
Abstract
Abstract
Background:
Video-assisted thoracic surgical (VATS) lobectomy is gaining popularity in the treatment of lung cancer. The aim of this study is to investigate the learning curve of VATS lobectomy by using multidimensional methods and to compare the learning curve groups with respect to perioperative clinical outcomes.
Methods:
We retrospectively reviewed a prospective database to identify 67 consecutive patients who underwent VATS lobectomy for lung cancer by a single surgeon. The learning curve was analyzed by using moving average and the cumulative sum (CUSUM) method. With the moving average and CUSUM analyses for the operation time, patients were stratified into two groups, with chronological order defining early and late experiences. Perioperative clinical outcomes were compared between the two learning curve groups.
Results:
According to the moving average method, the peak point for operation time occurred at the 26th case. The CUSUM method also showed the operation time peak point at the 26th case. When results were compared between early- and late-experience periods, the operation time, duration of chest drainage, and postoperative hospital stay were significantly longer in the early-experience group (cases 1 to 26). The intraoperative estimated blood loss was significantly less in the late-experience group (cases 27 to 67). CUSUM charts showed a decreasing duration of chest drainage after the 36th case and shortening postoperative hospital stay after the 37th case.
Conclusions:
Multidimensional statistical analyses suggested that the learning curve for VATS lobectomy for lung cancer required ∼26 cases. Favorable intraoperative and postoperative care parameters for VATS lobectomy were observed in the late-experience group.
Introduction
V
Cumulative sum (CUSUM) analysis is a graphic method that is widely used for date analysis in the medical field, including the learning curves of surgical procedures. Because CUSUM enables to show data deviation from the mean value, it is useful to detect data trends, which cannot be discernable with other approaches. 8 The moving average is a method that is used to analyze data points by creating a series of averages of different subsets of the full dataset. 9 As it would be difficult to represent an overall flow of data by plotting each data point, this method was used to apprehend the overall trend of data by detection of cumulative changes from average values. Recently, the CUSUM analysis has been applied to evaluation of the learning curve of minimally invasive surgical procedures in the field of rectal cancer, esophageal cancer, and sigmoid colon cancer.9–11 To the best of our knowledge, there has been no publication addressing the learning curve of VATS lobectomy for lung cancer using both the moving average method and the CUSUM method. Therefore, this study was designed to assess the learning VATS lobectomy for lung cancer by a single surgeon using multidimensional statistical methods: moving average method and CUSUM method.
Patients and Methods
We retrospectively reviewed a prospectively collected lung cancer database to retrieve 67 consecutive patients with non-small cell lung cancer (NSCLC) undergoing lobectomy who underwent VATS by a single surgeon (J.W.) at our institution from 2013, when VATS lobectomy was first adopted, to 2015. Before implementing the VATS technique, the surgeon had performed >100 open surgeries for lung cancer. The Institutional Review Board of the Affiliated Jiangning Hospital of Nanjing Medical University approved the database and the study design. Patient consent was waived due to the retrospective nature of the study. Patients who underwent sublobar resection (wedge or segmental resection) or multi-lobe resection (pneumonectomy or bilobectomy) were excluded. All patients were preoperatively evaluated by pulmonary function test with blood gas analysis, contrast-enhanced computed tomography (CT) scans of the chest and upper abdomen, flexible bronchoscopy, brain magnetic resonance imaging, and bone scintigraphy. If the lymph node had a diameter longer than 10 mm, positron emission tomography was performed. Preoperative tissue diagnosis of NSCLC by CT-guided fine needle aspiration or transbronchial biopsy was done in selected patients. Endobronchial ultrasonography or mediastinoscopy was not used routinely.
