
Abstract
Abstract
Background:
Severe acute pancreatitis (SAP), one severe and fatal disease, the therapy of which is pretty hard. This study aimed to study the effect of laparoscopic peritoneal lavage and drainage (LPLD) and continuous venovenous diahemofiltration (CVVDH) on SAP.
Materials and Methods:
Two hundred forty-five patients with SAP in total were randomly assigned into four groups according to the therapeutic plan: basic treatment; LPLD; CVVDH; or LPLD+CVVDH. Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, the ratios of multiple organ dysfunction syndrome (MODS), mortality, hospitalization time, hospitalization cost, ratios of complications, the abdominal distention relief time, abdominal pain relief time, plasma concentration of endotoxin, tumor necrosis factor-α (TNF-α), interleukin (IL)-6, and IL-8 were evaluated.
Results:
Ratios of MODS, mortality, hospitalization time, hospitalization cost, the abdominal distention relief time, abdominal pain relief time, concentration of endotoxin, TNF-α, IL-6, IL-8, and APACHE II scores were significantly decreased in the CVVDH, LPLD, and CVVDH+LPLD groups, while ratios of recovery were significantly increased in the CVVDH, LPLD, and CVVDH+LPLD groups, especially in the CVVDH+LPLD group.
Conclusions:
LPLD and CVVDH are effective in the treatment of SAP by eliminating endotoxin, TNF-α, IL-6, and IL-8. The combination of CVVDH and LPLD can further improve the treatment effect.
Introduction
S
The morbidity and mortality of SAP are determined greatly by the extent of the related inflammatory response, which is mediated by a variety of cytokines, including proinflammatory cytokines, such as tumor necrosis factor-α (TNF-α), interleukin (IL)-6, and IL-8. These cytokines may injure the microcirculation endothelium and increase the capillary permeability and fluid sequestration, resulting in capillary leakage syndrome and multiple organ dysfunction syndrome (MODS).4–6
As is known, laparoscopic peritoneal lavage and drainage (LPLD) can protect the function of the important organ and reduce the occurrence of MODS by eliminating the accumulation of inflammatory mediators in the abdominal cavity and preventing the progress of local lesion. 7 Besides, continuous venovenous diahemofiltration (CVVDH) can effectively remove the early pancreatic enzymes, inflammatory mediators, cytokines, and endotoxin in the plasma. 8 Therefore, this study, based on all of the facts, aimed to evaluate the effects of monotherapy or combined therapy of LPLD and CVVDH on SAP.
Materials and Methods
Human subjects
This is a retrospective and randomized clinical study with a total of 245 patients diagnosed with SAP, who were admitted to the hospital from January 2004 to September 2015. SAP was diagnosed by referring to the criteria described in the Consensus of the International Symposium on Acute Pancreatitis (Atlanta definition). According to a random number table, the patients were divided into four groups: (1) basic treatment; (2) LPLD; (3) CVVDH; and (4) LPLD+CVVDH. SAP was characterized by one or more of the following characters: (1) systemic inflammatory response syndrome (SIRS); (2) persistent organ failure (defined by the Modified Marshall Scoring System) (> 48 hours); (3) CT scores of pancreas ≥6; and (4) Acute Physiology and Chronic Health Evaluation II (APACHE II) scores ≥8. Exclusion criteria included the following: (1) evidence or a known history of renal dysfunction (creatinine >1.5 mg/dL); (2) pregnancy, malignancy, or immunodeficiency; and (3) preexisting chronic kidney diseases requiring regular hemodialysis. This study protocol was approved by the Ethics Committee of Gannan Medical University, Ganzhou, China. The informed consent was obtained from all subjects. There were no statistical differences between the four groups in the serum level of amylase, CTSI (CT scan severity index), APACHE II scores, abdominal compartment syndrome rate, and severity grade ratio. Patient demographic data are shown in Table 1.
CVVDH, continuous venovenous diahemofiltration; LPLD, laparoscopic peritoneal lavage and drainage.
Basic treatment
Patients accepted traditional conventional therapy, including enteral nutrition, parenteral nutrition, somatostatin, antibiotic fluid replacement, gastric acid secretion inhibition, gastrointestinal decompression, and otherwise.
