
Abstract
Abstract
Aim:
This study aimed to report the results of a multicentric survey about laparoscopic treatment of pancreatic tumors in children.
Materials and Methods:
The data of patients operated using minimally invasive surgery (MIS) for a pancreatic tumor in 5 International centers of Pediatric Surgery in the last 5 years were retrospectively reviewed. We recorded data relating to the clinical presentation, diagnostic evaluation, surgical technique, and outcome.
Results:
Fifteen patients (average age 2.2 years) were identified. The most common symptoms at presentation were related to the hypoglycemic hyperinsulinism, followed by abdominal pain and vomiting. Tumor types were insulinoma (n = 4), congenital hyperinsulinism of infancy (CHI) diffuse type (n = 3), CHI focal type (n = 3), solid pseudopapillary tumor (n = 2), and cystic malformation (n = 3). The diagnostic assessment was completed using ultrasound associated with computed tomography (CT) scan in all centers; 18FDOPA positron emission tomography in combination with CT was adopted in 2 centers. The MIS procedures performed were as follows: tumor enucleation (n = 4), distal pancreatectomy (n = 8), subtotal pancreatectomy (n = 2), and pancreatico-jejunostomy (n = 1). Average operative time was 110 minutes. As for postoperative complications, we recorded 1 persistent hypoglycemia, requiring redo-surgery (IIIb Clavien-Dindo) and 1 thrombosis of splenic vein, not requiring any treatment (I Clavien-Dindo).
Conclusions:
Laparoscopic resection can be considered a safe and effective treatment with minimal morbidity and excellent outcomes for most pediatric pancreatic tumors. Suspension of the stomach with a transparietal stitch and use of new hemostatic devices as Starion TLS3 or Ligasure are key factors for the success of the procedure. A long-term follow-up is mandatory in these patients to evaluate postoperative complications and long-term outcome.
Introduction
P
According to U.K. registry, the most common pancreatic tumor is pancreatoblastoma, followed by solid pseudopapillary tumors and islet cell tumors. 2 Rickham in 1975 reported on the rarity of islet cell tumors in childhood. He described 3 patients: 1 neonate and 2 older children. 3
Insulinomas are insulin-secreting tumors that arise from pancreatic beta cells. They are the most common functioning neoplasm of the pancreas with an estimated incidence of 4 per million people. 4 Although most insulinomas are solitary and sporadic, 10% occur in the setting of multiple endocrine neoplasia-type 1 in which multiple tumors may be present. 5 Patients with insulinomas often have delayed diagnosis after months of nonspecific episodic symptoms related to underlying hypoglycemia. Once diagnosed, insulinomas are poorly managed medically, and surgical resection provides the only possibility for cure.6,7
Congenital hyperinsulinism of infancy (CHI) is another entity characterized by inappropriate over-secretion of insulin resulting in persistent hypoglycemia and can cause severe neurologic sequelae if it is not managed appropriately in timely fashion. Management consists of initial medical treatment that includes antisecretory medications (diazoxide) or in case of failure of this treatment long-acting somatostatin analog (octreotide). 8 Failure of medical treatment is an indication for surgical intervention. 9 Generally, an open near-total pancreatectomy is performed to control hypoglycemia.10,11
However, the recent advancements in minimally invasive surgery (MIS) techniques have enabled surgeons to perform laparoscopic pancreatectomy safely. Most of these reports are among adult population with mostly distal pancreatectomies.12,13
Very few reports in the literature have described the role of laparoscopic approach for treatment of these pathologies in children.14–17
The aim of this study was to report the results of a multicentric survey about laparoscopic treatment of pancreatic tumors in children.
Patients and Methods
A specific form based on patients characteristics, technical details and outcome of laparoscopic resection of pancreatic tumors performed in the last 5 years was mailed to 8 pediatric surgical centers.
Five out of the 8 pediatric centers completed the form and were enrolled in this study.
We retrieved data relating to the clinical presentation, diagnostic evaluation, details of surgical technique, and outcome.
Statistical analysis was carried out by using the Statistical Package for Social Sciences (SPSS, Inc., Chicago, IL), version 13.0. Significance was defined as P < .05.
This study received the appropriate Institutional Review Board approval.
The laparoscopic technique
All the patients were operated under general anesthesia with orotracheal intubation and they received a nasogastric tube and a bladder catheter before surgery.
The child was placed supine on the operative table with the legs in frog-like position at the lower end of the table, which was tilted in reverse Trendelenburg position.
The surgeon stayed at the lower end of the table with the cameraman to his left and the scrub nurse to his right. The first trocar was inserted in an open way through the umbilicus for a 10-mm 30° optic. The carbon dioxide pneumoperitoneum pressure was at 8 mmHg and flow at 2 L/min. Other two 5-mm trocars for working instruments were placed pararectally at umbilical level. We used 5-mm trocars to have the possibility to use clip appliers or new hemostatic devices.
