
Abstract
Abstract
Background:
Denver® shunts have traditionally been used for palliation of refractory malignant and chylous peritoneal and pleural collections. We describe an innovative use of the Denver shunt in a child with generalized lymphatic anomaly.
Materials and Methods:
Retrospective chart review of a 6-year-old girl with generalized lymphatic anomaly, who presented with refractory lymphorrhea from the labium majus, was performed. This was managed with innovative placement of the Denver shunt between a large abdominal wall cyst and the peritoneal cavity.
Results:
There was progressive reduction in lymphorrhea with complete cessation at 11 months post shunt placement. At 33-month follow-up, the shunt remains patent with no further lymphorrhea.
Conclusion:
Denver shunts can be utilized for the creation of internal drainage pathways besides its traditional uses for draining peritoneal and pleural fluids.
Introduction
D
Case Report
A 6-year-old girl presented to the vascular anomaly clinic with a 5-month history of continuous leakage of chylous fluid (lymphorrhea) from multiple cutaneous vesicles over an enlarged deformed left labium majus associated with lower abdominal and back swelling (Fig. 1). Imaging, including skeletal survey and whole body magnetic resonance imaging (MRI), revealed multiple lytic lesions involving the axial and appendicular skeleton, and ultrasound (Fig. 2) and MRI abdomen (Fig. 3) showed multiple fluid-filled cysts of various sizes (1–8 cm) within the subcutaneous tissues of the abdominal wall extending into the left labium majus. Dynamic MRI lymphangiogram revealed the absence of the thoracic duct and drainage of lymph from both lower extremities into the previously demonstrated cysts in the abdominal wall serving as collateral pathways. This led to the diagnosis of generalized lymphatic anomaly and the patient was started on Sirolimus therapy. To manage the lymphorrhea, multiple external drainage catheters were placed within the abdominal wall and labial cysts by interventional