LPLD procedure: The surgery was performed by the same group of doctors within 72 hours after the patients were admitted into the hospital. The detailed procedure was as follows: (1) after the patient was generally anesthetized, a 12-mm incision was made on the posterior axillary line and 2 cm under the 12th costal margin; (2) muscles and lumbodorsal fascia were bluntly separated to the retroperitoneal space by fingers with the help of long curved forceps; (3) a water capsule was placed in the retroperitoneal space and filled with 300–400 mL normal saline to expand the space and form a lacuna; (4) a 12-mm trocar was placed after the removal of the water capsule with the normal saline; (5) a 10-mm transverse incision was made 1 cm above the iliac crest in the midaxillary line; (6) forceps were used to bluntly separate muscles and fascia to the lacuna; (7) a 10-mm trocar was placed and used to aerate until the lacuna pressure reached 10–14 mmHg; (8) the laparoscope was used and a 5-mm trocar was inserted 2 cm below the anterior axillary line of the costal arch under direct endoscopic observation; (9) the perirenal fascia was opened along the front of the psoas muscle from the retrocolic space and then the retroperitoneal space was opened along the top of the pancreatic tail until the lesser sac; (10) the pus or effusion in the retroperitoneal space was sucked out by an aspirator and necrotic tissue was removed by forceps; (11) two to three drainage tubes were placed in the top of the pancreas and retrocolic space after the removal of necrotic tissue and pus for the patients with left retroperitoneal abscess; and (12) for patients with right retroperitoneal abscess, the perirenal fascia was opened and the anteromedial dissection continued until the duodenum was reached, and then two to three drainage tubes were placed in the retroduodenal space, anterior extrarenal space, and retrocolic space.
Continuous venovenous diahemofiltration
After the patients had been admitted into the hospital for 24 hours, CVVDH was performed and lasted for 72 hours. As to vascular access, a double coaxial lumen 14F catheter was inserted percutaneously through the right internal jugular or femoral vein by using the Seldinger technique. A Baxter BM25 system (Baxter) was used for CVVDH with a polyacrylonitrile NA69 hemofilter (1.2 m2 surface area, 35-kDa limit; Hospal). Blood flow was set at 50–75 mL/min and ultrafiltrate flow at 1000 mL/h, transmembrane pressure was maintained in 450–460 mmHg, and the replacement fluid was prediluted and infused. Low-molecular-weight heparin was used as the anticoagulant. Patient-activated clotting time was adjusted to 60–70 seconds and a strictly neutral balance was maintained through a digital balance system (Baxter). CVVDH was maintained for a mean of 6 days (ranged 3–8). The AN69 hemofilter (1.2 m2) was changed every 24 hours.
Assessment of APACHE II scores and clinical parameters
APACHE II scores, defined by Microsoft APACHE II graded computer program Version 5.1, were applied for analysis. MODS was defined as two or more organs having persistently two or more Marshall subscores for >24 hours despite aggressive resuscitation and organ support. All patients with SAP were detected by contrast-enhanced CT on admission. The contrast-enhanced CTSI was used to evaluate the severity of pancreatitis. Clinical parameters included the following: abdomen pain and releasing time of abdomen distention, ratio of recovery, incidence of complication, the average hospitalization time, cost of hospitalization, and mortality.
Measurement of plasma endotoxin levels
Plasma endotoxin concentration was measured by the Tachypleus Amebocyte Lysate Kit (Shanghai Medical Science and Technology Corporation, Shanghai, China). Plasma samples treated with heparin were diluted 1:10 with pyrogen-free water and heated for 10 minutes at 75°C. Fifty microliters of the inactivated sample was added to 50 μL of solution A and the mixture was incubated for 33 minutes at 37°C. Next, 100 μL of solution B, diluted 1:2 with solution C, and was then added to the mixture followed by incubation for 3 minutes at 37°C. The extinction of endotoxin was determined by calculating the absorbance by using a spectrophotometer at 405 nm. The endotoxin concentration of an unknown sample was determined by a simultaneously established standard curve developed from a pool of plasma from 20 healthy volunteers whose plasma has no endotoxin. The endotoxin concentration was expressed as endotoxin units (EU) per mL.
Cytokine quantification
Peripheral blood samples from the SAP patients were collected, respectively, at six time points: before treatment, the 1st, the 2nd, the 3rd, the 7th, and the 14th day after the onset of treatment. Peripheral blood samples were centrifuged to collect serum, which was then dispensed in 50-μL aliquots and stored at −20°C before experiments. Plasma concentrations of TNF-α, IL-6, and IL-8 were determined using enzyme-linked immunosorbent assay (ELISA) kits following the manufacturer's instructions (R&D).
