
Abstract
Abstract
Background:
Colonoscopy outcome is limited by endoscope looping, which leads to patient discomfort, prolonged procedure, and increased sedation requirement. Traditional manual abdominal pressure is imprecise and manually intensive. A hands-free abdominal compression device (ACD) may improve colonoscopy outcome. We aimed to assess the effect of a novel ACD on colonoscopy outcomes compared to manual pressure.
Materials and Methods:
This was a prospective single-blinded study of patients undergoing outpatient colonoscopy. The ACD (N-Doe Pillow™) was applied on 50 consecutive patients. Endoscopists were blinded to device usage. Control cases using manual pressure were randomly selected in a 2:1 manner. Primary outcome was cecal intubation time. Secondary outcomes included sedation requirement and complications. Subgroup analyses evaluated ACD effect on endoscopists with different experiences and patients at higher risk of difficult colonoscopy. Fisher's exact and Student's t-tests were performed for univariate analyses. Multivariate analysis was performed using generalized linear regression.
Results:
Fifty patients undergoing colonoscopy with ACD assistance were compared to 100 matched controls. Mean cecal intubation time was significantly reduced in the ACD group compared to controls (6.38 minutes versus 11.8 minutes, P < .0001). Multivariate analysis showed that ACD use was independently associated with reduction in cecal intubation time (β-coeff: −4.11, P = .007). Subgroup analyses revealed a trend toward increased improvement in cecal intubation time among junior endoscopists and obese patients.
Conclusions:
A novel, hands-free ACD significantly decreased cecal intubation time in this prospective, single-blinded, match-controlled study. A trend toward more improvement was seen among junior faculty, suggesting an application for trainees and/or endoscopists with smaller case volumes.
Introduction
C
Several studies have shown that external abdominal pressure is effective at reducing loop formation. It has been demonstrated that if the pressure is applied properly, patient discomfort can be minimized and cecal intubation time decreased.7,8 However, traditional manual abdominal pressure applied by nursing staff is imprecise, manually intensive, and often ineffective. Furthermore, studies have shown that endoscopy nurses are at particular risk of developing musculoskeletal injuries of the neck, back, and upper extremities. One observational study exploring the occurrence of injury in this population found that as many as 33% of nurses were missing work due to work-related pain. 9
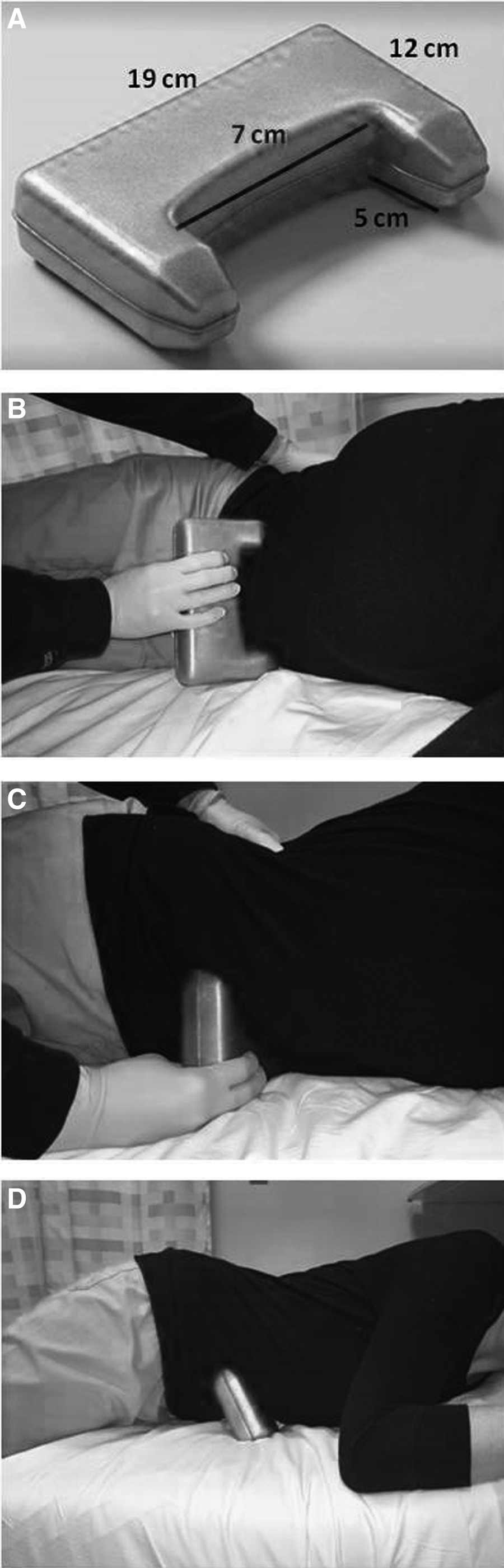
A novel abdominal compression device (ACD) has been developed to be used during colonoscopy to reduce or eliminate the need for manual pressure. This device, known as the N-Doe Pillow™ (NM Beale Co., Inc., Harvard, MA), is a hands-free, reusable ACD designed to apply external pressure on the patient's abdomen in three different pressure zones during colonoscopies (Fig. 1). When applied, this device can help reduce looping during colonoscopy similar to effective manual pressure, thereby promoting advancement of the endoscope and eliminating the need for manual compression by nursing staff. As the device utilizes the patients' own body weight to help apply constant