For analysis of baseline characteristics and perioperative outcomes, the following variables were analyzed: sex, age, body mass index (BMI), smoking status (never-smokers were defined as patients who smoked fewer than 100 cigarettes in their lifetime), associated comorbidities, preoperative pulmonary functional assessment, American Society of Anesthesiologists (ASA) physical status classification, tumor location, operation time (defined as the time in minutes from skin incision to final skin closure), estimated blood loss (estimated by assessment of the suction bottles, sponges, and the surgical drapes and gowns), intraoperative transfusion, duration of chest drainage (defined as from the day of the operation until the chest tube was removed), postoperative hospital stay (defined as from the day of the surgical procedure to the day of discharge), conversion (defined as unplanned extension of the incision and rib spreading beyond that required for specimen extraction), postoperative complications (defined as Grade 2 or above for severe complications requiring medical or surgical interventions under the Clavien-Dindo classification system within 30 postoperative days), 12 and 30-day operative mortality (defined as death during the same hospitalization or within 30 days after the operation). In addition, lymph node data (number of harvested lymph nodes and sampled mediastinal stations) and pathologic staging according to the TNM classification of the American Joint Commission on Cancer Staging Manual (Seventh Edition) were recorded to investigate pathologic outcomes.
Surgery
All procedures were performed in the lateral decubitus position with single lung ventilation. VATS lobectomy was performed by using a three-port non-rib spreading technique with standard thoracoscopic instruments. A 4-cm anterior utility incision through the fourth or fifth intercostal space was used. The 1-cm camera port was placed in the seventh or eighth intercostal space at the anterior axillary line. The first assistant used a 1-cm posterior port in the seventh intercostal space at the posterior axillary line for lung retraction. The pulmonary vein, pulmonary artery, and lobar bronchus were individually divided with an endoscopic stapler (Ethicon Endo-Surgery, Inc., Cincinnati, OH). Fissures were completed with either sharp dissection or endoscopic staplers, and the specimen was retrieved with an endoscopic bag. Systematic mediastinal and hilar lymph node dissections were performed for all cases. Mediastinal lymph nodes stations addressed typically included 2, 4, 7, 8, and 9 for right-sided resections and 5, 6, 7, 8, and 9 for left-sided resections. One chest tube was used for postoperative drainage in all patients. Epidural analgesia is avoided in all patients. Postoperative pain control was achieved by a combination of intercostal nerve blocks during the operation and postoperative patient-controlled analgesia. Patients were routinely discharged 2 days after chest tube removal.
Moving average method
The moving average method is used with time series data to smooth out short-term fluctuations and highlight longer-term trends or cycles. It was created by an average of subsets, which were modified by adding new data to the subsets and then by shifting forward all data sets. In this study, we applied the method to the operation time of VATS lobectomy, with a moving average order of 5 cases to apprehend the overall trend of data by detection of cumulative changes from average values. 23
CUSUM method
CUSUM is a statistical technique that shows the sequential difference between the individual data and the target value. The CUSUM is the running total of differences between the individual data points and the mean of all data points; xi represents the individual data points, and μ represents the mean of all data points: CUSUM =
Statistical analysis
Variables were analyzed as proportions, means, or medians with variability estimates in the form of standard deviation and interquartile ranges (IQR), as appropriate. Statistical analyses of the continuous data were performed by using Independent-Samples t-test for normally distributed data and the Mann–Whitney U test for skewed data. Categorical data were compared by using the χ2 test and the Mann–Whitney U test. All statistical analyses were carried out with SPSS for Mac (version 22.0; IBM, New York). The moving average method and the CUSUM method were calculated by Microsoft Excel for Mac version 2013 (Microsoft Corporation, Redmond, WA). Differences were considered significant for P < .05 (two sided).
Results
Overall patient characteristics
A total of 67 patients with lung cancer underwent VATS. Their mean age was 58.5 ± 9.4 years old, and 41 (61.2%) were men. Baseline, perioperative, and histopathologic characteristics of the entire cohort are listed in Table 1. The tumor was located in 52.2% of the right lung, and in 47.8% of the left lung. The mean operative time was 173.2 ± 51.1 minutes, and the median estimated blood loss was 100 mL (IQR 50–150). The median postoperative duration of chest drainage was 3.0 days, and the median postoperative hospital stay was 6.0 days. Pathologic stage I, II, and III were observed in 48 (71.6%), 10 (14.9%), and 9 (13.4%) patients, respectively. There was 1 (1.5%) conversion to thoracotomy due to bleeding from the pulmonary artery. Postoperative complications more than Grade 2 based on Clavien-Dindo classification were observed in 14 (20.9%) patients. The median number of harvested lymph nodes and median sampled mediastinal stations were 12.0 and 3.0, respectively. There were no 30-day operative mortalities.