Statistical analysis
All data were prepared and compiled by the SPSS computer program (version 19.0 for Windows). The data were expressed as mean ± standard error of the mean. Analysis of variance was used to compare data among the four groups when they were normally distributed. Chi-squared test and Fisher's exact test were used for quantitative data analysis. P < .05 was considered statistical significance.
Results
Comparison of APACHE II scores
As shown in Figure 1, on the third day after the onset of treatment, APACHE II scores were decreased in the LPLD group, CVVDH group, and LPLD+CVVDH group, and the decrease in the LPLD+CVVDH group is much more obvious than that in the LPLD group or CVVDH group.
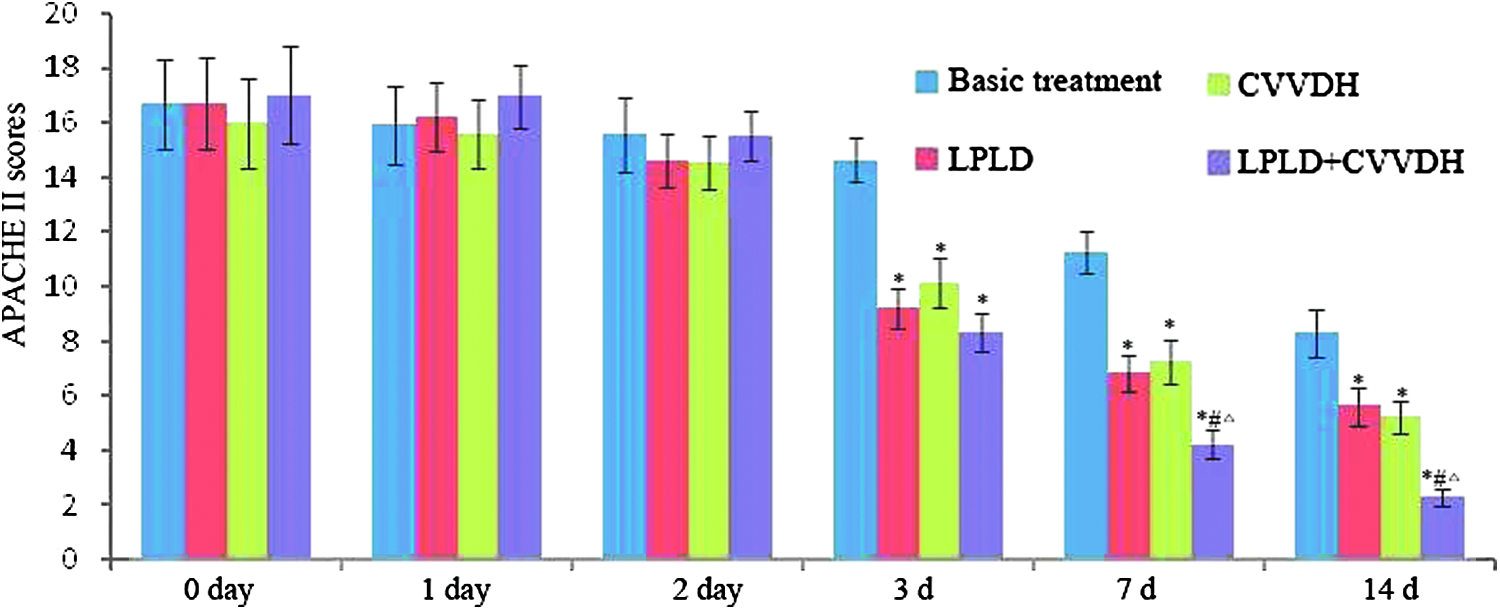
Comparison of APACHE II scores in the four groups. *versus Basic treatment, P < .05; #versus LPLD, P < .05; Δversus CVVDH group, P < .05. CVVDH, continuous venovenous diahemofiltration; LPLD, laparoscopic peritoneal lavage and drainage; APACHE II, Acute Physiology and Chronic Health Evaluation II.
