
Abstract
Abstract
Background:
The safety and oncologic completeness of video-assisted lateral neck dissection (VALND) for papillary thyroid carcinoma (PTC) with lateral neck lymph node metastasis (LNM) have been reported. However, their generalization has remained limited because the advantages and drawbacks are not well demonstrated.
Materials and Methods:
A total of 64 patients with PTC and unilateral lateral neck LNM who underwent total thyroidectomy with central compartment neck dissection and lateral neck dissection (LND) were prospectively enrolled. They were randomly assigned to the video-assisted (VA) group (n = 32) or open group (n = 32) and were treated either by VALND or conventional open LND, respectively. We compared operating time, complications, oncologic completeness, postoperative pain, and cosmetic results between the two groups.
Results:
The complication rate and oncologic completeness, including the results of radioactive iodine scans, mean number of lymph nodes retrieved, and mean postoperative serum thyroglobulin levels, were similar between the groups. Postoperative pain was observed less frequently after surgery in the VA group (P < .0001). Cosmetic results evaluated by a verbal response scale and a numeric rating scale were in favor of the VA group (P < .0001 and P = .0004, respectively). Total operating time was 176 ± 16 minutes in the VA group and 161 ± 16 minutes in the open group (P = .0003).
Conclusions:
VALND yielded complication and oncologic completeness rates that were similar to those of open LND. However, VALND resulted in less postoperative pain and better cosmetic results.
Introduction
S
Materials and Methods
Patients
Between April 2014 and November 2015, 64 consecutive consenting patients with PTC and unilateral lateral neck LNM who underwent total thyroidectomy (TT) with central compartment neck dissection (CCND) and LND at the Head and Neck Surgery Department in Sir Run Run Shaw Hospital, Institute of Micro-Invasive Surgery, Zhejiang University, were prospectively enrolled. All subjects who had lateral lymph nodes with a suspicious appearance on ultrasonography underwent ultrasound-guided fine-needle aspiration cytology examination. An enhanced computed tomography scan of the neck was also performed to estimate the extent of invasion of the primary tumor and the status of the neck LNM. All enrolled patients met strict eligibility criteria. The inclusion criteria were as follows: (1) a primary tumor size ≤4.0 cm and (2) a largest metastatic lymph node diameter ≤3.0 cm. The exclusion criteria were as follows: (1) a history of neck surgery or irradiation, (2) metastatic lymph nodes at level I or Va, (3) a suspicious primary tumor or invasion of metastatic lymph nodes to adjacent structures, such as the trachea, esophagus, or internal jugular vein (IJN), and (4) distant metastases. The patients were randomly allotted to the VALND approach (video-assisted [VA] group) or the open LND approach (open group). Randomization was performed via a computer-generated randomization chart immediately before surgery. The patients were not blinded to the surgical procedure and equally divided into the VA group or the open group. The study protocol was approved by our institutional review board and informed consent was obtained from all study participants.
Surgical procedure
Briefly, under general tracheal intubation anesthesia, the patient was placed in supine position with the anterior neck slightly extended by a roll beneath the shoulders and a donut placed under the occiput to stabilize and support the head.
VALND procedure
A 4–5 cm symmetrical anterior neck incision was made along the natural skin fold (one fingerbreadth above the sternal notch) and the skin incision margin was then covered and protected by several small dressing strips. The TT and CCND were accomplished by a conventional procedure. After TT and CCND, the patient's head was turned to the side opposite the lesion to expose the lateral neck compartment area, and LND was performed using the VA approach. The procedures of the VALND were similar to those reported previously,6–8 but with some modifications. A 10-mm 30° endoscope was used for vision. Three long retractors were used to maintain a wide working space for our approach (Fig. 1). To prevent raising too large or too small a flap under endoscopic vision, the anatomic landmarks, such as the mandibular angle, hyoid bone, anterior border of the sternocleidomastoid muscle (SCM), and cervical midline, were labeled on the skin. Limited skin flaps were attached to the hyoid bone superiorly, the anterior edge of the SCM laterally, the cervical midline medially, and the superior edge of the clavicle inferiorly. A self-developed working space creator consisting of one long retractor fitted with a suction apparatus (Hangzhou Good Grams Photoelectric Instrument Co. Ltd.) was used to maintain a wide, stable, and tent-like working space for the LND. This system can mechanically elevate the upper skin flap and keep the working space stable for a prolonged period. The steam or smoke generated by the harmonic scalpel (Ethicon Endo-Surgery, Cincinnati, OH) or electrosurgical knife was cleared immediately using the continuous negative pressure suction apparatus connected to the long retractor. The medial border of the SCM was dissected up to the posterior belly of the digastric muscle and retracted with another long retractor; one other retractor was used to retract inward and could be applied as needed, depending on the dissection location (Fig. 2). Then, the omohyoid muscle was exposed and dissected to the level of the hyoid bone, the submandibular gland was retracted superiorly with a long retractor, and the posterior belly of the digastric muscle was exposed and dissected. The carotid sheath was opened, the IJN was retracted medially with a long retractor, the vagus nerve was exposed, and the lymph nodes and surrounding fibroadipose tissue were dissected downward. The spinal accessory nerve (SAN), cervical plexus nerve, phrenic nerve, brachial nerve, and transverse cervical artery were exposed and preserved (Fig. 3). The thoracic duct on the left side or the lymphatic duct on the right side could be identified and spared in some cases due to the endoscopic magnification and were ligated safely when necessary. The lateral neck lymph nodes and fibroadipose tissue (sublevels II, III, IV, and Vb) were resected en bloc (Fig. 4).