Independent-Samples t-test.
χ2 test.
Mann–Whitney U test.
ASA, American Society of Anesthesiologists; BMI, body mass index; CAD, coronary disease; COPD, chronic obstructive pulmonary disease; CVD, cerebral vascular disease; DLCO, diffusion capacity of the lung for carbon monoxide; FEV1, forced expiratory volume in 1 second; IQR, interquartile range; SD, standard deviation.
Determining the learning curve
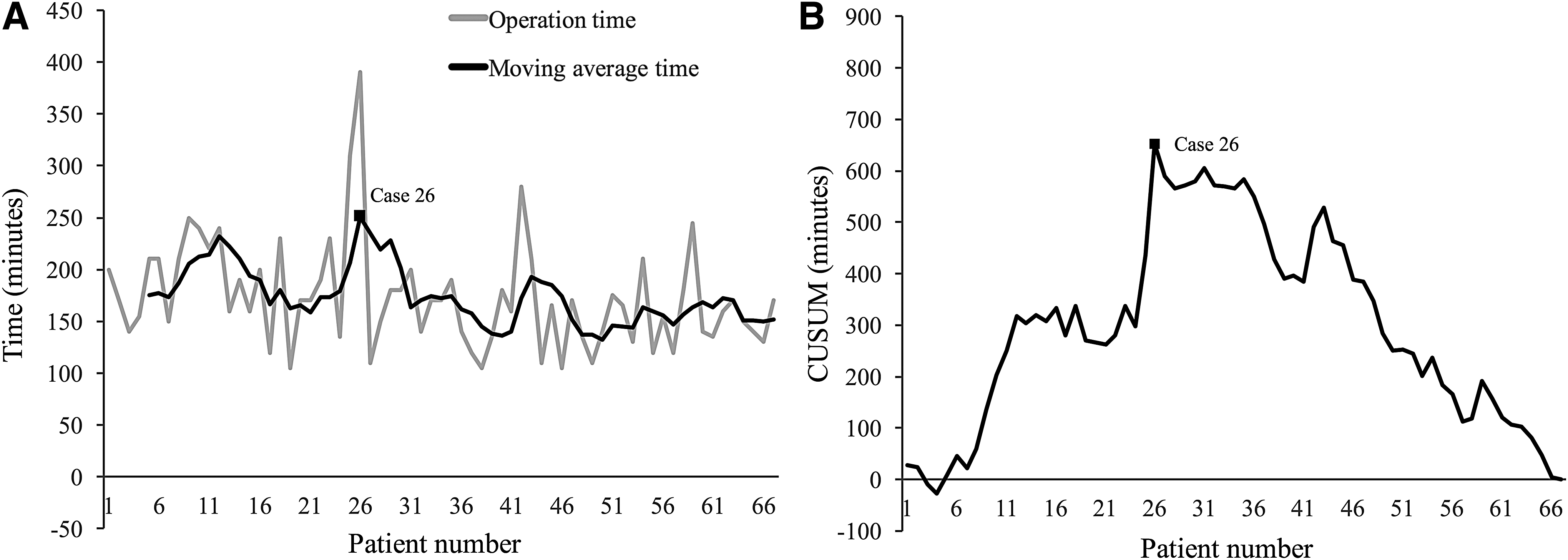
The moving average method showed the overall trends for the operation time; the peak point occurred at the 26th case (Fig. 1A). According to the CUSUM for the operation time, the operation time peak point also occurred at the 26th case (Fig. 1B). As these results indicated that the learning curve for VATS for lung cancer peaked at the 26th cases, we divided the patients into two groups at the 26th case: early-experience group (n = 26), cases 1 to 26; and late-experience group (n = 41), cases 27 to 67 (Table 1).
Demographic and clinical characteristics of the two groups are reported in Table1. The most frequently reported comorbidities were hypertension, coronary artery disease, cerebral vascular disease, chronic obstructive pulmonary disease, and diabetes. There were no significant differences in the frequency of major comorbidities between the two groups. There were no significant differences in age, sex, BMI, smoking status, preoperative pulmonary functional assessment, ASA physical status classification, and tumor location between the early- and late-experience groups.