Comparison of clinical parameters
As shown in Table 2, abdominal distention relief time and abdominal pain relief time experienced by patients in LPLD, CVVDH, and LPLD+CVVDH group were significantly shorter than those by patients in the basic treatment group, with the shortest in the LPLD+CVVDH group. Mean time of hospitalization, time of recovery to normal heart rate, time of recovery to normal respiration rate, abdominal distention relief time, abdominal pain relief time, and the time of recovery to normal blood amylase and glucose in the LPLD group, the CVVDH group, and LPLD+CVVDH subgroups were largely decreased compared with those in the basic treatment group. The incidence of MODS was 18.3%, 11.3%, 12.3%, and 6.9% in the basic treatment, LPLD, CVVDH, and LPLD+CVVDH group, and the incidence of mortality was 20%, 11.3%, 12.3%, and 6.9%, respectively. In terms of the incidence of MODS, mortality, and cure rate, there were statistical differences in the incidence of complication between the basic treatment group and other three groups or among the three experimental groups.
Cure means “the patients recovered completely.”
versus Basic treatment, P < .05.
versus LPLD, P < .05.
versus CVVDH group, P < .05.
CVVDH, continuous venovenous diahemofiltration; MODS, multiple organ dysfunction syndrome; LPLD, laparoscopic peritoneal lavage and drainage.
Changes of plasma endotoxin levels
As shown in Figure 2, plasma endotoxin levels were decreased greatly on the third day after the onset of treatment in the LPLD group and on the first day after the onset of treatment in the CVVDH group. The levels were further decreased in the LPLD+CVVDH group on the third day after the onset of treatment.
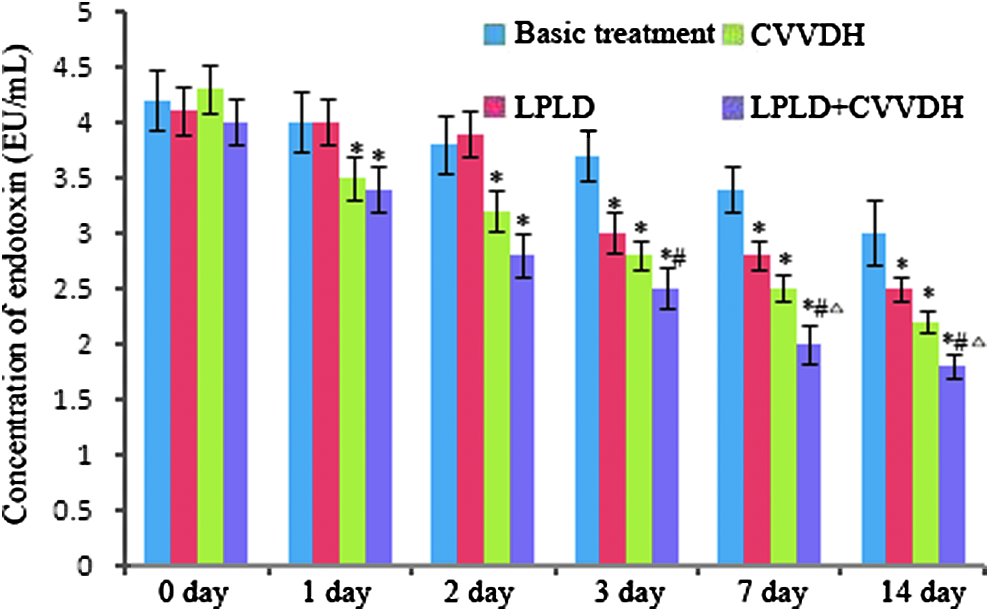
Changes of plasma endotoxin levels in the four groups. *versus Basic treatment, P < .05; #versus LPLD, P < .05; Δversus CVVDH group, P < .05. CVVDH, continuous venovenous diahemofiltration; LPLD, laparoscopic peritoneal lavage and drainage.
Changes of plasma cytokine levels
As shown in Figure 3, TNF-α level was extremely high in SAP patients. After treatment, TNF-α levels were decreased on the third day after the onset of treatment in the LPLD group and on the first day after the onset of treatment in the CVVDH group, and decreased more in the LPLD+CVVDH group on the third day after the onset of treatment.