pressure throughout the procedure in a standard manner, it may provide advantage over traditional manual pressure in colonoscope advancement by reducing the imprecision and inconsistency involved. Therefore, we hypothesized that this novel ACD would improve colonoscopy outcomes, including procedural time and patient comfort, over manual pressure. Moreover, since colonoscope looping and difficulty with advancement may affect less experienced endoscopists more significantly, the beneficial effect of the ACD may be more pronounced in early-career providers. In this study, we aimed to assess the effect of this novel ACD on objective colonoscopy outcome measures compared to traditional manual pressure.
Materials and Methods
This was a prospective, single-blinded, matched-cohort study of adult patients (age ≥18 years) who underwent elective outpatient colonoscopy between July and September 2013 at the endoscopy centers of an urban academic medical center and a satellite community ambulatory care center. All procedures involving trainees, patients with prior colonic resection, combined upper endoscopy and colonoscopy, and need for anesthesia support were excluded. Patients with known allergy and intolerance to benzodiazepines or opiates were also excluded from the study. Included patients were then randomly selected to undergo their procedures with the aid of the ACD (ACD group). A single endoscopy room was randomly selected every 10 days where all colonoscopies during that session were performed with the use of the ACD. The endoscopists were blinded to the use of the ACD. For 10 sessions, up to 5 cases were performed each time. A total of 50 cases were performed.
Controls whose procedures did not involve the use of ACD were then selected from the remaining cohort in a 2:1 manner, matched by age, gender, endoscopist, procedure location, indication, bowel preparation quality, and history of abdominal surgery (control group). All colonoscopies performed outside the 50 ACD cases at the two endoscopy centers during the 3-month period were candidates for being drawn as controls. For each of the 10 endoscopy sessions during which ACDs were used, the endoscopists and the location of the session were identified. Controls were then drawn from other sessions for each endoscopist at the same location. All patients of the same gender and at ± 5 years of each subject's age were then identified from the control sessions. We then excluded those patients with different bowel preparation quality reported or abdominal surgery history. Only screening colonoscopies were included for both groups.
All patients completed our unit's standard preprocedural preparation, including clear liquid-only diet on the day before the colonoscopy and an overnight fast. The standard bowel preparation used included two tablets of bisacodyl plus 238 g of polyethylene glycol on the day before the colonoscopy. However, if the procedure were scheduled after 11 AM, half of the polyethylene glycol solution was consumed in the morning of the colonoscopy. All subjects received intravenous midazolam and fentanyl for sedation, with medication titrated to patient comfort as per endoscopists' discretion. The standard procedural intravenous conscious sedation protocol of Brigham and Women's Hospital was observed for performance of all colonoscopies.