The greater curvature of the stomach was suspended with two transabdominal stay sutures, then the gastrocolic ligament was opened transversally, thus exposing the pancreas. If a lesion was not seen, the lower border of the pancreas was easily mobilized. Care was taken not to open the mesentery of the transverse colon. When a focal lesion was present, it was enucleated with the aid of sealing devices (Starion TLS3 or Ligasure).
In other cases, a distal or a sub-total pancreatectomy was performed using sealing devices and avoiding use of clips. The spleen was left in situ and its vessels intact. The specimen was extracted through the umbilicus by using an endo-bag.
Results
The data of 15 patients (8 girls and 7 boys) were reviewed and analyzed. Average age at surgery was 2.2 years (range 1 month–13 years). Average weight at surgery was 7.8 Kgs (range 3.8–35 Kgs).
Tumors with an endocrine component had clinical features mainly related to the hyperinsulinism and comprised hypoglycemia, lethargy, seizures, and drowsiness. Other presenting clinical features were typically nonspecific and comprised abdominal pain, nausea and/or vomiting, anorexia, and abdominal distension.
The diagnostic assessment was completed using ultrasound associated with computed tomography (CT) in all centers; 18FDOPA positron emission tomography (PET) in combination with CT was adopted in 2 centers (Fig. 1).

A 18FDOPA positron emission tomography/computed tomography, performed in a 40-day-old child with insulinoma, showed hyperaccumulation of radiopharmaceutical in the tail of the pancreas.
Tumor types were insulinoma (n = 4), congenital hyperinsulinism (CHI) diffuse type (n = 3), CHI focal type (n = 3), solid pseudopapillary tumor (n = 2), and cystic malformation (n = 3) (Fig. 2).
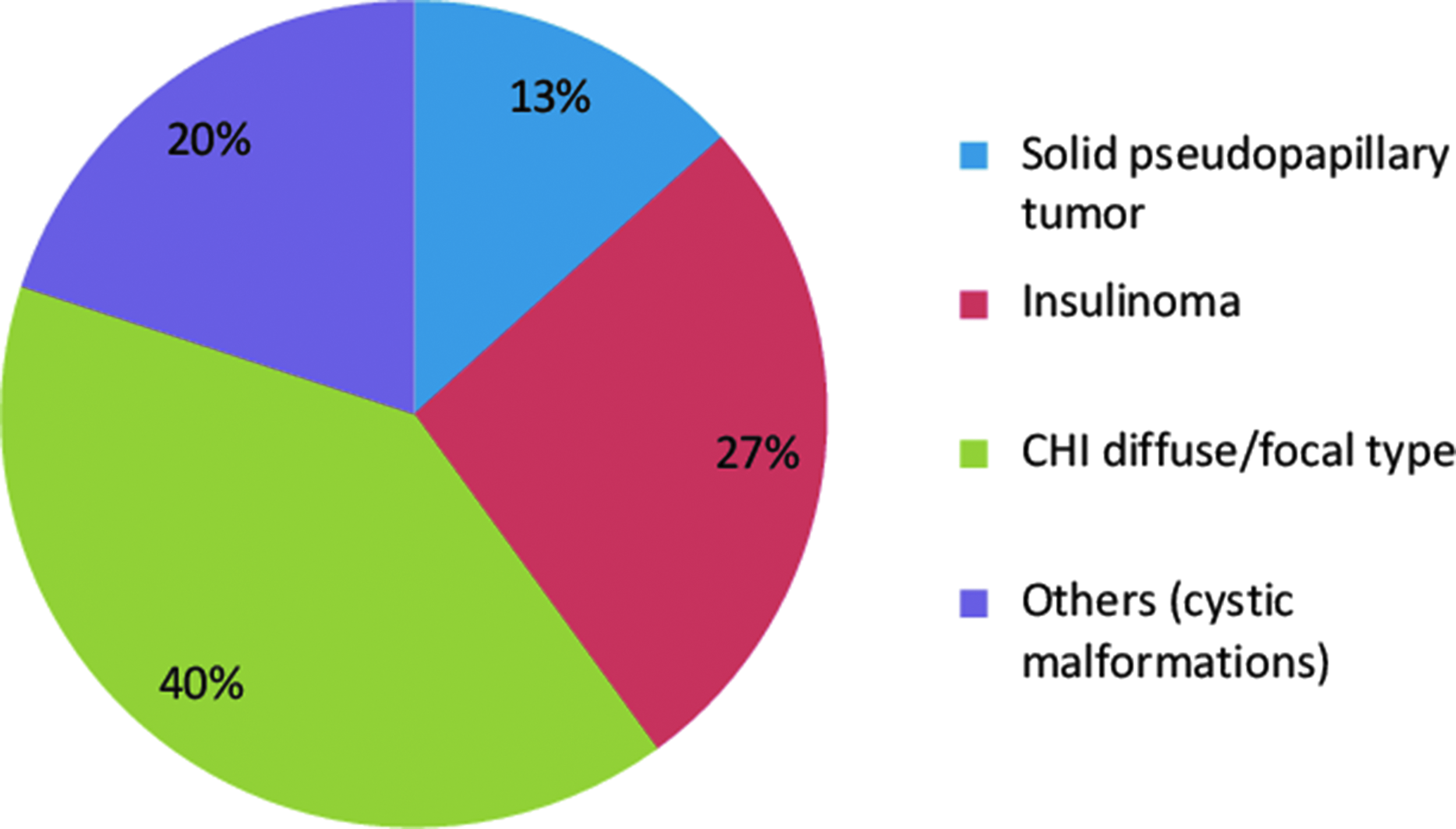
Distribution of pancreatic tumors treated in our series of patients (n = 15). CHI, congenital hyperinsulinism of infancy.