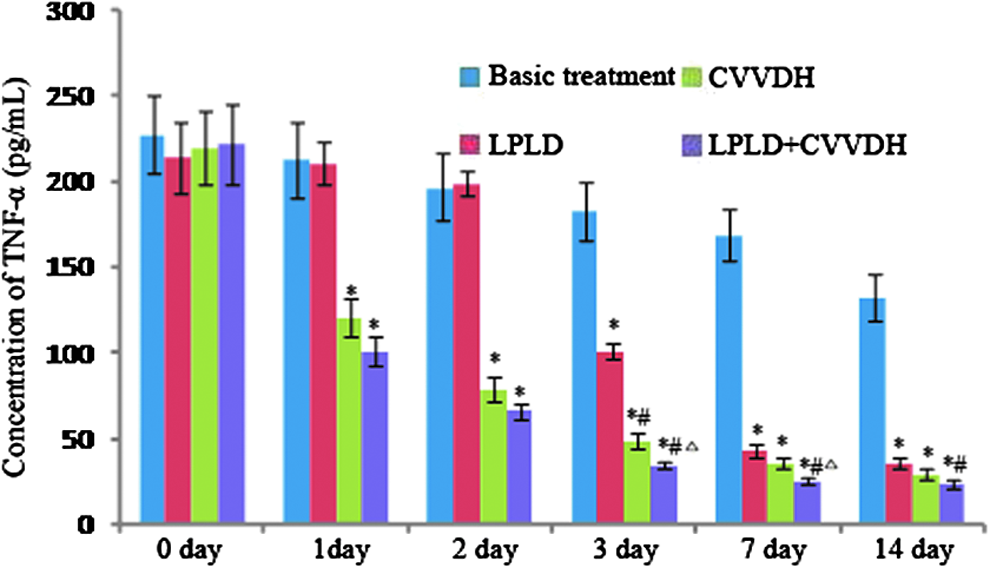
Changes of plasma TNF-α levels in the four groups. *versus Basic treatment, P < .05; #versus LPLD, P < .05; Δversus CVVDH group, P < .05. CVVDH, continuous venovenous diahemofiltration; LPLD, laparoscopic peritoneal lavage and drainage; TNF-α, tumor necrosis factor-α.
As shown in Figures 4 and 5, the levels of IL-6 and IL-8 were much higher in SAP patients. After treatment, the levels of IL-6 and IL-8 were decreased on the third day after the onset of treatment in the LPLD group and on the first day after the onset of treatment in the CVVDH group, and greatly decreased in the LPLD+CVVDH group on the third day after the onset of treatment.

Changes of plasma IL-6 levels in the four groups. *versus Basic treatment, P < .05; #versus LPLD, P < .05; Δversus CVVDH group, P < .05. CVVDH, continuous venovenous diahemofiltration; IL, interleukin; LPLD, laparoscopic peritoneal lavage and drainage.
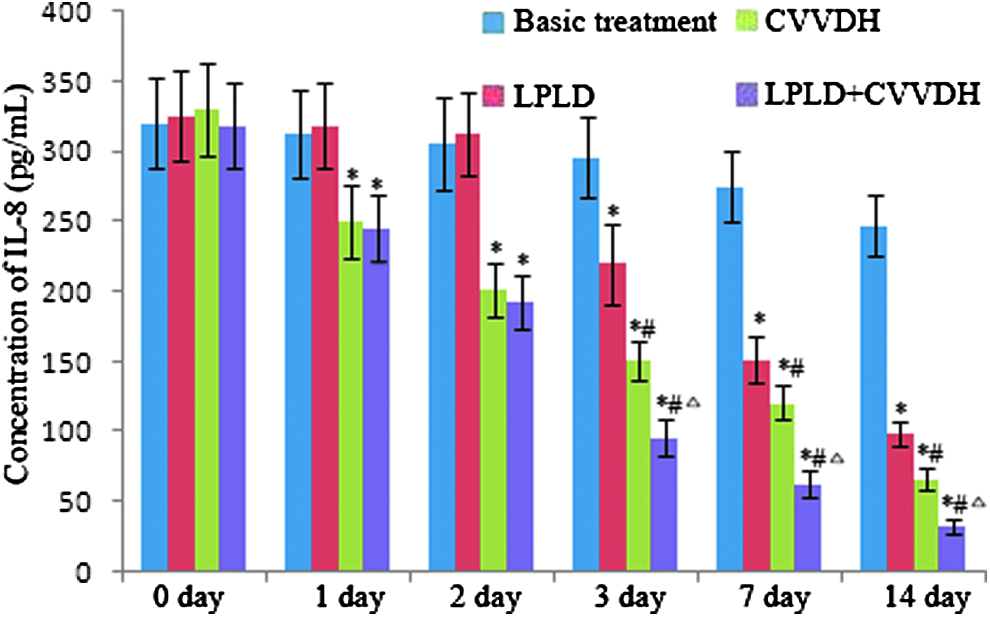
Changes of plasma IL-8 levels in the four groups. *versus Basic treatment, P < .05; #versus LPLD, P < .05; Δversus CVVDH group, P < .05. CVVDH, continuous venovenous diahemofiltration; IL, interleukin; LPLD, laparoscopic peritoneal lavage and drainage.