The included patients' demographics, medical history, procedure indication, sedation medication required, procedure time, complications, and procedural outcomes were reviewed. In addition, the endoscopists' years of experience in performing colonoscopy were also recorded. The primary outcome for the study was cecal intubation time, defined by the total minutes required for advancement from the anal verge to the cecum. Other outcomes analyzed included sedation medication requirements and procedural complication rates. Subgroup analyses were also performed to determine the effect of the ACD on procedural outcomes stratified by different endoscopist experience levels or patient risk factors for difficult colonoscopies. Endoscopists were classified as junior if they had < 5 years of colonoscopy experience. Those with 5 or more years of colonoscopy experience were considered senior endoscopists. Patient risk factors analyzed included gender (female versus male), age (≥65 versus < 65), and obesity (body mass index [BMI] ≥30 versus <30). The reduction in average cecal intubation time by ACD over manual pressure was compared between junior and senior endoscopists, male and female, older and younger patients, and obese and nonobese individuals to identify the differential effects of ACD on endoscopists of varying experiences and patients with different risk factors.
ACD group
In the ACD group, the patients were placed in the standard left lateral position, with the assistive device being applied to the sigmoid region before the start of procedure (Fig. 1). The endoscopists were blinded to the randomization and use of ACD in the patients. The nursing staff placed with ACD without the endoscopist present in the room, and the patients were draped in the same manner as we routinely do in our endoscopy center. The endoscopists were unable to see whether the device was present or not. Since the device is designed to be placed underneath the patient, routine draping easily concealed the presence of the ACD. The ACD was left in place until completion of the procedure. The colonoscopy would proceed as per standard protocol. Manual pressure by nursing staff was permitted if requested by the endoscopist.
Control group
All patients in the control group were also placed in the standard left lateral position for performance of the colonoscopy without the use of any assistive device. All patients were draped as per routine practice in our endoscopy center and in the same manner as the ACD group. Traditional manual pressure was applied as needed as per endoscopist's requests to aid passage of the colonoscope. The procedures were completed as per standard colonoscopy protocol.
Statistical analyses
All statistical analyses were performed using SAS 9.3 statistical package (SAS Institute, Inc., Cary, NC). Fisher's exact test for binary variables and Student's t-test for continuous variables were used to assess the differences between the two treatment groups. Multivariate analysis controlling for potential confounders, including age, sex, obesity, history of noncolonic abdominal surgery, and endoscopist experience (junior versus senior), was performed using generalized linear regression. Statistical significance was defined as P-values < .05.