Three long retractors were used to maintain a wide working space for our modified video-assisted lateral neck dissection.

The self-developed working space creating system was used to create the operative space. R, retractor; S, suction apparatus; W, working space creator.
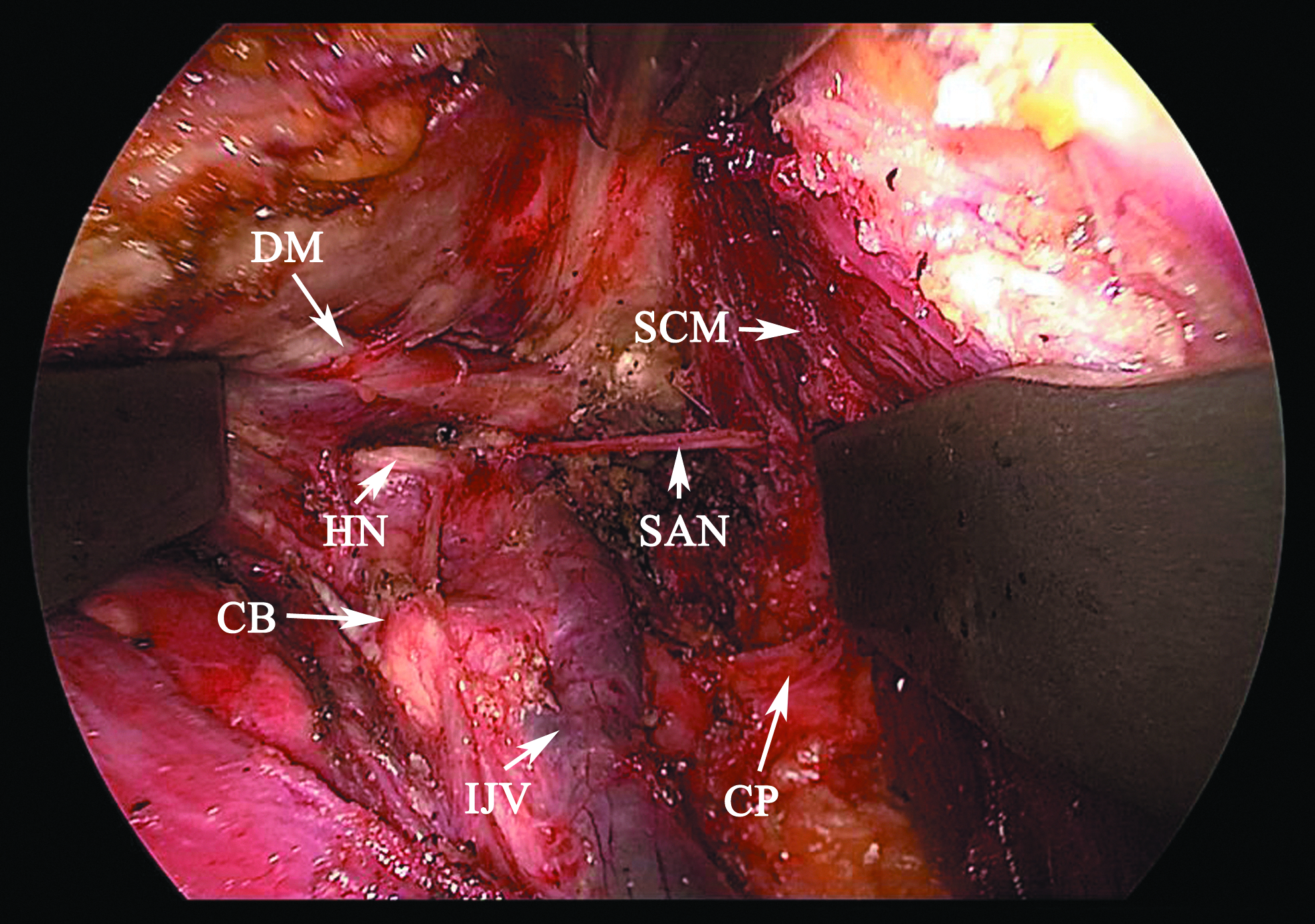
The surgical field after video-assisted lateral neck dissection and the working space were maintained by three long retractors. CB, carotid bifurcation; CP, cervical plexus; DM, digastric muscle; HN, hypoglossal nerve; IJV, internal jugular vein; SAN, spinal accessory nerve; SCM, sternocleidomastoid muscle.