One patient required conversion to an open procedure due to the pulmonary artery bleeding after stapling, which occurred in the early-experience group (P = .388). Operation time in the early-experience group was longer than in the late-experience group (mean 198.3 minutes versus 157.3 minutes; P = .001). Compared with the early-experience group, estimated blood loss was observed to decrease in the late-experience group (median 100 mL versus 100 mL; P = .049). For the management of chest tubes, there were significant differences in the duration of chest drainage between the two groups, and chest tubes were removed early in the late-experience group of patients (median 3.0 days versus 2.0 days; P < .001). Postoperative hospital stay decreased significantly from a median of 7.0 days in the early-experience group to 6.0 days in the late-experience group (P < .001). Between the two groups, more patients in the late-experience group were diagnosed with lung adenocarcinoma at the time of the surgical resection (73.1% versus 90.2%, P = .006). There were no significant differences in postoperative complications (Grade 2 or above based on Clavien-Dindo classification), lymph node data (number of harvested lymph nodes and sampled mediastinal stations), and pathologic staging between the two groups.
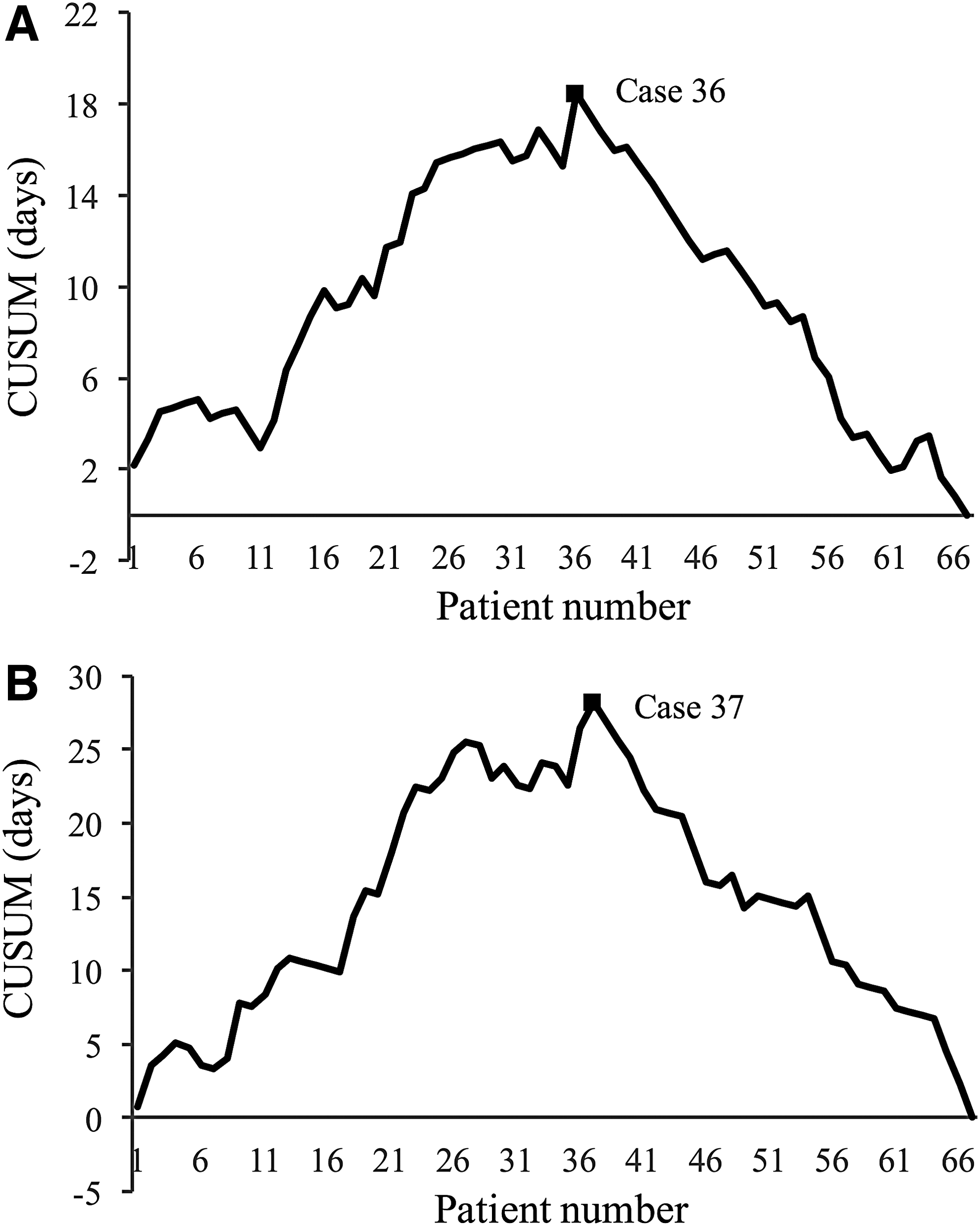
On visual analysis of the CUSUM chart, an inflexion point for decreasing chest tube duration was observed after case 36, as shown in Figure 2A. In the case of postoperative hospital stay, an inflexion point was seen after case 37, as shown in Figure 2B.