This study was approved by the Human Research Committee of the Partners Institutional Review Board before inception.
Results
During the study period, 50 patients were randomly selected to undergo their elective outpatient colonoscopy with the application of ACD. One hundred matched controls who underwent routine outpatient colonoscopy, with the use of traditional manual pressure as needed, only were included in the study (Fig. 2). The overall cohort had a mean age of 58 years and 34% male patients, with no differences between the two study groups. Overall baseline demographics, procedural indication, history of abdominal surgery, and bowel preparation quality were similar between the ACD and control groups (Table 1).
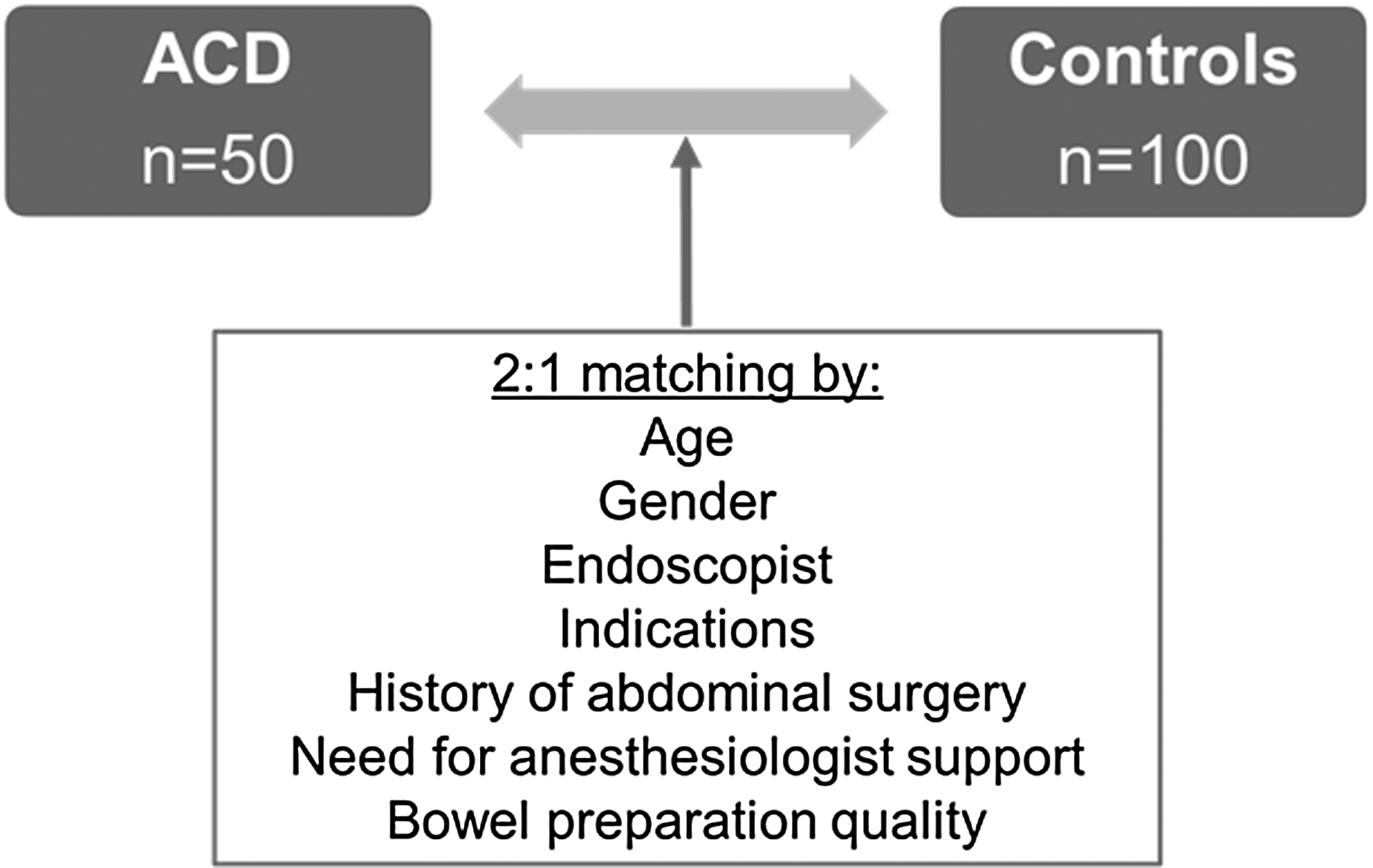
Flowchart of the selection and matching of the ACD and control groups. ACD, abdominal compression device.
ACD, abdominal compression device; BMI, body mass index; SD, standard deviation.
Procedural outcomes are listed in Table 2. Cecal intubation rate was 100% in both study groups. For the primary outcome, the ACD group demonstrated a significantly shorter cecal intubation time compared to the control group (6.38 ± 6.60 minutes versus 11.8 ± 3.92 minutes, P < .0001). The mean midazolam dosage requirement for sedation was similar between the two groups (4.72 ± 1.15 mg versus 4.57 ± 1.19 mg, P = NS), as was the mean fentanyl dose needed (110.3 ± 35.0 μg versus 117.3 ± 31.3 μg, P = NS). No procedural complication was noted in either patient group. Multivariate analysis controlling for potential confounders showed that ACD remained independently associated with significant reduction in cecal intubation time (β-coefficient −4.11, P = .007), while junior faculty status (β-coefficient 2.91, P = .02) and history of abdominal surgery (β-coefficient 2.44, P = .02) were associated with longer cecal intubation times (Table 3).
Statistically significant improvement in cecal intubation time was noted in the ACD group compared to controls. No other significant differences were noted in other outcomes.
ACD, abdominal compression device; SD, standard deviation.
ACD, abdominal compression device; BMI, body mass index.
In the secondary analysis of ACD effect on endoscopists of different experience levels, a trend for greater improvement in cecal intubation time with ACD was noted among junior endoscopists (< 5 years of colonoscopy experience) compared to senior endoscopists (>5 years of experience), although statistical significance was not reached (− 6.95 ± 6.58 minutes versus − 4.32 ± 5.14 minutes, P = .31) (Fig. 3). An interaction term, including junior faculty status and ACD use, was also incorporated into the multivariate regression model to assess for effect modification. Similarly, ACD use resulted in further reduction in cecal intubation time among junior faculty, although statistical significance was not reached with this effect modification (β-coefficient of the interaction term −2.63, P = .21) (Table 3).