The operative incision (4-cm length) after video-assisted lateral neck dissection and the lateral neck lymph nodes (sublevels II, III, IV, and Vb) were resected en bloc.
Open LND procedure
A 9–12 cm asymmetrical, extended, inferior, cervical collar incision was made along the natural skin fold about one fingerbreadth above the sternal notch. The skin flap was applied to the hyoid bone superiorly, the superior edge of the clavicle inferiorly, the cervical midline medially, and the anterior edge of the trapezius posteriorly. After TT and CCND, the patient's head was turned to the opposite side of the lesion to better expose the lateral neck area. Then, the carotid sheath was opened, the IJN and vagus nerve were exposed, and the lymph nodes and surrounding fibroadipose tissue were dissected downward. The SAN, cervical plexus nerve, phrenic nerve, brachial nerve, and transverse cervical artery were exposed and preserved. The lateral neck lymph nodes (sublevels II, III, IV, and Vb) were resected en bloc.
All patients underwent 100 mCi radioactive iodine (RAI) ablation 2–4 months after surgery. Before administration of 131-I, blood was drawn to measure serum thyroglobulin (sTg) and thyroglobulin antibody levels. A 24-hour neck and whole body 131-I uptake scan was performed in each patient while off levothyroxine therapy. All patients received suppressive levothyroxine during follow-up. The sTg and thyroglobulin antibody levels were measured every 6 months postoperatively. Neck ultrasound was performed to assess the thyroid bed and lateral neck compartment every 6 months during follow-up after surgery. Direct or indirect laryngoscopy was performed preoperatively and postoperatively to assess vocal cord function. Permanent recurrent laryngeal nerve palsy was defined as vocal cord fixation at 6 months after surgery. All patients were followed up for at least 1 year after surgery. We defined hypoparathyroidism as the condition in which the serum calcium levels were below 1.9 mmol/L on the first day after surgery and permanent hypoparathyroidism as the need for calcium and/or vitamin D supplements at 6 months after surgery.
Postoperative pain was scored using a visual analog scale (VAS) consisting of a 100 mm line anchored by “0 = no pain” at one end and “100 = worst pain imaginable” at the other. 11 No analgesic medication was given postoperatively in either group, and all patients were asked to rate their pain 24 and 48 hours after surgery by pointing to the level indicating its severity on the 100 mm line. Cosmetic outcome score was evaluated on a numeric rating scale and a verbal response scale. 11 The numeric rating scale ranged from 0 to 10, with a higher score indicating a better cosmetic result. The verbal response scale comprised four options (1 = poor; 2 = acceptable; 3 = good; 4 = excellent). All patients were asked to evaluate the cosmetic appearance of the cutaneous scar on the neck at 1 year after surgery.
The data from the two groups were analyzed and compared, and the results are expressed as mean ± standard deviation. Statistical analysis was performed using Statistical Analysis System version 9.0 software (SAS, Inc., Cary, NC) with the chi-squared test, Fisher's exact test, the Student's t-test, or Wilcoxon two-sample test as appropriate. Statistical significance was defined at P < .05.