Discussion
As the most advisable treatment, pulmonary lobectomy offers a potential cure for patients with lung cancer. However, conventional open lobectomy has the disadvantages of extensive trauma, severe postoperative pain, long recovery time, and high risk of complication. 13 Therefore, there has been increasing interest in adopting minimally invasive approaches to lobectomy in an attempt to improve postoperative outcomes. Since the early 1990s, lobectomy using VATS technology has been described and widely applied around the world. Studies have provided strong evidence that VATS lobectomy is an acceptable alternative to traditional open lobectomy.14–16 However, even with these advantages, VATS lobectomy is a challenging procedure for beginner thoracic surgeons that requires experience in handling the instruments, obstacles created by inappropriate port incisions, and most of all, catastrophic events resulting from pulmonary vessel injury.5,7 Therefore, it is important to determine the learning curve, because this indicates whether this technique procedure can be successfully taught to residents, fellows, and thoracic surgeons who are looking to transition in their practice.
The learning curve for VATS lobectomy has been previously reported. Li et al. previously analyzed the learning curve for VATS lobectomy with the CUSUM method. They reported that to achieve proficiency in performing VATS lobectomy required more than 100 cases of personal experience to develop efficiency, and attaining consistency required 200 or more cases. 17 Zhao et al. reported the learning curve for VATS lobectomy, with patients simply divided into three groups and compared. They concluded that the learning curve for VATS lobectomy for lung cancer was overcome after ∼30 consecutive patients. 5 Ra et al. suggested that it took 6 months for young surgeons without experience in VATS lobectomy to be able to reliably perform a VATS lobectomy, but their study included a small number of patients (n = 38) and failed to mentioned how many cases were needed to overcome the learning curve. 7 As can be seen here, most previous reports used just one statistical method to analyze the learning curve. Decreasing the operation time is one of the most important factors that reflects surgical proficiency. 9 However, operation time at a specific point cannot fully reflect the entire learning curve. Therefore, to have a better understanding of the surgeon's performance in VATS lobectomy, we applied the moving average and CUSUM methodology to determine the learning curve when the outcomes of interest started to improve significantly. As shown in Figure 1A, the trends for operation time were clearly demonstrated by the moving average method. After the 26th case, an inflexion point of decreasing operation time was observed. The CUSUM, which shows the sequential changes between each case and the mean value, revealed a similar inflexion point of operation time as the moving average method (Fig. 1B). Therefore, a reasonable learning curve for a VATS lobectomy may require more than 26 cases of operation.
Our findings suggested that successful surgery for VATS lobectomy was achieved after 26 cases. Even then, we cannot simply compare our results with those of previous reports, because many other factors, in addition to a surgeon's experience, can influence the time required to complete the surgery. We do believe that several factors help to reduce our learning curve of VATS lobectomy.