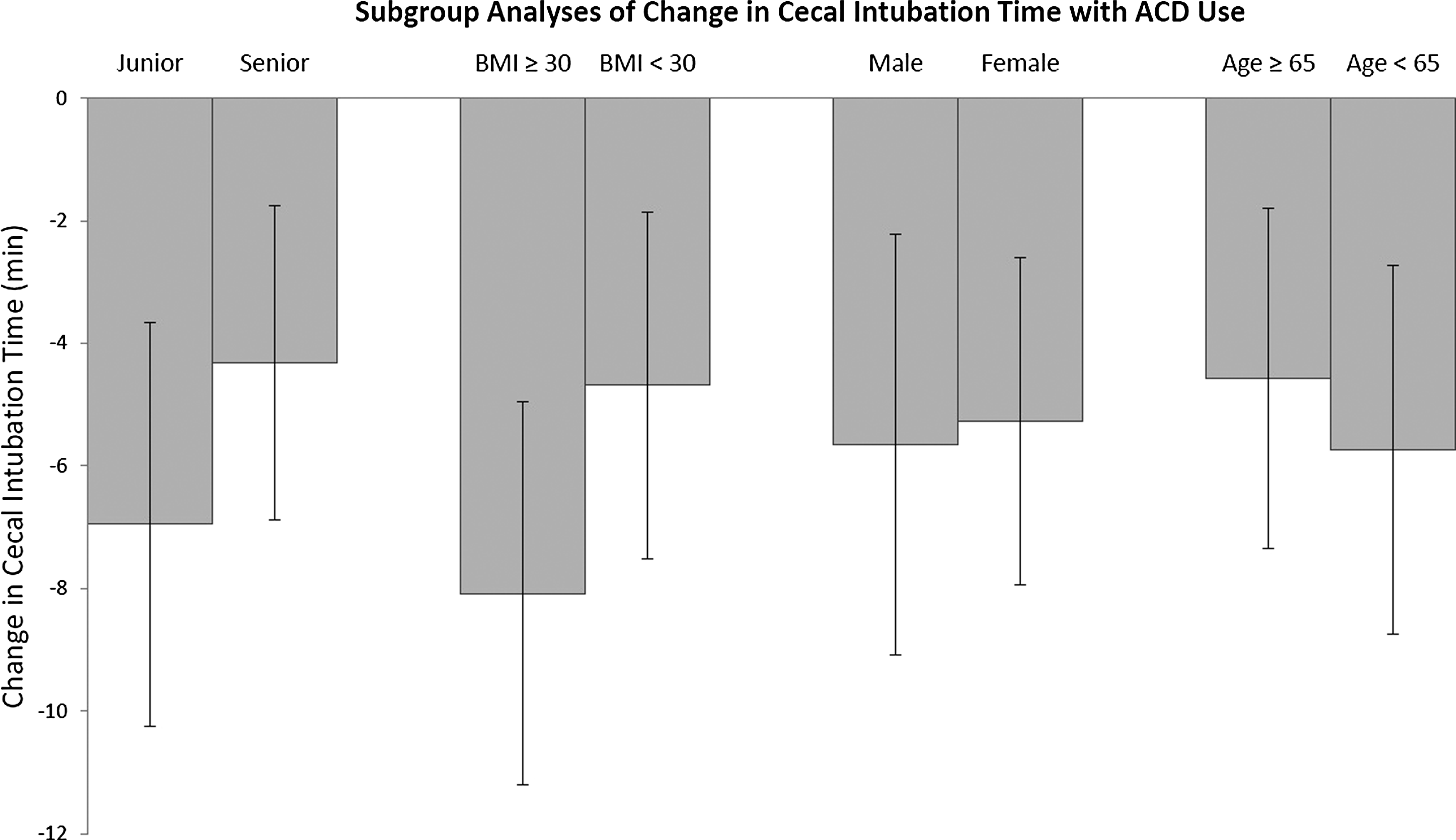
Comparison in cecal intubation time improvement with the use of ACD between junior endoscopists (<5-year experience) and senior endoscopists (>5-year experience) and between obese (BMI ≥30) and nonobese (BMI <30) patients showed a trend toward more reduction in time for colonoscope advancement among junior endoscopists and obese patients, although statistical significance was not reached. The reduction in cecal intubation time appeared to be similar between male and female patients, and between older (age ≥65) and younger (<65) patients. ACD, abdominal compression device; BMI, body mass index.