radiology, followed by multiple sessions of trans-catheter sclerosant injection (doxycycline, sodium tetradecyl sulfate, and absolute alcohol). Despite aggressive sclerotherapy, the patient continued to have a total drain output of 4 L/day, severe fluid and electrolyte imbalance, anemia, hypoalbuminemia, and low Immunoglobulin G (IgG), requiring inpatient management. A multidisciplinary team discussion proposed internal drainage as a solution to management of lymphorrhea alongside medical management with daily oral Sirolimus, weekly intravenous injections of pegylated Interferon alpha 2b, and 6 monthly intravenous injections of Zoledronic acid. A Denver shunt was utilized to create this internal drainage pathway 3 months after initial presentation.

A six-year-old girl presenting with diffuse abdominal and lower back swelling

Axial ultrasound image of the left flank shows multiple subcutaneous lymphatic cysts ranging from 1 to 8 cm. Note the internal echoes due to the chylous content of these cysts.
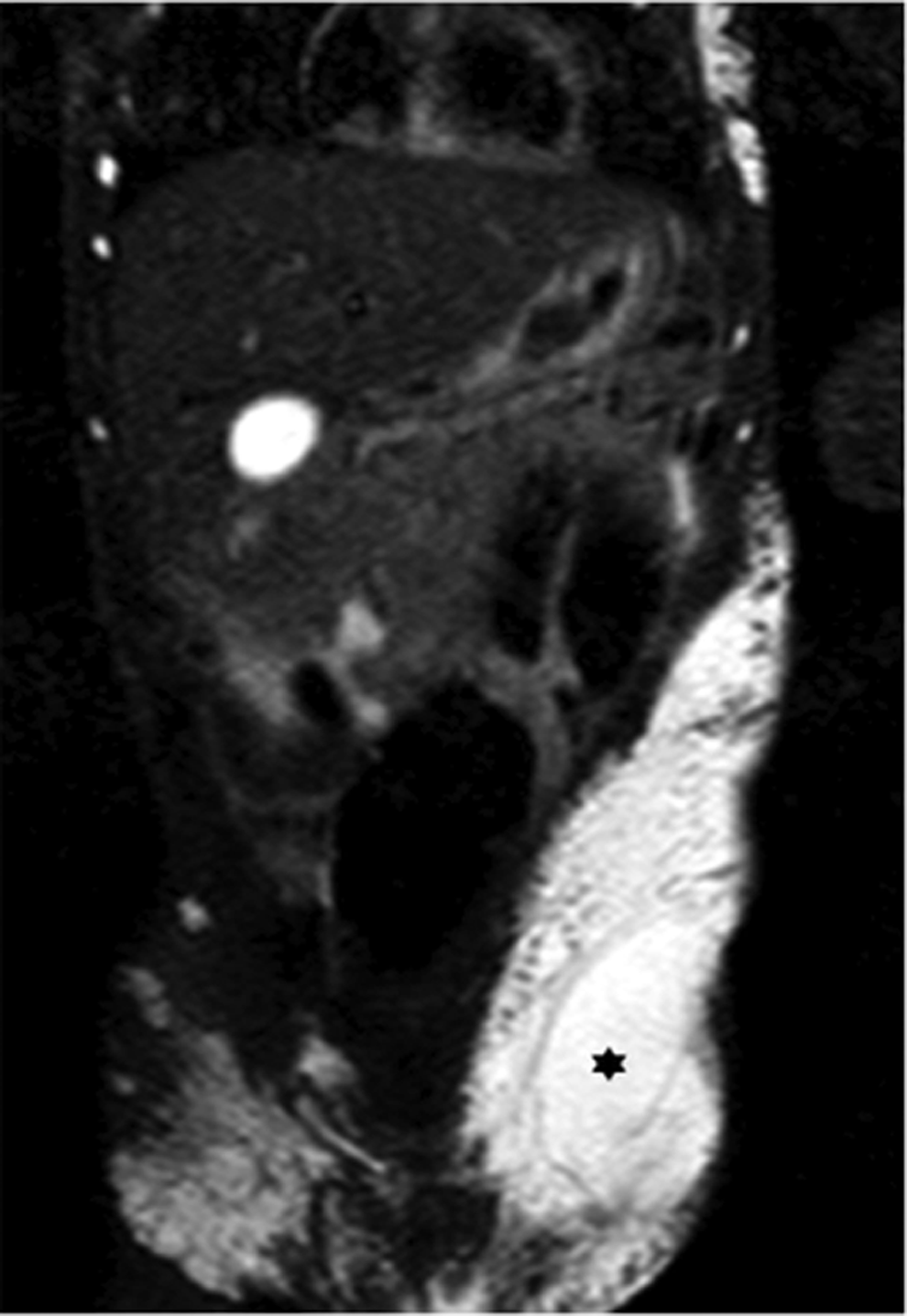
Coronal T2-weighted MRI of the anterior abdomen shows large areas of bright signal within the subcutaneous tissues of bilateral flanks and the left abdomen similar to the fluid-filled cysts seen on ultrasound. The largest cyst (black asterix) measuring 8 × 4 cm in the left flank was utilized for placement of the inflow catheter of the Denver® shunt.
Technique
The child was anesthetized in a supine position and the abdomen was painted and draped. The three components of the Denver shunt (CareFusion Corporation, San Diego, CA), that is, a multiside hole 15.5F inflow catheter, a double-valved shunt chamber, and an 11F end-hole outflow catheter, were placed as illustrated in Figures 4 and 5. An incision was made in the scar of the umbilicus and a 5-mm Step trocar (Medtronic, Minneapolis, MN) was introduced. Pneumoperitoneum was achieved with CO2 of 5 L/M and pressure of 12 mm Hg. The peritoneal cavity was inspected using a 5-mm 30° telescope, which showed no intestinal adhesions.
