasis rates of the thoracic right para-recurrent laryngeal nerve origin (1R zone) and thoracic left recurrent laryngeal nerve origin (4L zone) were 28.12% and 15.63%, respectively. Table 2 shows the upper mediastinal lymph node metastases in different groups.
Discussion
The presence of upper mediastinal lymph node metastasis predicts a poor outcome in patients with esophageal carcinoma. In the lymph nodes of the upper mediastinal area, the left and right para-recurrent laryngeal nerve lymph nodes are the most common metastatic location from thoracic esophageal squamous carcinoma and are in a key position for metastatic spread from the mediastinum to the neck, which highlights the importance of lymph node dissection of this region in the surgical treatment of middle thoracic esophageal squamous carcinoma. Fujita et al. 10 reported that the metastatic rate of right para-recurrent laryngeal nerve lymph nodes was the highest. Malassagne et al. 11 reported that the 5-year survival rate of patients with positive thoracic para-recurrent nerve nodal involvement was 21%, which was much lower than that in the nonmetastatic group (47%), and suggested that thoracic para-recurrent nerve nodal involvement was strongly associated with the prognosis of esophageal carcinoma.
In this study, the number of upper mediastinal lymph nodes removed by VATS was more than that with open surgery, especially for lymph nodes with a diameter less than 2 mm. The left and right para-recurrent laryngeal nerves were exposed clearly and could be protected, while all of the surrounding lymph nodes were removed, with a low hoarseness rate after the surgery.
Li et al. 12 indicated that paratracheal nodes were the most frequently metastasized nodes (17.5%) and the frequency of lymph node metastasis was 18.8% in the middle mediastinum. In this study, the frequency of lymph node metastasis was 4.69%, 3.91%, and 5.47% in the 2R, 4R, and 5 zones, respectively, and there were no obvious differences among the 3 zones.
Thoracic upper esophageal squamous carcinoma at the early stage spreads to the right para-recurrent laryngeal nerve lymph nodes, and it may be involved in the metastasis of thoracic middle esophageal carcinoma owing to the extended distance of the dense submucous drainage vessels. 13
Lymph node metastasis of esophageal squamous carcinoma is the main factor affecting prognosis. 14 Routine esophagectomy usually has a poor prognosis, and upper mediastinum involvement is the main cause of local recurrence after surgery. The diagnostic accuracy of lymph node metastasis depends on the metabolic activity of the thoracic primary lesion of esophageal carcinoma. 15
Whether lymph node dissection is complete or not distinctly affects postoperative survival. The upper mediastinal area is the most common site of lymph node metastasis of thoracic middle esophageal squamous carcinoma, including the thoracic left para-recurrent laryngeal nerve (1, 2, and 4L zones) lymph nodes, thoracic right para-recurrent laryngeal nerve (1R zone) lymph nodes, and 2R zone, 4R zone, and 5 zone lymph nodes. Moreover, left para-recurrent laryngeal nerve lymph node metastasis is the most common metastasis site in the upper mediastinal lymph nodes.
Upper mediastinal lymph node dissection with VATS, especially for the complete removal of the left and right para-recurrent laryngeal nerve lymph nodes, can reduce the residual tumor and postoperative recurrence rate. The left and right para-recurrent laryngeal nerves can be clearly exposed and protected during the dissection, which improves the quality of life. Our results support the standardization of a minimally invasive treatment approach to esophageal carcinoma.
Footnotes
Disclosure Statement
No competing financial interest exists.