ACD use also appeared to provide more benefits for obese patients (BMI ≥30) compared to nonobese patients (BMI < 30), although statistical significance was also not reached (−8.08 ± 6.24 minutes versus −4.68 ± 5.66 minutes, P = .16). When an interaction term, including obesity and ACD use, was incorporated into the multivariate regression model, a trend toward effect modification by obesity was also noted but did not reach statistical significance (β-coefficient of the interaction term −2.32, P = .30). Subgroup analyses by age (≥65 versus < 65) and gender (male versus female) did not demonstrate meaningful differences in cecal intubation time reduction by ACD (− 4.57 ± 5.56 minutes versus −5.74 ± 6.03 minutes, P = .61 and −5.65 ± 6.87 minutes versus −5.27 ± 5.32 minutes, P = .86, respectively) (Fig. 3).
Discussion
Colonoscopy is the gold standard for detection of CRC and its precursors, and has become the most common gastrointestinal endoscopic procedure performed in the United States. Despite its widespread use, failure to reach the cecum frequently occurs from persistent looping of the colonoscope, leading to abdominal discomfort and increasing the risk of complications.3–6,10
The application of external abdominal pressure has been widely used as common practice during colonoscopies, with reported incidence ranging from 12% to 82% in the literature.11–13 This is predominantly performed by nursing staff and has been demonstrated to reduce loop formation in the sigmoid and transverse colon, thereby decreasing patient pain and improving rates of successful cecal intubation.
However, traditional manual abdominal pressure is manually intensive, often predisposing to musculoskeletal injuries of the neck, back, and upper extremities. The Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire, a validated tool to assess work-related injury, has been used in a variety of studies to investigate the incidence of injury among endoscopy nurses.9,14 The questionnaire is scored from 1 to 100, with a mean DASH score for work-related disability of 8.8. 15 Studies to date have consistently found that endoscopy nurses have increased DASH scores, with averages reported to be as high as 21.5.9,14 Furthermore, studies have shown that almost half of the endoscopy nurses have reported using analgesics for upper extremity pain, 60% reported seeing a physician for upper extremity symptoms, and 33% noted missing work because of upper extremity discomfort. Significantly higher DASH scores (i.e., increased injury) are found among those nurses who sought physician consultation, regularly used analgesics, and missed work. 9 Working full-time has also been shown to be a significant predictor of increased injury. 14
Musculoskeletal injuries in the workplace not only cause pain and suffering to the employee but also affect the employee financially through lost wages. Furthermore, these injuries disadvantage employers through paid sick days, lost productivity, and increased healthcare and workers' compensation costs. 16
Alternative techniques to provide abdominal pressure have been investigated. For example, Catalano et al. developed an external straightener device that enabled compression of the abdomen during colonoscopy. This apparatus was successful at reducing cecal intubation and decreasing the pain reported by patients undergoing the procedure, however, the device itself was costly. 7 Tsutsumi et al. evaluated the usefulness of an abdominal bandage to keep the colonoscope straight in the sigmoid colon and prevent looping throughout the examination. This device similarly led to improvement in cecal intubation time and reported pain, but the bandage required a maneuver to wrap it many times around the abdomen and may not be a feasible option for all providers and patients. 8 More recently, Toros et al. developed a fitted abdominal corset to exert pressure for preventing stretch of the mesentery and formation of sigmoid looping. 17 While this apparatus was effective, inexpensive, and easy to obtain, it has only been investigated in patients of low BMI since its design requires encircling of the abdomen. Moreover, the use of a corset may not be practical for patients who are obese.
Despite the effectiveness of each of the aforementioned devices, none has been widely used due to cost or feasibility. Applicability has also been limited, particularly in the obese population, given the requirement of several of these devices to be fitted or wrapped around a patient's abdomen.