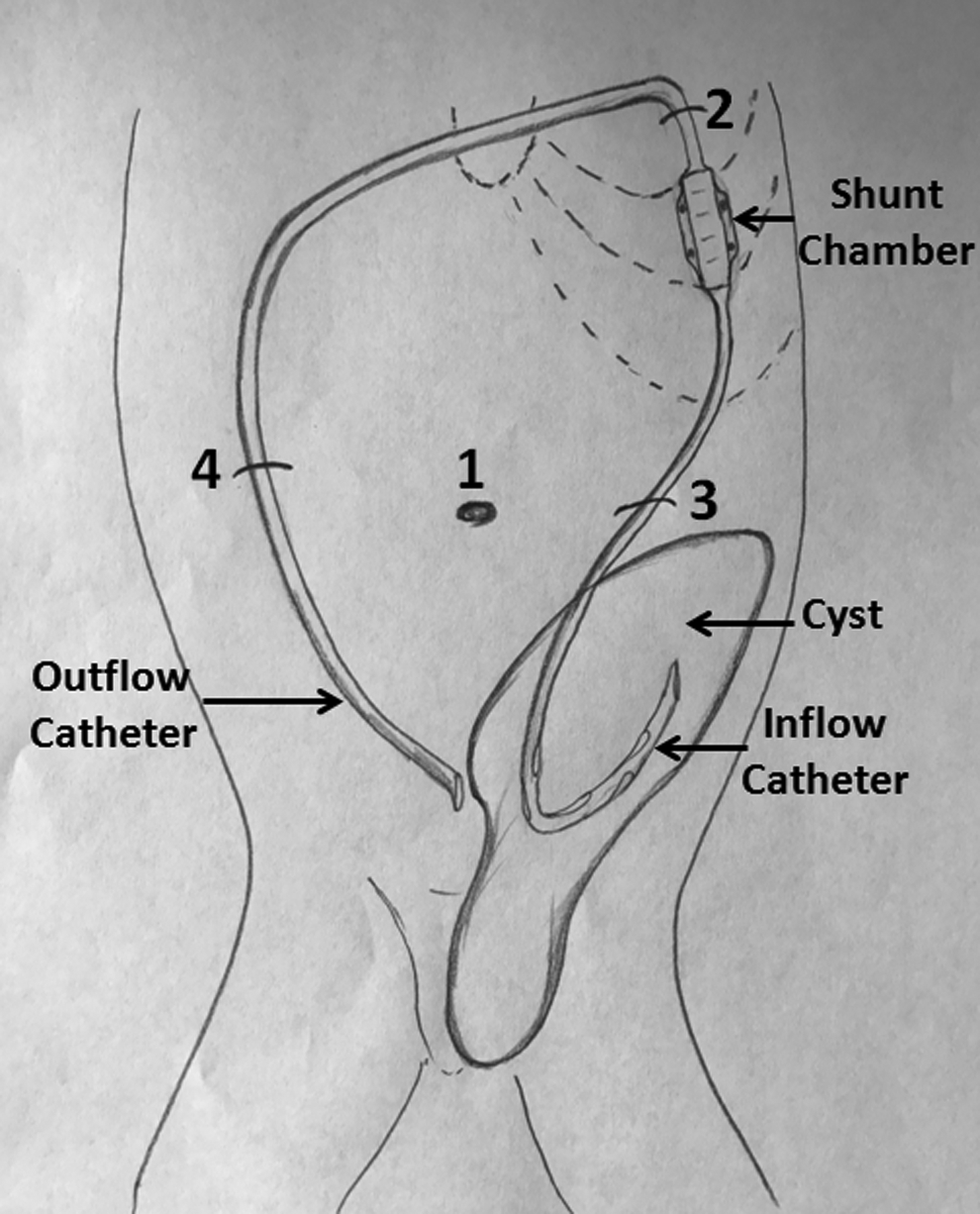
Diagrammatic representation of the Denver shunt placement technique. A 5-mm 30° telescope was introduced through incision 1 (umbilical) after creation of pneumoperitoneum. The shunt chamber was placed in a subcutaneous pocket created below incision 2. The inflow catheter (15.5F) was tunneled subcutaneously from this pocket to incision 3 and inserted into the left flank abdominal wall lymphatic cyst using the Seldinger technique. The outflow catheter (11F) was tunneled subcutaneously from incision 2 to incision 4 and inserted into the peritoneal cavity using the Seldinger technique.