All patients were operated using MIS. The procedures performed were as follows: tumor enucleation (n = 4), distal pancreatectomy (n = 8), subtotal pancreatectomy (n = 2), and wirsungo-jejunostomy (n = 1).
Seven children had an intraoperative (frozen section) biopsy during excision.
Average operative time was 110 minutes (range 60–180 minutes) and all procedures were completed in laparoscopy, without conversions to open surgery or intraoperative complications. In all procedures special hemostatic devices (Starion TLS3 or Ligasure) were adopted for dissection and parenchymal section and no major intraoperative bleeding was reported.
Average hospital stay was 4.5 days (range 2–8 days). Average time to restart full-oral intake was 1.8 days (range 1–3 days). Average analgesic requirements was 1.5 days (range 1–3 days).
Average follow-up was 45 months (range 12–60 months). All patients showed normal levels of blood sugar and insulin at follow-up.
We recorded postoperative complications in 2 patients (13.3%). One child with CHI diffuse type, treated with subtotal pancreatectomy (>85%), presented postoperatively a persistent hypoglycemia and he was reoperated, performing a near total (85%> 99%) pancreatectomy (IIIb Clavien-Dindo). The head of the pancreas and the uncinate process were removed, leaving just a little nubbin of pancreas just below the distal end of the choledochal duct. The spleen was left in situ and the repeat laparoscopic surgery was surprisingly easy, with relief of persistent symptoms.
Another child with CHI focal type, underwent a spleen-preserving distal pancreatectomy, developed postoperatively a thrombosis of splenic vein, not requiring redo-surgery (I Clavien-Dindo). She developed on seventh postoperative day thrombocytosis (platelets count 1,230,000/mm3) and was treated with acetylsalicylic acid, with a normalization of platelets count (492,000/mm3) 90 days postoperatively.
Patients' demographics, presentation, and treatment of pancreatic tumors are reported in Table 1.
CHI, congenital hyperinsulinism of infancy.
Discussion
In the adult population, pancreatic tumors represent almost 3% of all malignancies and are predominantly ductal in origin. 2 In contrast, pancreatic tumors in the pediatric population are much rarer, they have a different histopathological basis and they are generally benign although some lesions may have malignant potential.18,19
All pancreatic tumors reported in our series were benign.
The most common pancreatic lesions in our series were represented by congenital hyperinsulinism of infancy (CHI) in both its forms, diffuse and focal, followed by insulinomas (10/15 patients, 67%).
CHI is a rare congenital disease of glucose metabolism, characterized by inappropriate over-secretion of insulin resulting in persistent hypoglycemia. 8 Insulinomas are insulin-secreting tumors that arise from pancreatic beta cells. Most of these patients presented clinical features related to hyperinsulinism, with hypoglycemia and neurological manifestations such as seizures, lethargy, and drowsiness and their average age at presentation was very low (2.9 months). Only 2 older patients (2 and 4 years, respectively) presented with nonspecific symptoms such as abdominal pain, nausea, and anorexia. Several medical agents are available to control severe hypoglycemia with a variable success rate.9,15 Surgical intervention is advocated when medical therapy fails.8,9 The failure of diazoxide or octreotide treatment to provide adequate relief of hypoglycemia in our patients corroborates other studies, which have shown that medical management of insulinoma has very limited success but may allow for symptomatic control during preoperative evaluation to localize the tumor.7,20 There are no data to correlate the degree of hypoglycemia with neurologic damage, and some reports advocated early surgical intervention to prevent neurologic complications. 21 Among patients managed surgically, diabetes mellitus develops in 12%–56% of them depending on extent of surgery, age at surgery, and length of follow-up.22,23 Some recommendations were made according to the pathologic type (focal, diffuse, or mixed), but data are unclear in that regard.8,9,14 There is evidence that the exocrine function is impaired as well, so extended pancreatectomy should only be performed in diffuse forms that do not respond sufficiently to medical treatment. For focal disease, if localization techniques are successful preoperatively, limited resection is curative.9,14
The differentiation between focal and diffuse forms is not easy. Classic imaging studies using ultrasound, CT are not very helpful either.