This study investigated the N-Doe Pillow, a novel, hands-free ACD that is easy to use and practical in all patients. We found that use of this device independently decreased cecal intubation time in a prospective, single-blinded, matched-controlled pilot study. While this study focused on cecal intubation time, use of this ACD may have implications for other important outcomes such as sedation requirements, risk of sedation-related complications, patient scheduling, endoscopy room staffing, and physician and technical reimbursement.
Several factors have been associated with a higher risk of incomplete colonoscopy or more difficult cecal intubation, and may aid in identifying specific subgroups that may benefit from the assistance of this device. Female gender is the most frequently reported predictive factor,18–22 although patients with advanced age,18,21–23 low BMI, 20 history of hysterectomy, 19 or diverticular disease 22 have also been shown to lead to more difficult and incomplete colonoscopies. In our study, the ACD group demonstrated a significantly shorter cecal intubation time compared to the control group. The benefits of this ACD do not appear to be limited to these specific patient subpopulations in whom completion of colonoscopy may be less predictable, as subgroup analyses did not reveal significant differences in the effect of ACD by age or gender.
One of the most important factors affecting the success of colonoscopy is the technical skill of the endoscopist. A higher level of experience has been demonstrated to be significantly predictive of cecal intubation rates.24,25 In addition, a lower endoscopist annual case volume has been reported to be associated with a higher risk of incomplete colonoscopy.21,24–26 The completion rate for junior endoscopists (< 5 years of experience) with a higher procedure volume per year has been demonstrated to be higher than for those with a lower procedure volume per year.24–26 In our study, there was a trend toward more significant reduction in cecal intubation time among less-experienced junior faculty, suggesting this device may have particular applicability in the trainee and/or early career endoscopists, or in surgeons who perform endoscopy and for whom case volumes tend to be lower.
There is great need for an inexpensive and easily manipulated device that provides abdominal pressure, is effective at improving the quality of colonoscopy, and practical for use in all patients. The N-Doe Pillow may have the potential to fulfill this role. This device is affordable and reusable. It is easily positioned under the patient before the colonoscopy, providing constant pressure throughout the procedure in a standard manner. It takes advantage of the individual's own body weight, avoiding traditional manual abdominal pressure applied by nursing staff, which is imprecise and manually intensive, often leading to musculoskeletal injuries. As the amount of pressure exerted by the ACD depends on the patient's own body weight, it is also not surprising that a trend toward more significant reduction in cecal intubation time among patients with higher BMI was observed. Furthermore, unlike other ACDs, this device does not require wrapping or bandaging of the abdomen, which can often be timely and of limited feasibility in people of high BMI.
The strengths of this study include that it was prospectively performed and single blinded. Furthermore, patient selection was matched by age, gender, endoscopist, procedure location, indication, bowel preparation quality, and history of abdominal surgery, thereby minimizing important factors known to affect the success of colonoscopy completion. In addition, we were able to perform multivariate analysis to further control for these confounders. Consistent with previous literature, endoscopist experience and abdominal surgery were also found to be significantly associated with cecal intubation time, further validating our cohort.
The limitations of this study include the small sample size and the fact that it was not a randomized controlled trial. In addition, it was only performed at a single academic center, where case volume and endoscopist skill level may not be representative of the broader population. Furthermore, it excluded patients with prior colonic resection and those identified as needing anesthesia support, possibly selecting for a healthier population of patients.
In summary, this work represents a prospective, single-blinded, matched-cohort study of adult patients investigating the use of a novel, hands-free ACD, with an objective outcome (i.e., cecal intubation time). Our results demonstrate that the mean cecal intubation time was significantly reduced in the ACD group compared to controls, even after controlling for potential confounders. Further randomized controlled trials are needed to verify the beneficial effects of this device on colonoscopy outcomes, and also potentially aid in identifying specific patient subpopulations that might benefit more from the ACD.
Footnotes
Acknowledgments
We would like to acknowledge the Brigham and Women's Hospital Endoscopy unit nurses and staff for their assistance in completing this study.
Disclosure Statement
Drs. A.R.S. and W.W.C. have no conflict of interest or financial ties to disclose. Dr. M.R. has an equity interest in GI Windows and is a consultant to Medtronic.