Discussion
SAP is associated with SIRS, the presence of pancreatic and peripancreatic inflammation, retroperitoneal edema, and peritoneal fluid due to the leakage of pancreatic fluid followed by the disruption and necrosis of pancreatic parenchyma, including pancreatic ductules. As an inflammatory process, SAP triggers excessive leukocyte activation and migration of neutrophils to the inflamed area with a consequent release of endotoxin, proinflammatory mediators, including interleukins (IL-β, IL-6, IL-8, IL-10, IL-18, and so on) and TNF-α, described as a “cytokine storm,” which results in an uncontrolled pathogenic progression of a pancreatic infection to necrosis and consequently to SIRS and multiorgan failure.9–11 TNF-α, a mediator of induced neutrophil activation, is involved in the pathophysiological responses and plays an important role in promoting pancreatic injury during pancreatitis. 12 IL-8 is one of the most important inflammatory mediators in acute pancreatitis and other inflammatory processes. 13 IL-6, another early mark of the inflammatory cascade, will induce the chemokines, chemokine (C-C motif) Ligand 2 protein (CCL2) and IL-8, and aggravate the inflammatory response. 14 Since SAP is mediated by proinflammatory cytokines and other inflammatory mediators, strategies for interrupting this process are the most effective form of therapy.15,16 LPLD, a microtrauma operation with little injury and interference on the body, can inspect the abdominal cavity and peripancreatic lesions accurately and clearly. Intraoperative lavage can reduce the intra-abdominal pressure, remove the necrotic tissue containing large amounts of pancreatic enzymes, dilute the pancreatin, inflammatory mediators, and translocate intestinal flora.17,18 CVVDH can overcome the imbalance between SIRS and CARS (Compensatory anti-inflammatory response syndrome) and restore the broad-based humoral homeostasis by normalizing the patients' water, electrolyte, and acid–base balance and homeostasis related to renal dysfunction, and removing most of the inflammatory mediators with moderate molecular weights (i.e., within the range of 5–60 kDa) such as cytokines, chemokines, complement components, thromboxanes, platelet-activating factor (PAF), leukotrienes, and kinins.19,20 Therefore, combination of CVVDH and LPLD can reach an accumulated effect in treating SAP.
In this study, we retrospectively estimated the efficacy of CVVDH and LPLD on treatment of SAP and found that the ratios of MODS, mortality, hospitalization time, and cost of hospitalization were lower, while ratios of recovery were higher in the CVVDH, LPLD, and the CVVDH+LPLD subgroups compared to the basic treatment subgroup. Endotoxin, TNF-α, IL-6, and IL-8 levels on the first day and APACHE II scores on the third day after treatment showed considerable decrease in the CVVDH subgroup compared to the basic treatment subgroup, while the above parameters on the third day after treatment showed significant decrease in the LPLD subgroup compared to the basic treatment subgroup. The abdominal pain relief times in the LPLD group were shorter than those in CVVDH group. All of the above parameters are further enhanced in the CVVDH+LPLD group than the monotherapy of CVVDH or LPLD subgroups alone. These results showed that LPLD can relieve the clinical symptoms more effectively than CVVDH, while CVVDH can eliminate cytokines more effectively than LPLD. Both will decrease APACHE II scores, reduce the incidence of MODS and mortality, reduce the hospitalization time and cost of hospitalization, and improve the cure rate. In addition, the combined therapy of CVVDH+LPLD can further enhance these benefits.
In conclusion, LPLD and CVVDH are effective in treating SAP by eliminating endotoxin, TNF-α, IL-6, and IL-8. The combined therapy of CVVDH+LPLD can further improve the benefits than the treatments individually.
Footnotes
Acknowledgments
We acknowledge the support of National Natural Science Foundation of China (81360080, 81071594), the Science Foundation of Science and Technology Hall of Jiangxi Province, China (20091391308000), and Ethics Committee of Gannan Medical University.
Disclosure Statement
The authors declare that they have no conflict of interest.