First, before the implementation of this technology, we standardized our VATS lobectomy procedure. As shown in Figure 3, after entering the thoracic cavity, we first released the inferior pulmonary ligament and completely opened the pleural around the hilum of the lung. This process might help early detection of vascular and bronchial abnormalities, and it might facilitate the dissection of the pulmonary vessels, bronchi, and fissure. Such a protocol allowed us to be more efficient and safe in the implementation of this technology. Second, during the procedure of learning VATS lobectomy, three-dimensional (3D) reconstruction images based on the multidetector CT were used for preoperative surgical simulation. Due to the great variability of pulmonary vessels and bronchi, preoperative understanding of the anatomy of these structures would make VATS safer. Using the 3D images for preoperative surgical simulation would increase the surgeon's confidence in maneuvering complicated procedures such as VATS lobectomy. 24
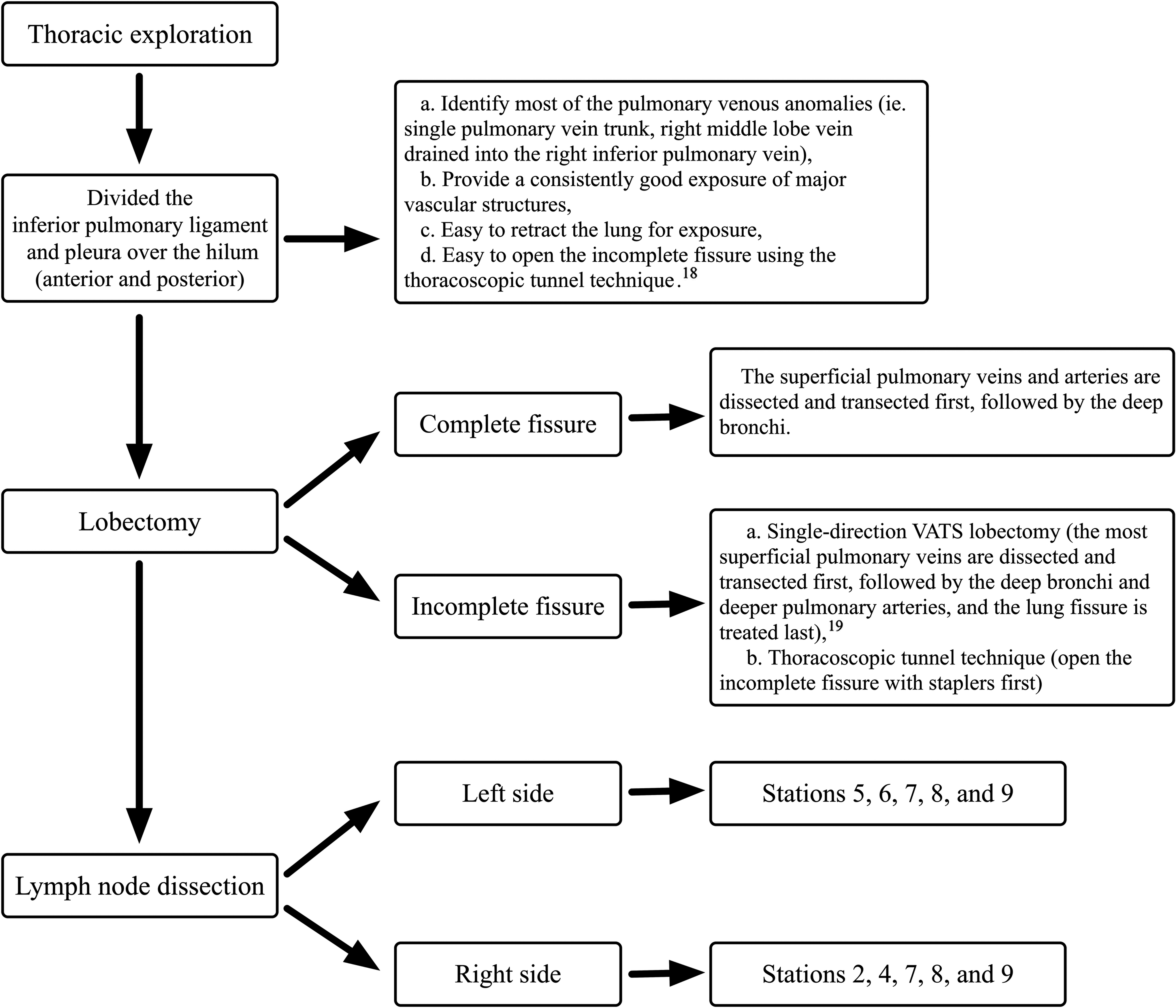
Flow diagram of VATS lobectomy for lung cancer. VATS, video-assisted thoracic surgical.