Results
The clinicopathologic characteristics of the two groups are summarized in Table 1. The VA group included 32 patients (22 women, 10 men) of mean age 39.7 ± 12.0 (range 16–63) years. The open group included 32 patients (26 women, 6 men) of mean age 41.2 ± 9.7 (range 24–64) years. The two groups were similar in terms of age, sex ratio, tumor size, and extrathyroid tumor extension. The mean numbers of retrieved and positive retrieved total, central, and lateral lymph nodes were similar in the two groups. The mean operating time was 176 ± 16 minutes in the VA group and 161 ± 16 minutes in the open group (P = .0003), but the duration of postoperative hospital stay was similar between the two groups.
According to the seventh edition of American Joint Committee on Cancer staging criteria.
VA, video-assisted; SD, standard deviation; LND, lateral neck dissection; LN, lymph nodes; TNM, tumor, node, metastasis.
The 32 patients in the VA group successfully underwent a VA procedure and none needed conversion to an open procedure. In the open group, a superior neck transverse incision was made in 1 patient to expose the level II area better as the patient had a long neck.
The complication rates were similar between the two groups (Table 2). No cases of permanent hypocalcemia were observed in either group. One case of permanent recurrent laryngeal nerve palsy occurred in the open group. One case of transient SAN injury occurred in the open group and 1 transient sympathetic nerve injury was observed in the VA group. Three cases of minor chyle leaks (1 case in the VA group and 2 cases in the open group) were observed, and these successfully responded to conservative treatment. No major chyle leak was observed in either group.
VA, video-assisted.
At the time of thyroid remnant ablation, all patients had a thyroid stimulating hormone level >30 μm/mL. Mean 131-I uptake was 0.4% ± 0.5% (range 0.1%–2.6%) in the VA group and 0.7% ± 0.9% (range 0.1%–3.4%) in the open group (P = .3951). The 24-hour 131-I uptake ≤1% in the thyroid bed was observed in 29 (90.6%) cases in the VA group and 26 (81.3%) cases in the open group (P = .4741). Mean sTg levels off levothyroxine were 2.06 ± 4.63 (range 0.02–24.7) ng/mL in the VA group and 2.45 ± 4.52 (range 0.03–21.19) ng/mL in the open group before RAI ablation (P = .7204). No patients showed any uptake of 131-I outside the thyroid bed as assessed by whole-body scans performed after administration of 100 mCi of 131-I. The mean sTg levels on levothyroxine were 0.12 ± 0.40 (range 0–2.25) ng/mL in the VA group and 0.10 ± 0.35 (range 0–1.96 ng/mL) in the open group 1 year after surgery (P = .2735). One patient had a serum Tg >1 ng/mL in the VA group and the open group, respectively. Neck ultrasound showed no tumor recurrence or residual disease in either group during follow-up (Table 3).
VA, video-assisted; sTg, serum thyroglobulin; RAI, radioactive iodine; LT4, levothyroxine.
Postoperative pain was significantly less severe in the VA group than in the open group as assessed by VAS at 24 and 48 hours after surgery (P < .0001). Cosmetic results were significantly better in the VA group than in the open group as evaluated by both the verbal response scale and the numeric rating scale 1 year after surgery (P < .0001 and P = .0004, respectively) (Table 4).
VA, video-assisted; VAS, visual analog scale.
Discussion
In recent years, several VALND approaches for PTC with lateral neck LNM have been described by many centers.5–8 However, we have experienced some drawbacks to the reported VALND techniques. In previously described VALND techniques, the working space was maintained by one or two retractors managed by an assistant, and the working space was small and unstable, making the VALND (especially level II) difficult and unsafe. Meanwhile, the steam or smoke generated by the energy instrument, such as a harmonic scalpel or electrosurgical knife, cannot be cleared immediately during the operation, which obscures the surgical field, also making the VALND procedure unsafe, in addition to prolonging the operative time. Therefore, we modified the VALND procedure in two ways. The first modification was in the technique used to create working space. In our modified VALND, three long retractors were used to create and maintain the surgical working space. Instead of having an assistant apply manual retraction to create the working space, one long retractor was connected to a self-developed working space creator that can mechanically elevate the upper skin flap and keep the working space stable for a prolonged period. Another long retractor was used to retract the SCM outward, and one other long retractor was used to retract inward, and could be repositioned as needed, depending on the dissection location. Therefore, the modified VALND procedure could be performed easily in a relative large and stable surgical working space. The second modification is the use of a continuous negative pressure suction device that was attached to the long retractor to remove the steam or smoke that was generated by the energy instrument, which ensures a clearly visible surgical field, makes the procedure safer, and decreases the operative time. These modifications make our modified VALND easier and safer than previously reported VALND procedures.