Clinical photograph immediately after insertion of Denver shunt. Note the inflow catheter in the left flank (black arrow), the shunt chamber (black asterisk), and the entry point of the outflow catheter (white arrow). The interventional radiology drain sites were closed with glue.
A subcutaneous pocket was fashioned for placement of the shunt chamber using a 1.5-cm transverse incision and blunt dissection over the left lower chest wall. Abdominal ultrasound was used to plan a 1.5-cm transverse incision in the left flank adjacent to the largest subcutaneous cyst (8 × 4 cm). The inflow catheter was tunneled from the shunt chamber pocket downward into the left flank incision. The subcutaneous cyst was accessed under ultrasound guidance using the Seldinger technique, a 16F peel-away sheath was placed and the inflow catheter was advanced into the cyst through the peel-away sheath.
Next, the entry site of the outflow catheter was created using a 1.5-cm transverse incision within the right flank, which was free of subcutaneous cysts. The outflow catheter was tunneled from the left chest wall incision to the right flank incision. An 18G needle was introduced through the right flank incision and advanced inferomedially into the peritoneal cavity through a subperitoneal tunnel under laparoscopic guidance. A 12F peel-away sheath was then placed using the Seldinger technique through which the outflow catheter was positioned in the peritoneal cavity. Free flow of fluid was established from the left flank lymphatic cyst into the peritoneal cavity. The laparoscopy port was withdrawn after desufflation of the peritoneal cavity. All incision sites were closed with sutures and glue.
Results
Following placement of the Denver shunt, the fluid and electrolyte imbalance improved rapidly and the patient was discharged home 9 days after shunt placement. The child resumed normal daily activities and schooling. Minor complications in the early postoperative period such as leakage from interventional radiology external drain sites and laparoscopy incision sites were managed with suture and glue application. There was normalization of serum albumin and IgG levels at 7 months and progressive reduction in leakage of fluid from the labia with complete cessation at 11 months post shunt placement. At 33-month follow-up, the shunt remains patent and functional with no further leakage from the labia and completely decompressed abdominal wall cysts (Fig. 6). The patient is on regular outpatient medical management.

Clinical photograph at 33-month follow-up shows complete decompression of the abdominal and left labium majus cysts and cessation of lymphorrhea.
Discussion
Denver shunts have been used in the management of refractory ascites and pleural effusions in adults.1,2 There are very few reports in the pediatric literature. The largest series reported so far is by Rahman et al. 3 The authors describe placement of peritoneovenous shunts in 22 children (1 month to 12 years) most of whom had refractory ascites post abdominal surgery. Shunt blockage, pulmonary edema, shunt infection, and wound leakage were the complications reported in this series. The Denver shunt has also been used to create pleuroperitoneal drainage in children with chylous pleural fluid. 4
The patient in the present study had multiple dilated subcutaneous lymphatic cysts within the abdominal wall causing abdominal distention and lymphorrhea. In the absence of the thoracic duct, these channels served as a collateral pathway for lymphatic drainage. This was a difficult case scenario with no well-established management pathway. External drainage was attempted, but produced excessive fluid and protein losses and sclerotherapy failed to obliterate the cysts. The child required daily fluid and electrolyte replacement, albumin, and IgG replacement and could not be discharged from the hospital. In addition, despite administration of antibiotics, the continued lymphorrhea posed a risk of sepsis. Innovative use of the Denver shunt in this challenging clinical situation facilitated cessation of fluid losses and facilitated discharge. It also helped to provide temporary benefit until Sirolimus could have an effect on lymphatic fluid production.
Conclusion
Denver shunts can be utilized for creation of internal drainage pathways besides their traditional uses for draining peritoneal and pleural fluid. Innovative use of Denver shunt could provide symptom relief in a patient with generalized lymphatic anomaly. Minor complications in the early postoperative period such as leakage from interventional radiology drain sites and laparoscopy incision sites are easily managed.
Footnotes
Disclosure Statement
No competing financial interests exist.