Recently, the 18FDOPA PET/CT has been used for the detection of focal lesions.24,25
In our series, 18FDOPA PET/CT was adopted in 2 centers. Seven of the 10 patients of our series presenting endocrine pancreatic tumors had a focal lesion (CHI focal type, insulinoma), which was confirmed at surgery and by histology. In the remaining 3 patients, CHI diffuse disease was confirmed histologically. One of these patients required a redo-surgery for persistent hypoglycemia and underwent a near total (85%> 99%) pancreatectomy with relief of symptoms.
In contrast to previous literature reports,2,17 solid pseudopapillary tumors had a lower incidence in our series (2/15 patients, 13%), they presented with nonspecific symptoms including abdominal pain and vomiting and were diagnosed in older children (4 and 5 years, respectively). Pancreatic and liver enzymes as well as tumor markers were within normal limits. Their treatment was complete laparoscopic excision via either surgical enucleation in case of tumors located in the pancreatic tail and distal pancreatectomy when the lesion was located in the body of the pancreas.
The remaining cases (3/15 patients, 20%) were represented by pancreatic cystic malformations: in 2 patients with nonspecific symptoms including abdominal pain and distension we found a congenital pancreatic cyst, located in the body of the pancreas, treated by laparoscopic distal pancreatectomy and with resolution of symptoms. In one child, presenting with acute epigastric pain, vomiting, and weight loss, it was found a cystic dilatation of the pancreatic duct with calcifications in the pancreatic head, related to a chronic pancreatitis. Two endoscopic retrograde cholangio-pancreatographies failed to drain the pancreatic duct and a wirsungo-jejunostomy was successfully performed under laparoscopy with drainage of the pancreatic duct and relief of the symptoms.
Use of minimally invasive techniques in pancreatic surgery is fairly new.16,17,22 Most of the reports are among adult population and limited to benign lesions.12,13 Few case reports have shown the feasibility of laparoscopic pancreatic surgery in children and exceptionally MIS was performed in patients under 10 kgs.8,9,26
For lesions located in the pancreatic tail, laparoscopic distal pancreatectomy with preservation of the spleen appears to be the preferred surgical approach over open surgery. For lesions elsewhere, enucleation together with a distal pancreatectomy could be offered.9,27 The spleen, however, should be preserved 9,28
For benign or low-grade malignant lesions located in the head of the pancreas, duodenum-preserving pancreatic head resection has been shown to have favorable outcomes in adults in terms of postoperative complications, pancreatic function, and recurrence. 29 This duodenum-preserving approach has also been reported in children with pancreatic head lesions. 30
We used a pancreas sparing approach in the management of our patients and thus attempted enucleation in all cases in which injury to the main pancreatic duct did not seem likely.
Enucleation was accomplished in 4 of 15 cases for lesions preferentially located in the pancreatic tail, a distal pancreatectomy was performed in 8 of 15 cases for lesions in the tail and body, while a subtotal pancreatectomy (>80%) was preferred in 2 of 15 cases with multifocal involvement of the pancreas (CHI diffuse type). This is consistent with the literature reports in which enucleation was performed in 34%–54% of cases6,12 and was the procedure of choice in the absence of possible injury to the main pancreatic duct or when malignancy was not suspected. A wirsungo-jejunostomy was performed only in one case with involvement of the pancreatic duct.
We think that MIS is the procedure of choice to perform pancreatic resection in expert hands. Laparoscopic excision of pancreatic tumors can provide a definitive cure with minimal morbidity and excellent outcomes. Crucial to efficient management of a child with a pancreatic lesion is the accurate preoperative and intraoperative localization of the tumor.
Thanks to the miniaturization of laparoscopic instruments, technical expedients such as the suspension of the stomach with transparietal stitches and the use of the currently available sealing devices such as Starion TLS3 and Ligasure, it is possible to resect the pancreas easily and rapidly without clips positioning. After the resection, the pancreatic specimen is extracted through the umbilicus into an endobag to avoid pancreatic fragmentation and eventually tumoral spreading.
In addition, laparoscopy has revealed relatively easy even when used for repetitive surgery.
A long-term follow-up is mandatory in these patients to evaluate postoperative complications and long-term outcome. In our mind, considering the rarity of the pathology and the scanty experience of pediatric surgeons, these patients should be referred only in experienced centers with high-volume MIS activity.
Footnotes
Disclosure Statement
No competing financial interests exist.