When mentioned to the oncologic completeness of the VALND, some authors reported that it seems to be comparable to the conventional open procedure if selection criteria are careful followed as given in Ref. 7 With the improvement of surgical instruments and endoscopic techniques, our considerable experience with VALND convinces us that a compartment-oriented anatomical dissection could be performed and a complete lateral neck lymph node dissection in accord with oncologic principles is possible. 10 In an earlier retrospective and comparative study, we demonstrated that oncologic completeness, including a number of retrieved lymph nodes and follow-up sTg (on levothyroxine) levels, was similar between VALND and open LND. 9 In the present study, we additionally performed thyroid bed 24-hour 131-I uptake and sTg measurement (off levothyroxine) before RAI ablation as a reliable predictor of the extent of thyroid and/or tumor residue. 12 Miccoli et al. have concluded that the MIVAT achieved similar completeness compared with conventional open total or near-TT in terms of the 131-I uptake and sTg measurement (off levothyroxine) before RAI ablation.4,13 The results obtained in this study showed no significant difference both in terms of thyroid bed 131-I uptake and circulating sTg (on and off levothyroxine) levels between the two groups. The average 24-hour 131-I uptake and the 24-hour 131-I uptake ≤1% in the thyroid bed were similar between the two groups. And the negative result by the whole-body 131-I uptake scan revealed no locoregional or distant metastasis of all the patients in the two groups. Mean values of sTg found in this study were low in both groups of patients. Although 2 patients (1 in the VA group and 1 in the open group) had a serum Tg >1 ng/mL at 1 year after surgery, neck ultrasound showed no evidence of residual tumor or recurrence in either group. Meanwhile, the number of retrieved lymph nodes was similar between the two groups. In conclusion, our results showed that no significant difference in 131-I uptake, sTg levels (on and off levothyroxine), or number of retrieved lymph nodes was observed between the VA group and the open group. These evidences demonstrated that there was similar oncologic completeness of surgical resection between the two surgical procedures.
Postoperative pain was scored on a VAS at 24 and 48 hours after surgery, and less pain was documented for VALND; the difference between the two groups was statistically significant at both assessment times (P < .0001). It is probable that the smaller skin incision plays a role in alleviating pain; moreover, the less raised subcutaneous flap of the VALND could also have this effect because of less subcutaneous edema and a smaller inflammatory reaction. Meanwhile, compared with open LND, less retraction was needed for exposure in VALND due to the endoscopic magnification. However, patients' feeling after surgery also had bias from their self-evaluation of smaller incision in the VA group because it is a subjective measurement.
In terms of the cosmetic result, it seems reasonable that a 4–5 cm symmetrical scar is superior to an asymmetrical 9–12 cm incision scar. In our study, we evaluated the cosmetic result on a verbal response scale and a numeric scale, and both favored the VA approach (P < .0001 and P = .0004, respectively).
The level II area locates deeply in the neck and there are several vital nerves and vessels in this area, which makes dissection of level II (especially level IIb) difficult and unsafe especially when the patient's neck is long and/or wide through the extended collar incision in the inferior neck. For conventional open LND, a wider incision is required to facilitate the identification of the SAN, carotid sheath, superior thyroid artery, and the branches of the IJN. Due to the magnification provided by the endoscope, the SAN and vessels could be exposed more clearly, permitting the careful dissection and safe preservation of those structures and making the level II dissection safer and easier. In this study, a superior neck transverse incision was made in 1 patient in the open group to expose the level II area better because of the patient's long neck.
The limitations of VALND are its longer operating time and higher cost. Although the time for surgery by VALND was longer than for the open approach in this study, improvement in surgical proficiency can lead to a decrease in the duration of surgery by VALND, making it comparable to the open approach. In our study, the mean operating time in the VA group was longer by about only 15 minutes when compared with the open group. Because a harmonic scalpel is used routinely in both approaches, no extra surgical instrumentation is needed for VALND. Therefore, there is no great increase in the overall costs if VALND is performed.
Although a study that includes a larger series of patients with longer follow-up is needed before deciding the advantages and oncologic completeness of VALND, we can conclude that this approach is safe and effective, and offers some advantages in selected patients with PTC and lateral neck LNM.
Footnotes
Disclosure Statement
No competing financial interests exist.