Third, in learning VATS lobectomy, thoracoscopic esophagectomy was also introduced to our department as an alternative of open Sweet esophagectomy (left thoracic esophagectomy). Performing thoracoscopic esophagectomy allowed us to have a better understanding of the mediastinal anatomy, which was helpful to the mediastinal lymph node dissection. Fourth, performance review using videotapes is a strategy employed to improve future performance. 20 In our department, we have established a minimally invasive surgical video database for reviewing. During the past several years, a huge number of surgical videos and teaching courses have been loaded on specialized websites. With the video database, we could easily review and compare our surgical procedures with those performed by other surgeons to improve our surgical skills.
When we divided the patients into two groups reflecting the experience level of the surgeon with the technique, the late-experience groups exhibited a shorter operation time, less estimated blood loss, shorter duration of chest drainage, and shorter postoperative hospital stay. With more VATS experience acquired by the surgeon and the surgical team, the decrease in operation time was expected. However, the difference in the duration of chest drainage and postoperative hospital stay between groups might reflect differences in the postoperative management. According to the CUSUM chart for chest tube duration and postoperative hospital stay, similar trends were observed. A possible explanation is that we usually have the patients discharged 2 days after the chest tube removal, if no contraindication was identified. In recent years, several studies on early chest tube removal from the pleural cavity after pulmonary resection have been made. Bjerregaard et al. reported it safe to remove chest tubes, despite drainage of 450 mL/day after lobectomy by VATS. 21 Xie et al. performed a prospective randomized study and found that a threshold volume of 300 mL/day for chest tube removal after VATS lobectomy was feasible and safe. 22
To achieve a better postoperative satisfaction in patients after VATS lobectomy, we implemented a new protocol for the chest tube management from the 35th patient. First, chest tubes removal protocol was changed from a drainage volume <150 to <250 mL/day. Second, to promote compensatory postoperative volume increase of the remaining lung, the chest tube was placed to suction (−10 cm H2O) when the patient was transferred into the general ward. There were no differences in postoperative complications rates between the two groups. However, we cannot state that using new chest tube management protocol is a feasible technique, since we have measured just one parameter in the present study. Future large, prospective, controlled studies are, therefore, needed in addressing this clinical issue. Our study also showed that more patients were diagnosed with lung adenocarcinoma at the time of the surgical resection in the late-experience group, as compared with the early-experience group. We do not have a reasonable explanation for that. Perhaps this represented only a statistical bias in consequence of the difference between the numbers of cases in both groups.
There are a number of potential limitations in this study. It represents the learning curve of a single surgeon in a single center with small samples. All VATS lobectomies in this study were performed by a surgeon with more than 5 years of thoracic surgery experience. We are not sure whether such perioperative results could be reproduced by a new learner who has little or no experience with conventional open thoracic surgery. Second, as the impact of a surgical approach on oncologic outcomes is an important consideration, a long-term follow-up will be needed to retrieve oncological information of this series. Finally, there might be biases in the selection of patients because of the retrospective nature of this study. Despite the mentioned limitations, we believe that the present work could be useful to guide those who may be considering adding VATS lobectomy to their armamentarium.
Conclusions
We have described the learning curve for VATS lobectomy by a single surgeon. We applied the moving average analysis and the CUSUM analysis to try to identify more precisely the moment when favorable results were observed. Our findings suggest that the intraoperative and postoperative care parameters are improved after 26 cases, which means that a successful surgery has been achieved. We expect that these results can help shorten the learning curve for VATS lobectomy beginners.
Footnotes
Acknowledgment
The authors would like to thank Prof. Liang Chen from the First Affiliated Hospital of Nanjing Medical University for providing useful suggestions.
Disclosure Statement
No competing financial interests exist.